 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 15(1); 2023 > Article
- Review Efficacy of monounsaturated fatty acids in reducing risk of the cardiovascular diseases, cancer, inflammation, and insulin resistance: a narrative review
-
Ki Hyun Kim
 , Yoonhong Kim, Kyung Won Seo
, Yoonhong Kim, Kyung Won Seo -
Annals of Clinical Nutrition and Metabolism 2023;15(1):2-7.
DOI: https://doi.org/10.15747/ACNM.2023.15.1.2
Published online: April 1, 2023
Department of Surgery, Kosin University College of Medicine, Busan, Korea
- Corresponding author: Kyung Won Seo, email: kwseo@office.kosin.ac.kr
• Received: October 26, 2022 • Revised: December 22, 2022 • Accepted: December 26, 2022
© 2023 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 40,127 Views
- 156 Download
- 12 Crossref
- Abstract
- Introduction
- Potential health benefits of olive oil
- Benefit of lipids as a source of energy and their relationship with immunity
- History of intravenous lipid emulsions
- Characteristics and effects of olive oil-based LEs
- The benefits of MUFAs focusing on the guidelines
- Conclusion
- Acknowledgments
- Notes
- References
Abstract
-
Purpose The purpose of this review is to explore the potential benefits of monounsaturated fatty acids (MUFAs), specifically those found in olive oil, on weight loss, cardiovascular disease, cancer, inflammation, and insulin resistance. Additionally, this review examines the use of olive oil–based intravenous lipid emulsions (ILEs) in providing parenteral nutrition to patients with diverse needs.
-
Current concept MUFAs, found in olive oil, nuts, and some animal foods, have been found to have numerous health benefits. A diet high in MUFAs can aid in weight loss and reduce the risk of cardiovascular disease. Olive oil, in particular, has been linked to a lower risk of cancer, inflammation, and insulin resistance. In addition, olive oil–based ILEs have been utilized for over two decades and are well tolerated by patients requiring parenteral nutrition.
-
Conclusion A diet rich in MUFAs, specifically from olive oil, can provide numerous health benefits, including weight loss and reducing the risk of cardiovascular disease, cancer, inflammation, and insulin resistance. Additionally, olive oil–based ILEs have been shown to effectively provide nutrients to diverse populations requiring parenteral nutrition and have demonstrated the ability to preserve immune function and induce less lipid peroxidation than other ILEs. Further research is needed to fully understand the potential benefits of MUFAs and olive oil-based ILEs, but current evidence suggests that they may be a valuable addition to a healthy diet and medical treatment.
Introduction
The type of fat found in parenteral nutrition (PN) formulations is triglycerides [1]. Triglycerides consist of a trio of fatty acid molecules bound to a glycerol backbone. A fatty acid molecule consists of a hydrocarbon ring and a methyl group (CH3) at one end of the ring and a reactive carboxyl group (COOH) at the other end. Fatty acids can be classified based on the length of the hydrocarbon ring, the number of carbon–carbon double bonds in the ring (saturation), and the position of the first double bond in the ring [2]. Saturated fatty acids such as stearic acid do not have double bonds. Monounsaturated fatty acids (MUFAs) like oleic acid have one double bond and polyunsaturated fatty acids (PUFAs), such as linoleic acid, have two or more double bonds. Fatty acids can be classified according to the position of the first double bond based on the ω (non-carboxylic acid) end of the hydrocarbon ring, known as the omega (ω or n) class. Using the omega classification, fatty acids with the first double bond on the third carbon relative to the ω terminus are ω-3 fatty acids (e.g., α-linoleic acid), fatty acids with the first double bond on the sixth carbon relative to the ω terminus are ω-6 fatty acids (e.g., linoleic acid), and fatty acids with a double bond at the ninth carbon from the ω terminus are ω-9 fatty acids (e.g., oleic acid) (Fig. 1). The clinical advantages and effectiveness of MUFAs were explored in this research.
