 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 13(2); 2021 > Article
- Original Article Clinical Significance of Malnutrition Risk in Severe Trauma Patients: A Single-Center Study
-
Hohyun Kim, M.D.1,2
 , Kum-Hee Hong, M.S.2,3, Inah Choi, M.S.2,4, Kyung-A Lee, M.S.2,5, Geun Am Song, M.D.2,6
, Kum-Hee Hong, M.S.2,3, Inah Choi, M.S.2,4, Kyung-A Lee, M.S.2,5, Geun Am Song, M.D.2,6 -
Annals of Clinical Nutrition and Metabolism 2021;13(2):68-74.
DOI: https://doi.org/10.15747/ACNM.2021.13.2.68
Published online: December 31, 2021
1Department of Trauma and Surgical Critical Care, Pusan National University Hospital, Busan, Korea
2Nutrition Support Team, Pusan National University Hospital, Busan, Korea
3Department of Nursing, Pusan National University Hospital, Busan, Korea
4Department of Pharmacy, Pusan National University Hospital, Busan, Korea
5Department of Nutrition, Pusan National University Hospital, Busan, Korea
6Department of Internal Medicine, Pusan National University Hospital, Busan, Korea
- Corresponding author: Hohyun Kim E-mail gskhh@naver.com ORCID https://orcid.org/0000-0001-9434-8654
• Received: December 5, 2021 • Revised: December 19, 2021 • Accepted: December 22, 2021
© The Korean Society of Surgical Metabolism and Nutrition and The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,761 Views
- 29 Download
Abstract
-
Purpose A suboptimal nutritional status is often observed among hospitalized patients across all medical/surgical specialties. The objective of the present study was to (1) analyze the prevalence of malnutrition in severe trauma patients and (2) evaluate the relationship between malnutrition and select clinical outcomes.
-
Materials and Methods This retrospective study was conducted between October 2015 and March 2017 at the Pusan National University Hospital Trauma Center. Of a total of 3,560 patients, 945 were enrolled in this study. Patients were checked for malnutrition using a nutrition assessment tool by the hospital nutrition support team. The parameters assessed included serum albumin, the ratio of actual body weight to ideal body weight (%), total lymphocyte count, appetite, and gastrointestinal problems. Clinical outcomes under consideration included 1) mortality, 2) length of hospitalization, and 3) length of stay in the intensive care unit (ICU).
-
Results The total prevalence of malnutrition in hospitalized trauma patients was 55.0% (n=520). Malnutrition risk was the independent prognostic factor of mortality in severe trauma patients (adjusted odds ratio [OR]=3.440; 95% confidence interval [CI]=1.401~8.447, P=0.007). Risk factors of malnutrition were age over 65 years (adjusted OR=2.393; 95% CI=1.699~3.370, P<0.001), injury severity score (adjusted OR=1.034, 95% CI=1.012~1.056, P=0.002), length of hospitalization (adjusted OR=1.104; 95% CI=1.007~1.020, P<0.001), and length of stay in the ICU (adjusted OR=1.050; 95% CI=1.029~1.072, P<0.001).
-
Conclusion Malnutrition is widespread in hospitalized patients with severe trauma and results in suboptimal clinical outcomes. Thus, patients at high risk of malnutrition should be monitored carefully during hospitalization.
INTRODUCTION
Suboptimal nutritional status is often observed among hospitalized patients across all medical specialties with prevalence rates ranging from 20% to 61%, depending on the disease [1-3]. As shown in previous studies, malnutrition often leads to prolonged hospitalization and higher complication rates [4-6].
The nutritional status at hospital admission is compounded by primary malnutrition mainly reflecting poor social-economic condition, and secondary malnutrition reflecting, usually, the impact of degenerative and chronic diseases. Trauma is assuming a leading cause of hospital admission of young people and associated to high rates of morbidity and mortality. However, there is still a paucity of information about nutritional status of severe trauma patients [7], In addition, there are few reports about the incidence of malnutrition in trauma patients.
It is therefore interesting to study the nutritional risk in trauma patients and the specific impact of this risk on in-hospital clinical course. The current study evaluated the impact of malnutrition risk on patients’ survival. We hypothesized that a positive malnutrition risk would be significantly associated with increased mortality and length of stay in patients with severe trauma.
MATERIALS AND METHODS
We retrospectively reviewed data from the medical records and included a total of 3,560 patients with severe trauma admitted to the trauma resuscitation unit at our Trauma Center between October 1, 2015 and March 31, 2017. Inclusion criteria were adult patients (≥18 years old) and injury severity score (ISS)≥16. Patients declared dead-on-arrival or transferred from a trauma resuscitation unit within 24 hours or discharged within 7 days or with unclear medical records on nutritional assessment were excluded. The final study population included 945 patients (Fig. 1). Available data included age, sex, ISS, abbreviated injury scale (AIS), Glasgow Coma Scale score (GCS), length of hospitalization, length of stay in intensive care unit (ICU), and survival status.
Nutrition assessment tool in Pusan National University Hospital nutrition support team (PNUH NST) was used to determine the prevalence of malnutrition and to divide patients into two cohorts: well or normal nourished and malnourished (including moderately malnourished or at risk of malnutrition, and severely malnourished) (Table 1). As shown in Table 1, we used five clinical measures (serum albumin, ratio of actual body weight to ideal body weight [%], total lymphocyte count, appetite, and gastrointestinal problem), and each measure was scored from 0~6 (serum albumin) or 0~3 (ratio of actual body weight to ideal body weight) or 0~2 (total lymphocyte count, appetite, and number of gastrointestinal problems). The malnutrition risk score corresponded to the total points for each item (0~15 points). Patients with positive malnutrition risk was defined as those with more than 4 points of malnutrition risk.
The primary outcomes were hospital mortality. Secondary outcomes included length of hospitalization and length of stay in ICU. Length of hospitalization was measured in days, from the day of admission to hospital to the time of release or death. Data were collected retrospectively to determine mortality and length of hospital stay.
Continuous variables (ISS, AIS, GCS, length of hospitalization) were reported as median and interquartile ranges (IQRs). Categorical variables were expressed as numbers and percentages.