Potential health benefits of olive oil
Olive oil is a liquid fat obtained by pressing whole olives. Olives are one of the key foods in Mediterranean cuisine and have been cultivated around the Mediterranean since 8000 BC. Today, olive oil is commonly used for frying foods or in salad dressings and is rich in ω-9 MUFAs, showing many health-related beneficial effects. In the United States (U.S.), the Food and Drug Administration allows olive oil producers to claim eligible health benefits on product labels. Due to the MUFAs, consuming roughly 2 T (23 g) of olive oil daily may lower the risk of coronary heart disease [3]. To lower the risk of heart disease, olive oil can replace a similar amount of saturated fat without increasing the total number of calories consumed per day. Several studies have shown that eating a diet high in MUFAs increases the high-density lipoprotein cholesterol concentration and reduces triacylglycerol levels [4,5]. Foods rich in MUFAs may help to regulate blood lipid profiles. Additionally, MUFAs can have a long-term hypoglycemic impact in type 2 diabetic individuals by decreasing the glycosylated hemoglobin concentration. Dietary management in type 2 diabetes mellitus (T2DM) is critical for reducing long-term complications. In a meta-analysis comparing a diet high in cis-MUFAs and a diet high in carbohydrates or PUFAs to assess metabolic risk factors in patients with T2DM [6], substantial reductions in fasting plasma glucose, triglycerides, and systolic blood pressure as well as significant increases in high-density lipoprotein cholesterol were identified when comparing high-MUFA to high-carbohydrate diets. In addition, fasting plasma glucose was significantly lower in high-MUFA diets compared to high-PUFA diets. This meta-analysis provides evidence that diets high in MUFAs can improve metabolic risk factors among patients with T2DM. For these reasons, national and international authorities recommend consumption of MUFAs [3]. However, several American societies have suggested that <20% MUFAs be consumed to prevent heart disease. Among various vegetable oils, when sorted by the ω-9 content, olive oil contains the highest percentage of MUFAs with >70% MUFAs. Therefore, olive oil may be a significant provider of MUFAs.
Benefit of lipids as a source of energy and their relationship with immunity
Lipid emulsions (LEs) are added to standard PN regimens for several reasons. First, they provide essential fatty acids. For example, both linoleic acid and α-linolenic acid are regarded as necessary fatty acids because they must be delivered to rather than being produced by the human body. LEs also allow the body to achieve the high caloric intake required by some patients without excessive glucose calories, thereby averting the hyperglycemia associated with the original glucose-rich admixture. They also help to reduce solution osmolarity, protect veins, and enhance the bioavailability of fat-soluble vitamins like vitamins A, D, E, and K. As the representative ω-3 PUFA, α-linoleic acid is converted in the body to eicosapentaenoic acid and docosahexaenoic acid through the action of several enzymes. Meanwhile, linoleic acid, the representative ω-6 PUFA, is converted to arachidonic acid through the action of the same enzymes. Among ω-6 fatty acids, the final metabolite has a proinflammatory effect, whereas the final metabolite of ω-3 fatty acids has an anti-inflammatory effect. On the other hand, oleic acid, a representative ω-9 MUFA, leads to a neutral immune response even though it undergoes a metabolic process and its metabolites do not participate in the immune response (Fig. 2).
History of intravenous lipid emulsions
The first attempt to infuse lipid parenterally took place in 1678. In 1955, the first intravenous lipid emulsion (ILE), a cottonseed oil–based emulsion (composed of 15% cottonseed oil, 1.2% soy phospholipids, 0.3% Pluronic 568, and 4% dextrose) was approved for use in the U.S.. However, it was later withdrawn from the market because of severe adverse reactions. In 1961, a soybean oil ILE (10% or 20% soybean oil ILE and 1.2% egg phospholipids) was introduced in Europe and it was approved for use in the U.S. in 1975. Then, in May 1979, 10% and 20% ILEs containing exclusively safflower oil were introduced into the U.S. market. In 1984, this product was reformulated to 10% and 20% ILEs at a 1:1 volume ratio in a blend of soybean oil and safflower oils for the purpose of increasing the α-linolenic acid content of the emulsion. In 2010, the manufacturer of safflower oil-containing products ceased manufacturing all ILEs, leaving a single source of ILE on the U.S. market, soybean oil. An soybean oil- and olive oil-based ILE was approved for use in 2013 but it was not marketed in the U.S. until 2019. In 2016, a 4-oil ILE was approved, while an exclusive fish oil-based ILE, which had been used previously on a compassionate-use basis, was approved in 2018 [7].
In terms of nutrition support, the lipid combination has changed over time. Consider the LEs used in PN as a good example of this. The first generation of such LEs consisted purely of soybean oil, the second-generation LEs includes medium-chain triglycerides (MCTs) extracted from coconut oil, and the third generation began to include structured lipids and olive oil. Most recently, third-generation LEs containing fish oil have been introduced [8]. The evolution of lipid sources used in PN over time started with first-generation, 100% soybean oil-based ILEs in the 1960s and currently includes third-generation products such as structured lipids, olive oil-based ILEs, and fish oil-containing ILE [8,9]. The characteristics of MUFAs are as follows. First, olive oil-based PN is the main source of oleic acid. Second, this product has relatively neutral physiologic effects. Third, a high MUFA content imparts greater resistance to peroxidation.
Characteristics and effects of olive oil-based LEs
The innate immune system is supported by olive oil-based ILEs, which may help to retain immunological function. Similarly, olive oil-based ILEs are likely to experience lower lipid peroxidation than soybean oil-based ILEs. Most studies have explained that olive oil-based ILEs maintain hepatobiliary marker and plasma lipid levels within normal or near-normal ranges. olive oil-based LEs have a higher percentage of MUFAs and lower potency of oxidation than fish oil-based LEs with PUFAs, resulting in less cell damage [10]. ω-9 fatty acids (e.g., oleic acid in olive oil) influence the metabolic effects of lipids but do not produce eicosanoids. ω-9 fatty acids reduce lipid peroxidation, preserve the immune function, and have a neutral inflammatory effect [11-14]. IV olive oil-based LEs are associated with fewer infections. A large, prospective, randomized, open-label, multicenter, non-inferiority study in China assessed the delivery, efficacy, and safety of soybean oil-based PN and olive oil-based PN in patients who required PN therapy during admission to hospitals for surgery. The results showed that the olive oil-based LE PN group experienced a significantly lower rate of infection compared to the soybean oil-based PN group [15]. In another study of trauma patients, sepsis markers improved over time in those who received olive oil-based PN and the lengths of mechanical ventilation and intensive care unit stays were shorter in the olive oil-based PN group [16]. However, there are studies which produced conflicting or seemingly unrelated results. Another prospective, double-blind, randomized controlled trial of patients receiving PN containing an soybean oil-based or olive oil-based LE showed similar overall rates of communicable and non-infectious complications, mortality, and length of stay in the intensive care unit. In addition, there were no significant differences of the metabolic, inflammatory, or immune markers among critically ill adult patients [17]. Another study showed no effect of an soybean oil-based vs. olive oil-based LE on infections, acute-phase proteins, or major health outcomes [18]. Further, since there are not many studies on the difference between olive oil-based and fish oil-based ILEs, additional research is needed in this area.
The benefits of MUFAs focusing on the guidelines
In the 2009 European Society for Clinical Nutrition and Metabolism (ESPEN) guideline, first and second generations of LEs were recommended for patients. The guideline also advised olive oil-based parenteral feeding of critically ill patients. At that time, research results of studies on fish oil were just starting to be released, as demonstrated in the guidelines [19]. According to the 2017 ESPEN surgery recommendations, postoperative PN with ω-3 fatty acids should be examined and surgical patients who receive ω-3 fatty acids have considerable advantages in terms of the postoperative infection rate and hospital length of stay [20]. With the accumulation of many research results on fish oil, the current guideline comprises a strong recommendation. In addition, the guideline recommends avoidance of ω-6 fatty acids. Alternative LEs (olive oil, fish oil, MCT) are available. olive oil also showed an advantage over soybean oil in terms of the length of hospital stay [21]. American Society for Parenteral and Enteral Nutrition classified the various ILEs available based on study design and potential benefits (Table 1) [22]. Among them, the advantages of third-generation ILEs are presented [7]. First, MUFAs produce less peroxide during oxidation than PUFAs. Second, oleic acid in olive oil is not metabolized as a mediator of inflammation or immunity. In conclusion, considering the relatively neutral physiological effects and reduced susceptibility to peroxidation, MUFAs can be effectively used for nutritional treatment of immunosuppressed or immunocompromised patients [23].