The Student or Wilcoxon tests were used to compare the two cohorts’ length of hospital stay, with P<0.05 defined as the alpha value. The chi-square test (P<0.05) was used to compare mortality of the two cohorts, with the Yates correction as needed. The power of association between the variables was calculated as odds ratio (OR) with a 95% confidence interval (CI). Variables considered to be risk factors for mortality (risk of malnutrition according to nutrition assessment tool, age, ISS, AIS, GCS, sex) and length of hospital stay were analyzed using a multivariable logistic regression model. The Statistical Package for the Social Sciences (Version 20.0; IBM Corp., Armonk, NY, USA) and STATA software (Version 14.2; Stata Corp., College Station, TX, USA) were used to analyze the data.
This project received research approval from the Research Ethics Board of Pusan National University Hospital and was performed in accordance with the ethical standards set forth in the 1964 Declaration of Helsinki. Its later amendments and Informed consent is not applicable.
RESULTS
A total of 945 patients were evaluated, 78.3% of which were male. The median age was 58 (IQR=41~70), with 25.0% of patients aged over 65. The median of ISS was 24 (IQR=19~29) and median GCS was 15 (IQR=11~15). The median AIS for head and abdomen were 3 (IQR=0~4) and 0 (IQR=0~2), respectively. The median length of hospitalization and length of stay in ICU were 29 days (IQR=17~50) and 6 days (IQR=2~15), respectively. In addition, the overall mortality rate was 4.9% (n=46).
According to nutrition assessment tool in PNUH NST, 17.4% (n=164) of patients had malnutrition risk at admission. On the other hands, 46.5% (n=439) of patients had malnutrition risk at 7 days of admission and 55.0% (n=520) had positive malnutrition risk during admission. Prevalence of malnutrition risk in severe trauma patients is shown in Fig. 2.
Table 2 demonstrates the clinical characteristics of patients with severe trauma according to mortality. Overall mortality rate was 4.9%. Nutritional screening showed the positive malnutrition risk at admission, 7 days of admission, and more than 7 days of admission. Mortality was higher in patients with positive malnutrition risk than in those with negative malnutrition risk. In addition, a comparison of the survivor group and non-survivor group revealed that patients in the non-survivor group had a higher proportion of patients aged 65 or more (P<0.001), a higher ISS (P<0.001), a higher head AIS (P<0.001), a higher GCS (P<0.001), longer length of hospitalization (P<0.001), and longer length of stay in ICU (P<0.001).
In univariable analysis, factors associated with mortality of patients with severe trauma were age≥65 years, ISS, head AIS, GCS, and positive malnutrition risk (Table 3). Multivariate analysis showed that positive malnutrition risk was an independent risk factor for mortality (adjusted OR=3.440, 95% CI=1.401~8.447, P=0.007) (Table 3). Fig. 3 demonstrated one minus survival curve of patients with severe trauma according to malnutrition risk.
Factors associated with positive malnutrition risk were age≥65 years, female, ISS, abdomen AIS, and GCS. In addition, there were a significant correlation between positive malnutrition risk, longer length of hospitalization, and longer length of stay in ICU (Table 4).
Univariable and multiple logistic regression analysis for malnutrition risk are demonstrated in Table 5. Age over 65 years, ISS, length of hospitalization, and length of stay in ICU were independent indicators of positive malnutrition risk.
DISCUSSION
This study was the first to evaluate the prevalence of malnutrition risk and relationship between malnutrition risk and clinical outcomes in a large contemporary cohort of severe trauma patients in South Korea. We found that malnutrition was an independent prognostic factor of mortality in severe trauma patients.
Malnutrition in hospitalized patients is an important factor to consider, because it is associated with adverse outcomes such as prolonged hospital length of stay, increased complications, in-hospital mortality, and healthcare costs [8-10]. In severely injured patients, the relationship between nutritional status and clinical outcome is complicated by the systemic pathophysiological responses to trauma, which may affect, as well as may be affected by, the patient’s nutritional status [11-13]. The metabolic changes after trauma are distinctive and complex and make trauma patients more susceptible for developing malnutrition. Second, in these patients a vicious circle is set in motion by malnutrition, leading to further deterioration of the nutritional- and health status. Malnutrition was associated with higher morbidity, delayed mobilization both after conservative and operative treatment, higher in-hospital mortality, prolonged hospital length of stay, reoperation and readmissions [7,12,14]. Our study found patients with malnutrition risk had higher mortality rate, longer length of hospitalization, and longer length of stay in ICU. The results of our study also underline the importance of early malnutrition recognition and intervention to prevent further deterioration.
Malnutrition has been defined in various ways due to the lack of a gold standard for diagnosing malnutrition [15,16]. The prevalence of malnutrition varied widely in the selected studies and depends upon the way in which malnutrition was defined and measured. The prevalence of malnutrition ranged from 7% to 76% in trauma patients in general [12,14,17-19]. We examined the development of malnutrition during hospital stay and showed an increase in prevalence from 17.4% on admission to 46.5% in the first week of hospital admission. Our study found comparable rates of overall prevalence of malnutrition risk of patients with severe trauma (55.0%).
The detection of malnutrition in an early phase provides the clinician with the opportunity to intervene and attempt to prevent further deterioration of the nutritional status. Our study indicated that the risk of developing malnutrition risk was high in patients with age over 65 years, high ISS, long length of hospitalization, and long length of stay in ICU. The literature suggests that only a fraction of malnourished hospitalized patients receive timely nutritional support to prevent nutritional status decline [20]. Improved training of medical staff in recognizing and treating malnutrition is needed to create more awareness for the underestimated problem of malnutrition. Especially, elderly trauma patients and patients with high ISS score and long length of hospitalization and/or length of stay in ICU should be monitored carefully during hospitalization.
There are several limitations to this study. First, the study was confined to patients at a single center, and our study population may have been specific to a certain region. Second, because this was a non-randomized and retrospective analysis with a limited number of cases, the results are not conclusive and lacked sufficient statistical power to detect a significant difference. Therefore, additional prospective studies involving larger sample sizes will be necessary to support our findings.
CONCLUSION
Malnutrition is highly prevalent among severe trauma patients. Malnutrition risk is an independent risk factor for mortality and prolonged length of hospitalization and stay in ICU. Based on the malnutrition associated adverse outcomes, efforts should be made to quickly assess the nutritional status of these patients and early start nutritional intervention. In particular, Elderly and high-risk patients for malnutrition should be monitored carefully during hospitalization.