Conclusion
MUFAs are fatty acids most commonly found in olive oil, nuts, and some animal foods. Third-generation injectable LEs may have advantages in certain clinical areas. As revealed during in vivo studies, MUFAs such as oleic acid have only one double bond and are less susceptible to lipid peroxidation compared to acids with additional double bonds. ω-9 fatty acids may benefit immunosuppressed patients because they reduce lipid peroxidation, preserve immune function, and have a neutral effect on inflammation.
Acknowledgments
None.
Authors’ contribution
Conceptualization: KWS. Formal analysis: KHK, YK. Methodology: KHK. Project administration: KHK, KWS. Supervision: KWS. Validation: KHK, KWS. Visualization: KHK, YK. Writing – original draft: KHK. Writing – review & editing: KHK, KWS.
Conflict of interest
Kyung Won Seo is an editorial board member of the journal, but was not involved in the review process of this manuscript. Otherwise, there is no conflict of interest to declare.
Funding
None.
Data availability
None.
Supplementary materials
None.
Fig. 1
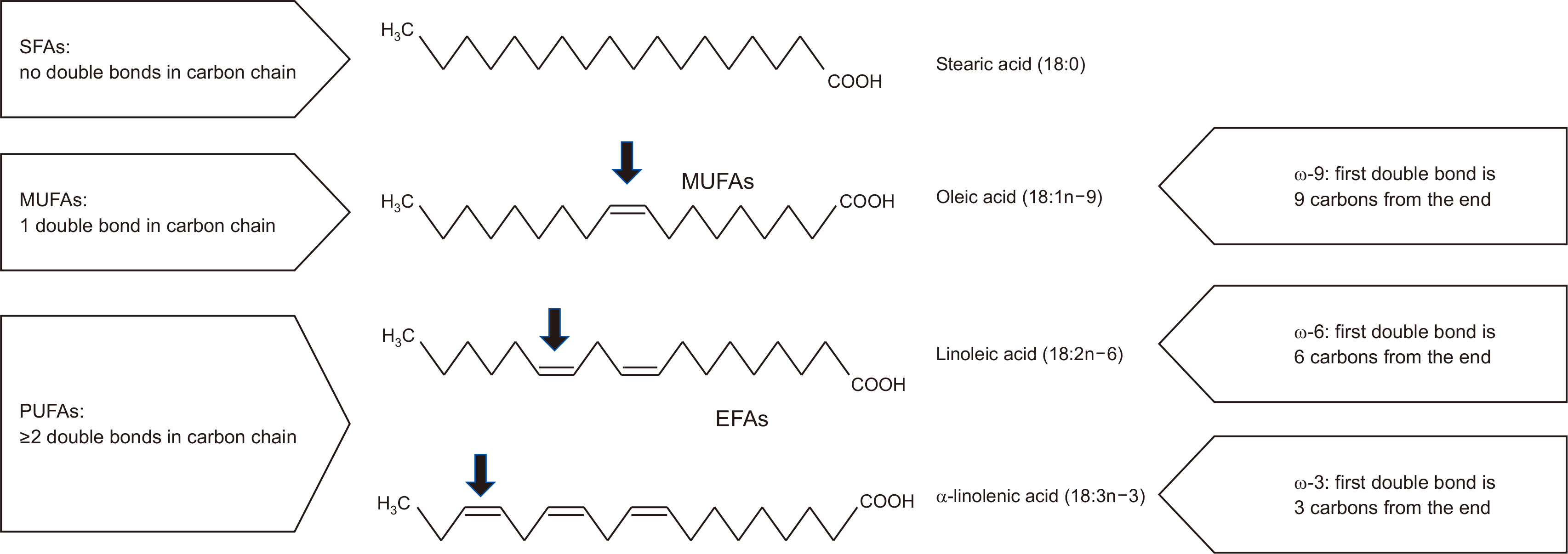
Structure and naming of selected 18-carbon fatty acids (drawing by the authors).
The black arrows indicate the first double bond.
SFA = saturated fatty acid; MUFA = mono-unsaturated fatty acid; PUFA = polyunsaturated fatty acid; EFA = essential fatty acid; COOH = carboxyl group.