AUTHOR CONTRIBUTIONS
Conceptualization: HK, KHH. Data curation: KHH. Formal analysis: HK. Investigation: HK. Methodology: KHH, IC, KAL. Project administration: HK, GAS. Resources: KHH, IC, KAL. Supervision: GAS. Validation: KHH, KAL. Visualization: HK. Writing – original draft: HK. Writing – review & editing: KHH, IC, KAL, GAS.
CONFLICTS OF INTEREST
The authors of this manuscript have no conflicts of interest to disclose.
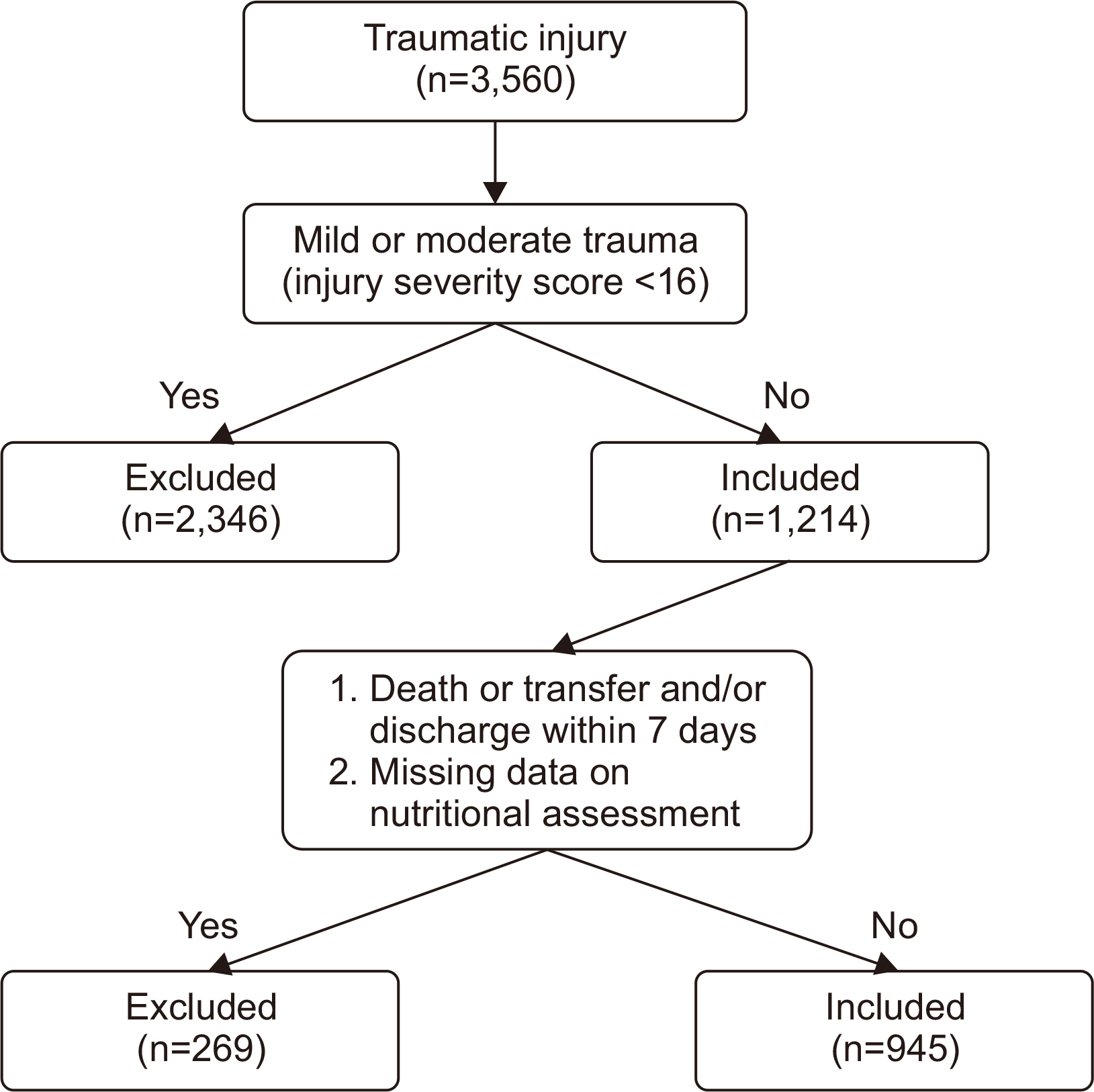
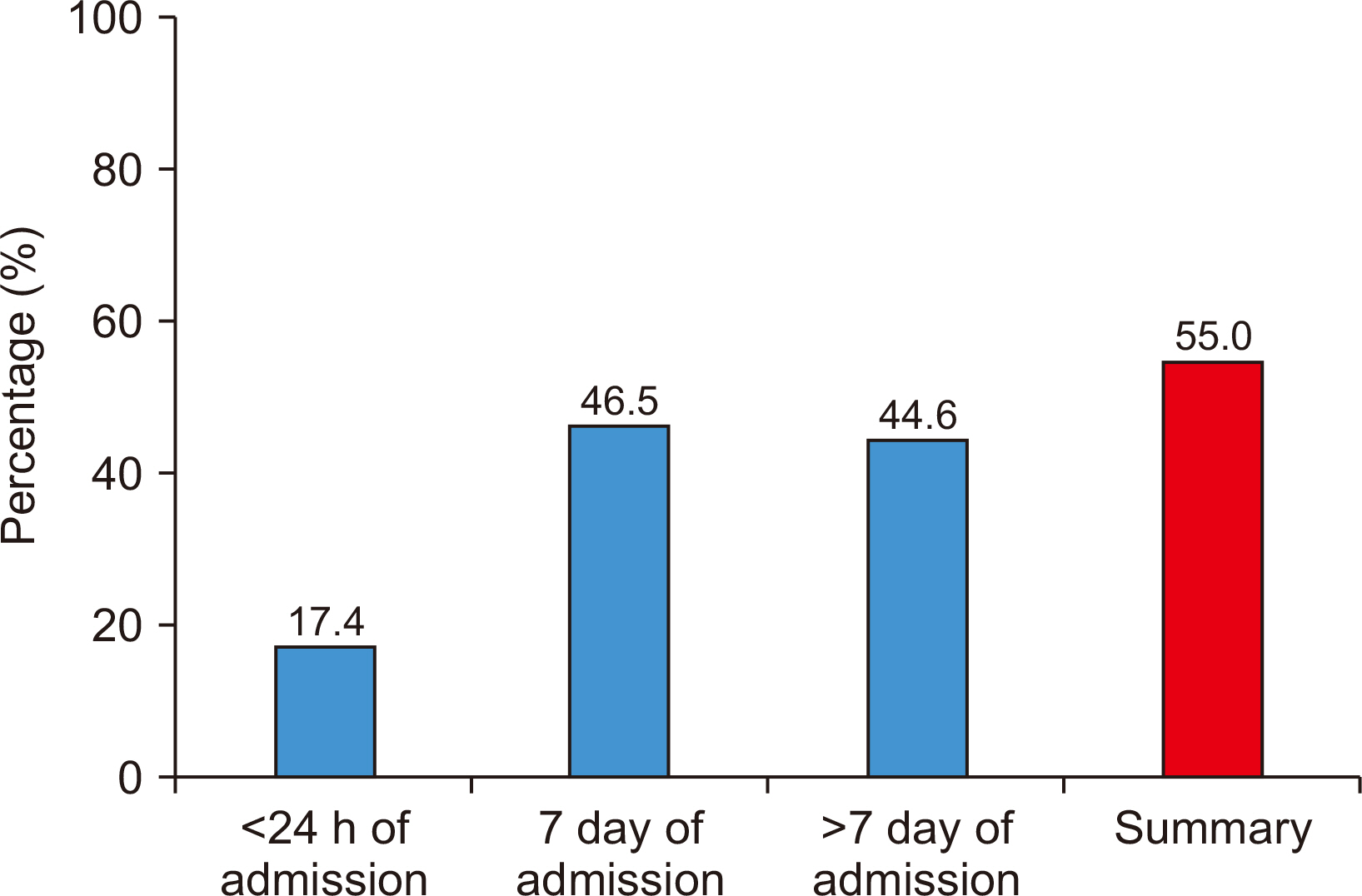
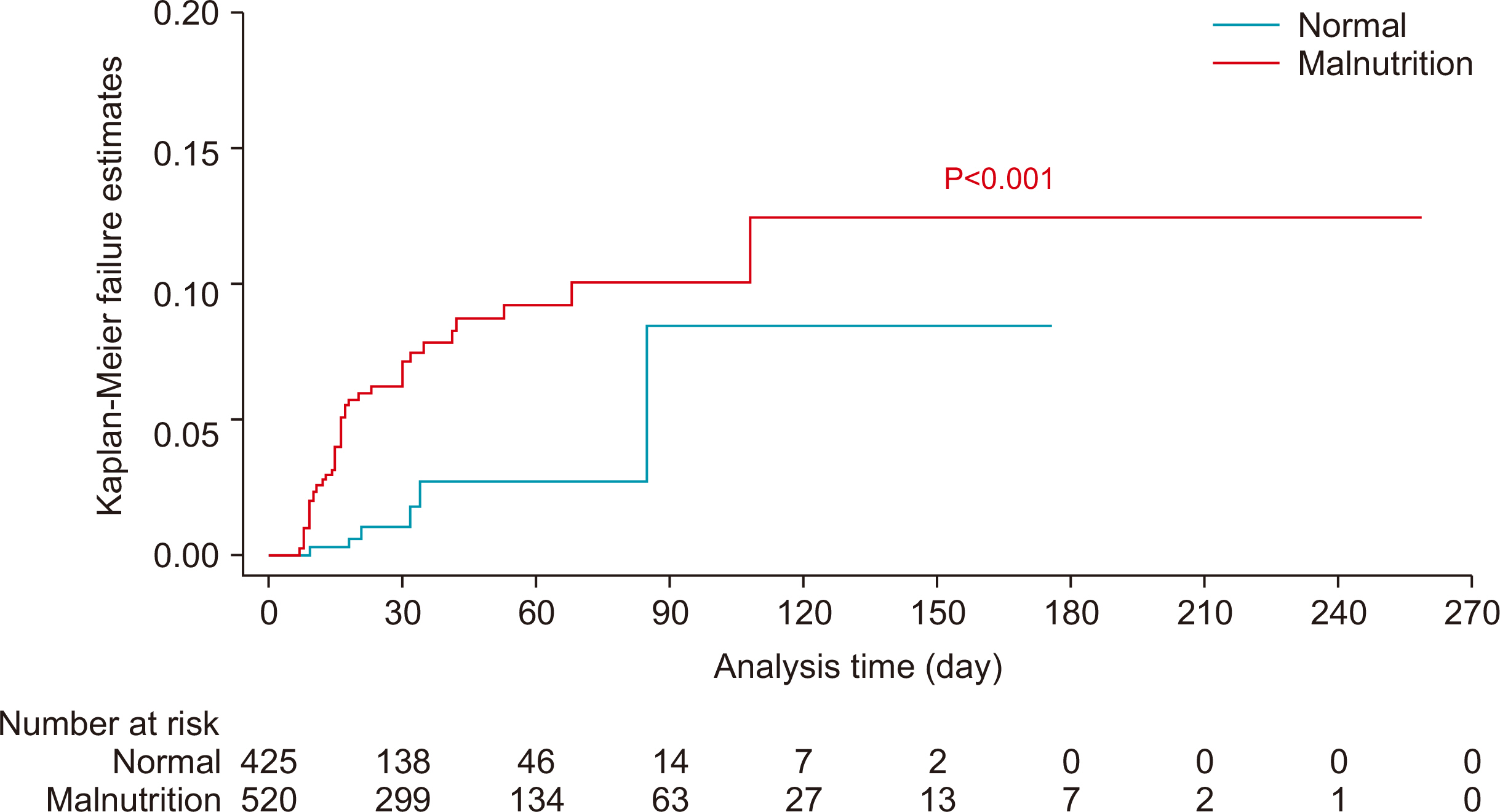
Table 1
Nutrition assessment tool in Pusan National University Hospital nutrition support team
Table 2
Clinical characteristics of patients with severe trauma
| Variable | Total group (n=945) | P-value | |
|---|---|---|---|
|
|
|||
| Survivor group (n=899) | Non-survivor group (n=46) | ||
| Malnutrition risk | |||
| <24 h of admission | 149 (16.6) | 15 (32.6) | 0.005 |
| 7 day of admission | 404 (44.9) | 35 (76.1) | <0.001 |
| >7 day of admissiona | 162 (41.8) | 22 (88.0) | <0.001 |
| Totalb | 480 (53.4) | 40 (87.0) | <0.001 |
| Age (≥65 yr) | 213 (23.7) | 23 (50.0) | <0.001 |
| Sex (male:female) | 704:195 | 36:10 | 0.994 |
| ISS | 24 (19~29) | 29 (25~34) | <0.001 |
| Head AIS | 3 (0~4) | 4 (3~5) | <0.001 |
| Abdomen AIS | 0 (0~2) | 0 (0~2) | 0.281 |
| GCS | 15 (12~15) | 9 (5~14) | <0.001 |
| Length of hospitalization (day) | 28 (18~51) | 16 (10~30) | <0.001 |
| Length of stay in ICU (day) | 5 (2~14) | 16 (11~30) | <0.001 |
Values are presented as number (%) or median (interquartile range).
ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit.
aSurvivor group (n=388), non-survivor group (n=25), Total (n=413).
bNutritional screening showed the positive malnutrition risk on <24 hours and/or 7 days and/or >7 days of admission.
Table 3
Univariable and multiple logistic regression analysis for mortality (n=945)
| Variable | Crude OR (95% CI) | P-value | Adjusted OR (95% CI) | P-value |
|---|---|---|---|---|
| Age (≥65 yr) | 3.221 (1.771~5.857) | <0.001 | 3.634 (1.842~7.170) | <0.001 |
| ISS | 1.049 (1.021~1.078) | 0.001 | ||
| Head AIS | 1.452 (1.207~1.747) | <0.001 | ||
| GCS | 0.818 (0.762~0.878) | <0.001 | 0.812 (0.752~0.877) | <0.001 |
| Malnutrition riska | 5.819 (2.443~13.863) | <0.001 | 3.440 (1.401~8.447) | 0.007 |
Table 4
Demographics of patients with severe trauma according to malnutrition risk
Table 5
Univariable and multiple logistic regression analyses for malnutrition risk (n=945)
- 1. Thomas MN, Kufeldt J, Kisser U, Hornung HM, Hoffmann J, Andraschko M, et al. Effects of malnutrition on complication rates, length of hospital stay, and revenue in elective surgical patients in the G-DRG-system. Nutrition 2016;32:249-54. ArticlePubMed
- 2. Geurden B, Franck E, Weyler J, Ysebaert D. The risk of malnutrition in community-living elderly on admission to hospital for major surgery. Acta Chir Belg 2015;115:341-7. ArticlePubMed
- 3. Pirlich M, Schütz T, Norman K, Gastell S, Lübke HJ, Bischoff SC, et al. The German hospital malnutrition study. Clin Nutr 2006;25:563-72. ArticlePubMed
- 4. Hertlein L, Kirschenhofer A, Fürst S, Beer D, Göβ C, Lenhard M, et al. Malnutrition and clinical outcome in gynecologic patients. Eur J Obstet Gynecol Reprod Biol 2014;174:137-40. ArticlePubMed
- 5. Karl A, Staehler M, Bauer R, Tritschler S, Hocaoglu Y, Buchner A, et al. Malnutrition and clinical outcome in urological patients. Eur J Med Res 2011;16:469-72. ArticlePubMedPMC