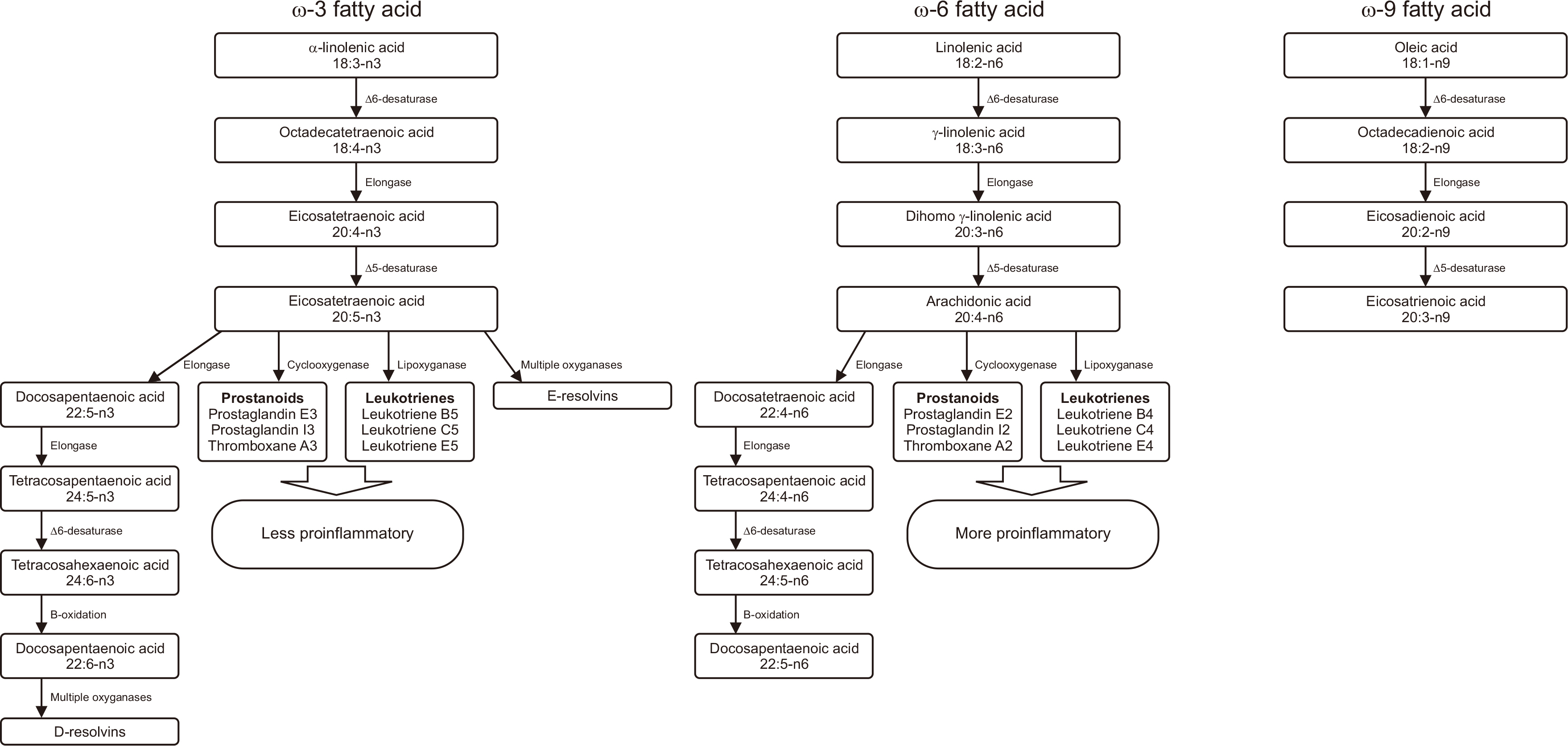
Table 1
Evolution of intravenous lipid emulsions
Revised from the article of Mirtallo et al. (Nutr Clin Pract 2020;35:769-82) [7] with original copyright holder’s permission.
ILE = lipid injectable emulsion; MCT = medium-chain triglyceride; EFA = essential fatty acid; FA = fatty acid; MUFA = monounsaturated fatty acid; PUFA = polyunsaturated fatty acid; IFALD = intestinal failure-associated liver disease.