- 6. Felder S, Lechtenboehmer C, Bally M, Fehr R, Deiss M, Faessler L, et al. Association of nutritional risk and adverse medical outcomes across different medical inpatient populations. Nutrition 2015;31:1385-93. ArticlePubMed
- 7. Ihle C, Freude T, Bahrs C, Zehendner E, Braunsberger J, Biesalski HK, et al. Malnutrition - an underestimated factor in the inpatient treatment of traumatology and orthopedic patients: a prospective evaluation of 1055 patients. Injury 2017;48:628-36. ArticlePubMed
- 8. Mogensen KM, Robinson MK, Casey JD, Gunasekera NS, Moromizato T, Rawn JD, et al. Nutritional status and mortality in the critically ill. Crit Care Med 2015;43:2605-15. ArticlePubMed
- 9. Correia MI, Waitzberg DL. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr 2003;22:235-9. ArticlePubMed
- 10. Amaral TF, Matos LC, Tavares MM, Subtil A, Martins R, Nazaré M, et al. The economic impact of disease-related malnutrition at hospital admission. Clin Nutr 2007;26:778-84. ArticlePubMed
- 11. Clendenen N, Nunns GR, Moore EE, Reisz JA, Gonzalez E, Peltz E, et al. Hemorrhagic shock and tissue injury drive distinct plasma metabolome derangements in swine. J Trauma Acute Care Surg 2017;83:635-42. ArticlePubMedPMC
- 12. Goiburu ME, Goiburu MM, Bianco H, Díaz JR, Alderete F, Palacios MC, et al. The impact of malnutrition on morbidity, mortality and length of hospital stay in trauma patients. Nutr Hosp 2006;21:604-10. PubMed
- 13. Rogobete AF, Sandesc D, Papurica M, Stoicescu ER, Popovici SE, Bratu LM, et al. The influence of metabolic imbalances and oxidative stress on the outcome of critically ill polytrauma patients: a review. Burns Trauma 2017;5:8.ArticlePubMedPMCPDF
- 14. Wilson JM, Lunati MP, Grabel ZJ, Staley CA, Schwartz AM, Schenker ML. Hypoalbuminemia is an independent risk factor for 30-day mortality, postoperative complications, readmission, and reoperation in the operative lower extremity orthopaedic trauma patient. J Orthop Trauma 2019;33:284-91. ArticlePubMed
- 15. Mueller C, Compher C, Ellen DM. American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors. A.S.P.E.N. clinical guidelines: nutrition screening, assessment, and intervention in adults. JPEN J Parenter Enteral Nutr 2011;35:16-24. PubMed
- 16. Lochs H, Allison SP, Meier R, Pirlich M, Kondrup J, Schneider S, et al. Introductory to the ESPEN guidelines on enteral nutrition: terminology, definitions and general topics. Clin Nutr 2006;25:180-6. ArticlePubMed
- 17. Müller FS, Meyer OW, Chocano-Bedoya P, Schietzel S, Gagesch M, Freystaetter G, et al. Impaired nutritional status in geriatric trauma patients. Eur J Clin Nutr 2017;71:602-6. ArticlePubMedPDF
- 18. Goisser S, Schrader E, Singler K, Bertsch T, Gefeller O, Biber R, et al. Malnutrition according to mini nutritional assessment is associated with severe functional impairment in geriatric patients before and up to 6 months after hip fracture. J Am Med Dir Assoc 2015;16:661-7. ArticlePubMed
- 19. Chakravarty C, Hazarika B, Goswami L, Ramasubban S. Prevalence of malnutrition in a tertiary care hospital in India. Indian J Crit Care Med 2013;17:170-3. ArticlePubMedPMC
- 20. Norman K, Pichard C, Lochs H, Pirlich M. Prognostic impact of disease-related malnutrition. Clin Nutr 2008;27:5-15. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteClinical Significance of Malnutrition Risk in Severe Trauma Patients: A Single-Center Study
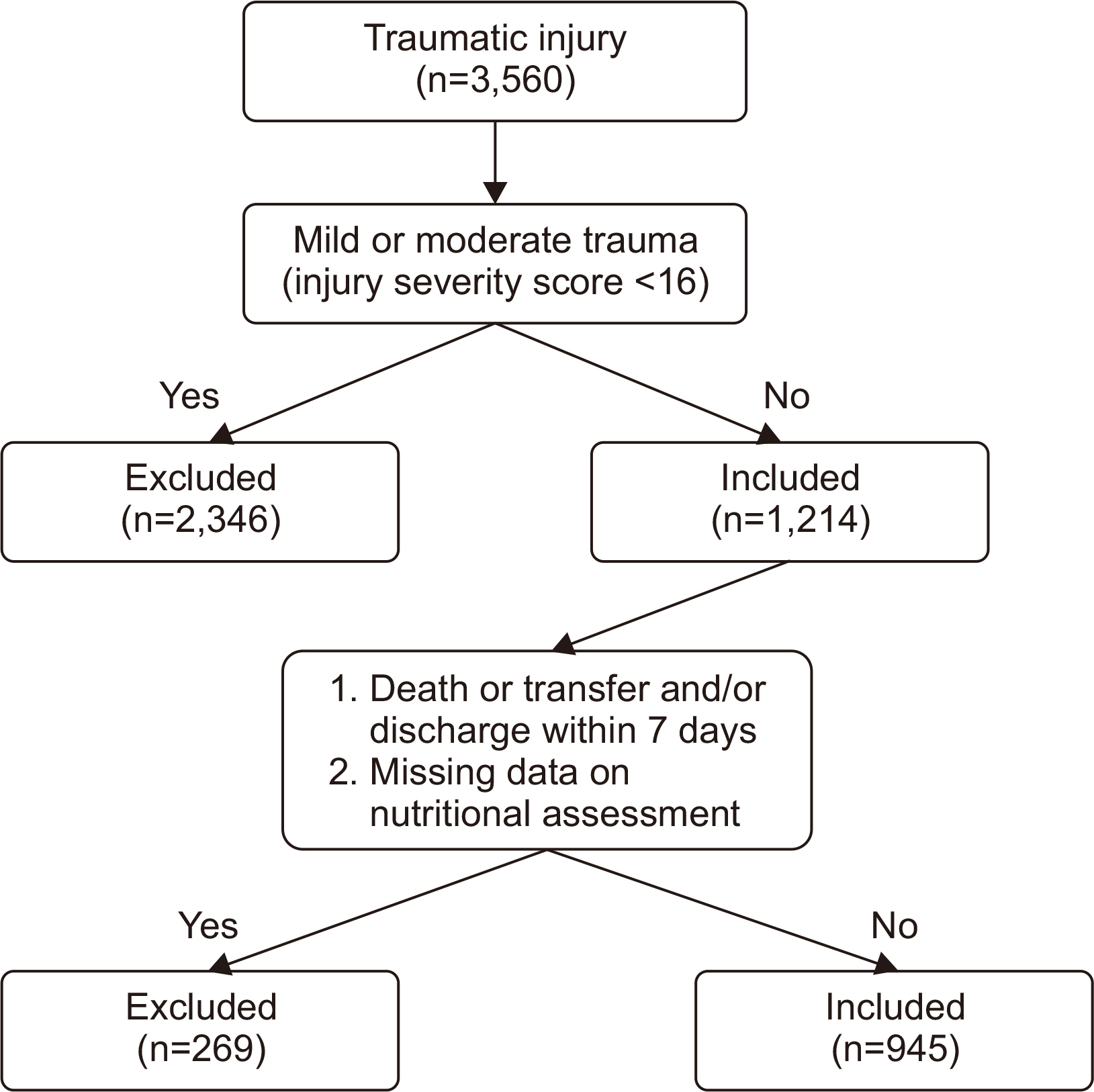
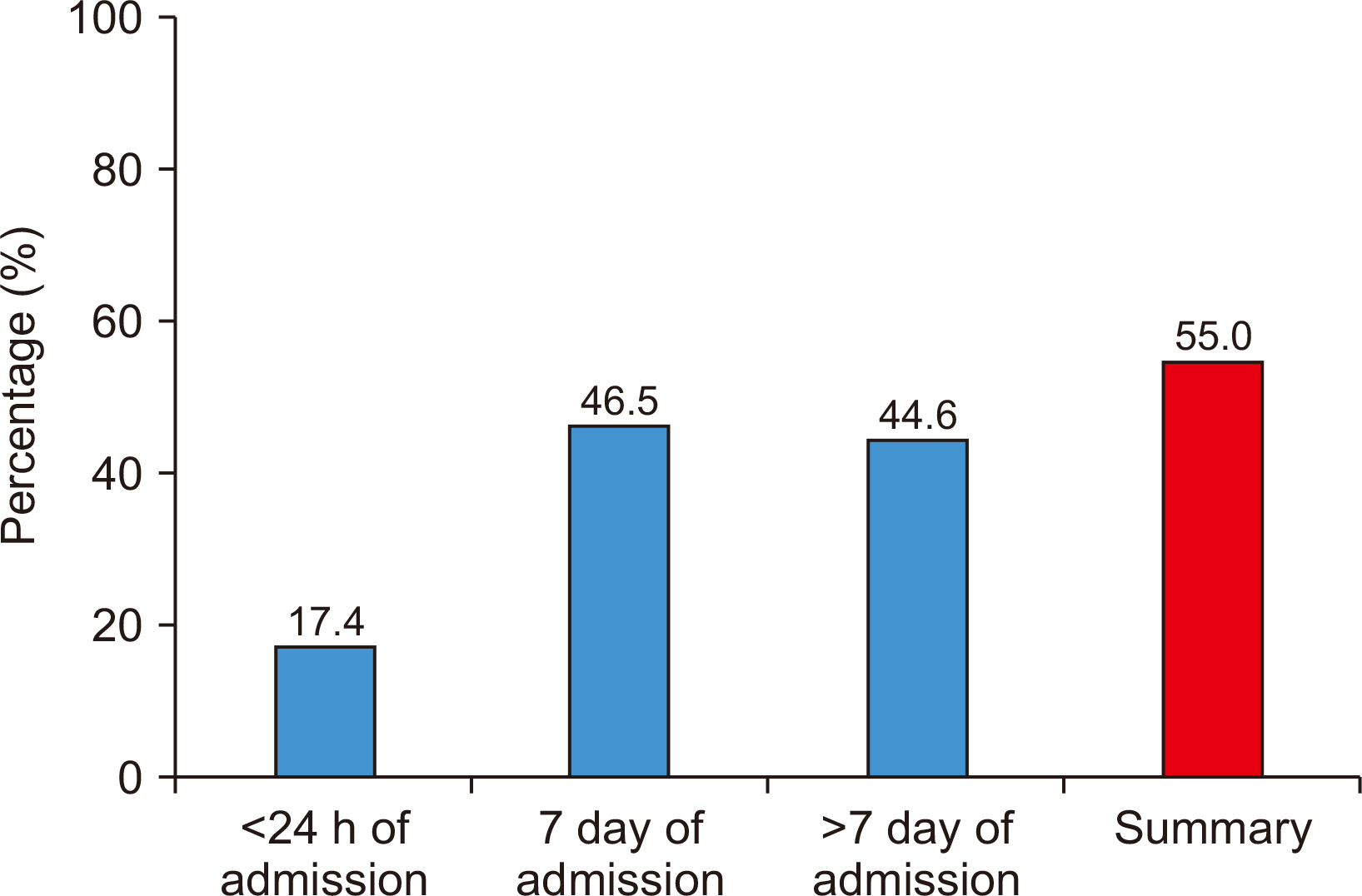
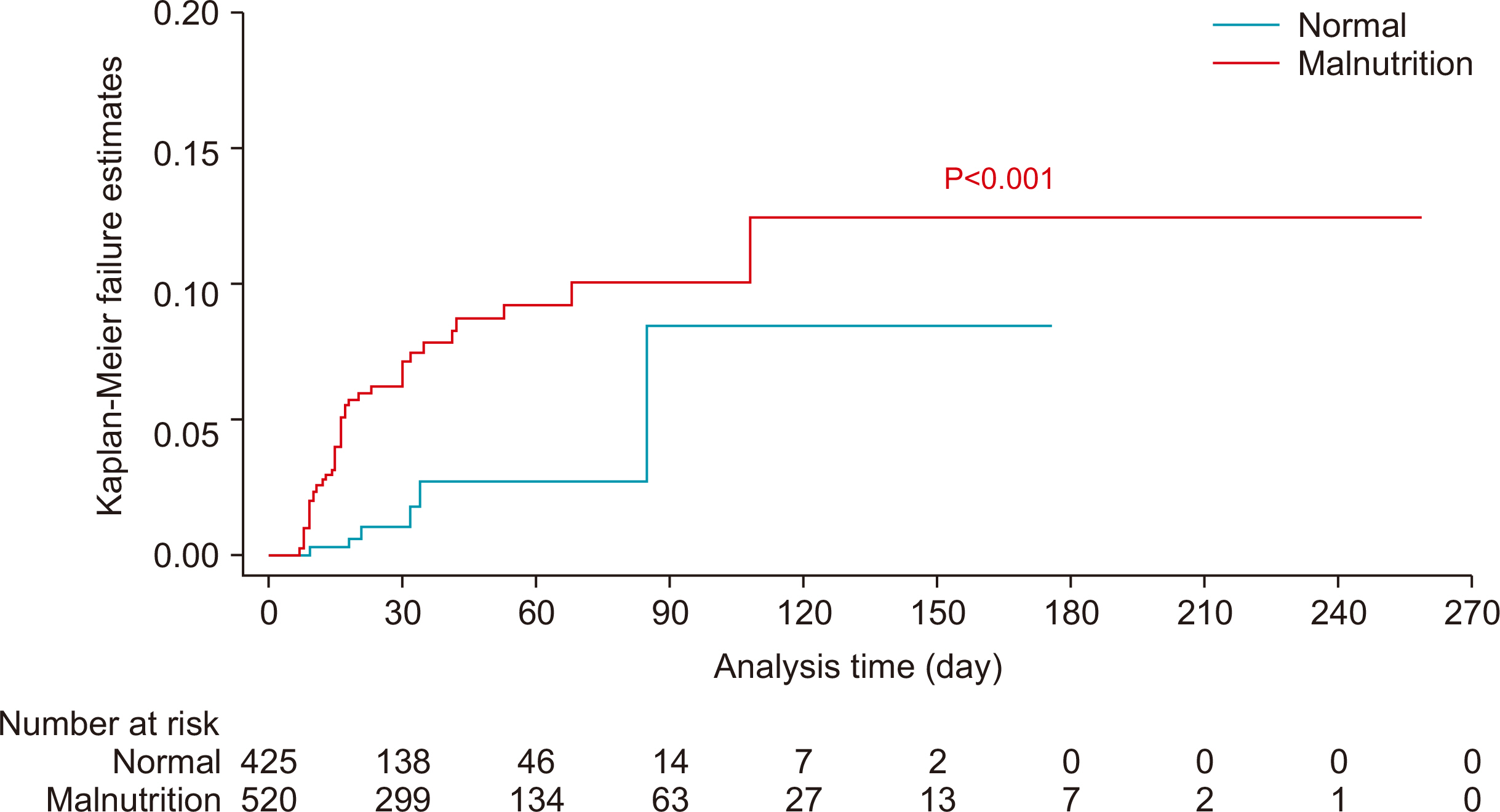
Fig. 1
Flowchart of the study.
Fig. 2
Prevalence of malnutrition risk of patients with severe trauma.
Fig. 3
One minus survival curve of patients with severe trauma according to malnutrition risk.