- 1. Gomes F, Schuetz P, Bounoure L, Austin P, Ballesteros-Pomar M, Cederholm T, et al. ESPEN guidelines on nutritional support for polymorbid internal medicine patients. Clin Nutr 2018;37:336-53. ArticlePubMed
- 2. Wanten GJ, Calder PC. Immune modulation by parenteral lipid emulsions. Am J Clin Nutr 2007;85:1171-84. ArticlePubMed
- 3. Schwingshackl L, Hoffmann G. Monounsaturated fatty acids and risk of cardiovascular disease: synopsis of the evidence available from systematic reviews and meta-analyses. Nutrients 2012;4:1989-2007. ArticlePubMedPMC
- 4. Cao X, Xia J, Zhou Y, Wang Y, Xia H, Wang S, et al. The effect of MUFA-rich food on lipid profile: a meta-analysis of randomized and controlled-feeding trials. Foods 2022;11:1982.ArticlePubMedPMC
- 5. Mensink RP, Katan MB. Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arterioscler Thromb 1992;12:911-9. ArticlePubMed
- 6. Qian F, Korat AA, Malik V, Hu FB. Metabolic effects of monounsaturated fatty acid-enriched diets compared with carbohydrate or polyunsaturated fatty acid-enriched diets in patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Care 2016;39:1448-57. ArticlePubMedPMCPDF
- 7. Mirtallo JM, Ayers P, Boullata J, Gura KM, Plogsted S, Anderson CR, et al. ASPEN lipid injectable emulsion safety recommendations, part 1: background and adult considerations. Nutr Clin Pract 2020;35:769-82; Erratum in: Nutr Clin Pract 2022;37:482. ArticlePubMedPDF
- 8. Calder PC, Adolph M, Deutz NE, Grau T, Innes JK, Klek S, et al. Lipids in the intensive care unit: recommendations from the ESPEN Expert Group. Clin Nutr 2018;37:1-18. ArticlePubMed
- 9. Wu GH, Zaniolo O, Schuster H, Schlotzer E, Pradelli L. Structured triglycerides versus physical mixtures of medium- and long-chain triglycerides for parenteral nutrition in surgical or critically ill adult patients: systematic review and meta-analysis. Clin Nutr 2017;36:150-61. ArticlePubMed
- 10. Demirer S, Sapmaz A, Karaca AS, Kepenekci I, Aydintug S, Balci D, et al. Effects of postoperative parenteral nutrition with different lipid emulsions in patients undergoing major abdominal surgery. Ann Surg Treat Res 2016;91:309-15. ArticlePubMedPMCPDF
- 11. Reimund JM, Scheer O, Muller CD, Pinna G, Duclos B, Baumann R. In vitro modulation of inflammatory cytokine production by three lipid emulsions with different fatty acid compositions. Clin Nutr 2004;23:1324-32. ArticlePubMed
- 12. Pontes-Arruda A, Aragão AM, Albuquerque JD. Effects of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanically ventilated patients with severe sepsis and septic shock. Crit Care Med 2006;34:2325-33. PubMed
- 13. Waitzberg DL, Torrinhas RS, Jacintho TM. New parenteral lipid emulsions for clinical use. JPEN J Parenter Enteral Nutr 2006;30:351-67. ArticlePubMedPDF
- 14. Calder PC, Jensen GL, Koletzko BV, Singer P, Wanten GJ. Lipid emulsions in parenteral nutrition of intensive care patients: current thinking and future directions. Intensive Care Med 2010;36:735-49. ArticlePubMedPMC
- 15. Jia ZY, Yang J, Xia Y, Tong DN, Zaloga GP, Qin HL. Safety and efficacy of an olive oil-based triple-chamber bag for parenteral nutrition: a prospective, randomized, multi-center clinical trial in China. Nutr J 2015;14:119.PubMedPMC
- 16. Huschak G, Zur Nieden K, Hoell T, Riemann D, Mast H, Stuttmann R. Olive oil based nutrition in multiple trauma patients: a pilot study. Intensive Care Med 2005;31:1202-8. ArticlePubMedPDF