Fig. 1
Fig. 2
Fig. 3
Clinical Significance of Malnutrition Risk in Severe Trauma Patients: A Single-Center Study
Nutrition assessment tool in Pusan National University Hospital nutrition support team
| Variable | Degree of malnutrition | Note | |||
|---|---|---|---|---|---|
| None | Mild | Moderate | Severe | ||
| Albumin (g/dL) | >3.2 | 3.2~2.8 | 2.7~2.1 | <2.1 | N/A |
| Score | 0 | 2 | 4 | 6 | 0 |
| IBW (%) | ≥90 | 89.9~80 | 79.9~70 | <70 | N/A |
| Score | 0 | 1 | 2 | 3 | 3 |
| TLC (cell/mm3) | >1,500 | 1,200~1,500 | 800~1,199.9 | <800 | N/A |
| Score | 0 | 1 | 2 | 0 | |
| Appetite | Good or usual | Bad | N/A | ||
| Score | 0 | 2 | 0 | ||
| Number of GI problem | None | 1~2 | 3 | N/A | |
| Score | 0 | 1 | 2 | 0 | |
Positive malnutrition risk: ≥4 points.
N/A = non-applicable; IBW = ideal body weight; TLC = total lymphocyte count; GI = gastrointestinal.
Clinical characteristics of patients with severe trauma
| Variable | Total group (n=945) | P-value | |
|---|---|---|---|
| Survivor group (n=899) | Non-survivor group (n=46) | ||
| Malnutrition risk | |||
| <24 h of admission | 149 (16.6) | 15 (32.6) | 0.005 |
| 7 day of admission | 404 (44.9) | 35 (76.1) | <0.001 |
| >7 day of admission |
162 (41.8) | 22 (88.0) | <0.001 |
| Total |
480 (53.4) | 40 (87.0) | <0.001 |
| Age (≥65 yr) | 213 (23.7) | 23 (50.0) | <0.001 |
| Sex (male:female) | 704:195 | 36:10 | 0.994 |
| ISS | 24 (19~29) | 29 (25~34) | <0.001 |
| Head AIS | 3 (0~4) | 4 (3~5) | <0.001 |
| Abdomen AIS | 0 (0~2) | 0 (0~2) | 0.281 |
| GCS | 15 (12~15) | 9 (5~14) | <0.001 |
| Length of hospitalization (day) | 28 (18~51) | 16 (10~30) | <0.001 |
| Length of stay in ICU (day) | 5 (2~14) | 16 (11~30) | <0.001 |
Values are presented as number (%) or median (interquartile range).
ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit.
aSurvivor group (n=388), non-survivor group (n=25), Total (n=413).
bNutritional screening showed the positive malnutrition risk on <24 hours and/or 7 days and/or >7 days of admission.
Univariable and multiple logistic regression analysis for mortality (n=945)
| Variable | Crude OR (95% CI) | P-value | Adjusted OR (95% CI) | P-value |
|---|---|---|---|---|
| Age (≥65 yr) | 3.221 (1.771~5.857) | <0.001 | 3.634 (1.842~7.170) | <0.001 |
| ISS | 1.049 (1.021~1.078) | 0.001 | ||
| Head AIS | 1.452 (1.207~1.747) | <0.001 | ||
| GCS | 0.818 (0.762~0.878) | <0.001 | 0.812 (0.752~0.877) | <0.001 |
| Malnutrition risk |
5.819 (2.443~13.863) | <0.001 | 3.440 (1.401~8.447) | 0.007 |
OR = odds ratio; CI = confidence interval; ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale.
aNutritional screening showed the positive malnutrition risk on <24 hours and/or 7 days and/or >7 days of admission.
Demographics of patients with severe trauma according to malnutrition risk
| Variables | Total group (n=945) | P-value | |
|---|---|---|---|
| Normal group (n=425) | Malnutrition risk group (n=520) | ||
| Age (≥65 yr) | 72 (16.9) | 164 (31.5) | <0.001 |
| Sex (male:female) | 347:78 | 393:127 | 0.024 |
| ISS | 22 (17~27) | 25 (22~29) | <0.001 |
| Head AIS | 3 (0~4) | 3 (0~4) | 0.653 |
| Abdomen AIS | 0 (0~2) | 2 (0~2) | 0.005 |
| GCS | 15 (13~15) | 15 (9~15) | <0.001 |
| Length of hospitalization (day) | 22 (15~34) | 35 (20~61) | <0.001 |
| Length of stay in ICU (day) | 3 (2~8) | 10 (4~20) | <0.001 |
Values are presented as number (%) or median (interquartile range).
ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit.
Univariable and multiple logistic regression analyses for malnutrition risk (n=945)
| Variables | Crude OR (95% CI) | P-value | Adjusted OR (95% CI) | P-value |
|---|---|---|---|---|
| Age (≥65 yr) | 2.259 (1.650~3.091) | <0.001 | 2.393 (1.699~3.370) | <0.001 |
| Male | 0.696 (0.507~0.955) | 0.025 | ||
| ISS | 1.056 (1.036~1.076) | <0.001 | 1.034 (1.012~1.056) | 0.002 |
| Abdomen AIS | 1.135 (1.039~1.240) | 0.005 | ||
| GCS | 0.917 (0.882~0.953) | <0.001 | ||
| Length of hospitalization | 1.019 (1.014~1.025) | <0.001 | 1.014 (1.007~1.020) | <0.001 |
| Length of stay in ICU | 1.066 (1.050~1.083) | <0.001 | 1.050 (1.029~1.072) | <0.001 |
OR = odds ratio; CI = confidence interval; ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit.
Table 1
Nutrition assessment tool in Pusan National University Hospital nutrition support team
Positive malnutrition risk: ≥4 points. N/A = non-applicable; IBW = ideal body weight; TLC = total lymphocyte count; GI = gastrointestinal.
Table 2
Clinical characteristics of patients with severe trauma
Values are presented as number (%) or median (interquartile range). ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit. aSurvivor group (n=388), non-survivor group (n=25), Total (n=413). bNutritional screening showed the positive malnutrition risk on <24 hours and/or 7 days and/or >7 days of admission.
Table 3
Univariable and multiple logistic regression analysis for mortality (n=945)
OR = odds ratio; CI = confidence interval; ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale. aNutritional screening showed the positive malnutrition risk on <24 hours and/or 7 days and/or >7 days of admission.
Table 4
Demographics of patients with severe trauma according to malnutrition risk
Values are presented as number (%) or median (interquartile range). ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit.
Table 5
Univariable and multiple logistic regression analyses for malnutrition risk (n=945)
OR = odds ratio; CI = confidence interval; ISS = injury severity score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ICU = intensive care unit.