- 17. Umpierrez GE, Spiegelman R, Zhao V, Smiley DD, Pinzon I, Griffith DP, et al. A double-blind, randomized clinical trial comparing soybean oil-based versus olive oil-based lipid emulsions in adult medical-surgical intensive care unit patients requiring parenteral nutrition. Crit Care Med 2012;40:1792-8. ArticlePubMedPMC
- 18. Mateu-de Antonio J, Grau S, Luque S, Marín-Casino M, Albert I, Ribes E. Comparative effects of olive oil-based and soyabean oil-based emulsions on infection rate and leucocyte count in critically ill patients receiving parenteral nutrition. Br J Nutr 2008;99:846-54. ArticlePubMed
- 19. Braga M, Ljungqvist O, Soeters P, Fearon K, Weimann A, Bozzetti F. Guidelines on parenteral nutrition: surgery. Clin Nutr 2009;28:378-86. PubMed
- 20. Weimann A, Braga M, Carli F, Higashiguchi T, Hübner M, Klek S, et al. ESPEN guideline: clinical nutrition in surgery. Clin Nutr 2017;36:623-50. ArticlePubMed
- 21. Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr 2019;38:48-79. ArticlePubMed
- 22. Vanek VW, Seidner DL, Allen P, Bistrian B, Collier S, Gura K, et al. A.S.P.E.N. position paper: clinical role for alternative intravenous fat emulsions. Nutr Clin Pract 2012;27:150-92. PubMed
- 23. Anez-Bustillos L, Dao DT, Baker MA, Fell GL, Puder M, Gura KM. Intravenous fat emulsion formulations for the adult and pediatric patient: understanding the differences. Nutr Clin Pract 2016;31:596-609. PubMedPMC
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Effects of daily extra virgin olive oil consumption on biomarkers of inflammation and oxidative stress: a systematic review and meta-analysis
Jéssica Vidal Damasceno, Anderson Garcez, Andressa Anelo Alves, Isabella Rosa da Mata, Simone Morelo Dal Bosco, Juliano Garavaglia
Critical Reviews in Food Science and Nutrition.2026; 66(2): 392. CrossRef - Applying Wild Mistol Fruits (Sarcomphalus Mistol) from the Paraguayan Chaco as Value-Added Food Ingredients
Villalba R., Belotto J., Coronel E., Carvajal M., Recalde C., Caballero S., Friesen A., Mereles L.
Plant Foods for Human Nutrition.2026;[Epub] CrossRef - Multi-Omics Integration Reveals Key Genes, Metabolites and Pathways Underlying Meat Quality and Intramuscular Fat Deposition Differences Between Tibetan Pigs and Duroc × Tibetan Crossbred Pigs
Junda Wu, Qiuyan Huang, Baohong Li, Zixiao Qu, Xinming Li, Fei Li, Haiyun Xin, Jie Wu, Chuanhuo Hu, Sen Lin, Xiangxing Zhu, Dongsheng Tang, Chuang Meng, Zongliang Du, Erwei Zuo, Fanming Meng, Sutian Wang
Animals.2026; 16(2): 214. CrossRef - The MetaboHealth Score Enhances Insulin Resistance Metabotyping for Targeted Fat Loss: The PERSON Study
Jordi Morwani‐Mangnani, Fatih A. Bogaards, Alexander Umanets, Gabby B. Hul, Anouk Gijbels, Gijs H. Goossens, Joris Deelen, Marian Beekman, Lydia Afman, Ellen E. Blaak, P. Eline Slagboom
Obesity.2026; 34(3): 550. CrossRef - Video and Text‐Based Supplemental Health Information and Consumer Willingness to Pay for Nutrient‐Enhanced Eggs
Edeoba W. Edobor, Michael J. Best, Anita R. Best, Ondulla T. Toomer
Agribusiness.2026;[Epub] CrossRef - Optimizing Pistacia lentiscus (mastic tree) food and healthcare applications: phytochemical composition, extraction methods, quality control, and novel delivery systems
Mohamed A. Anwar, Yuting Fu, Haroun Khan, Mohamed A. Farag
Phytochemistry Reviews.2026; 25(5): 3249. CrossRef - Soybean molasses: a promising substrate for the production of microbial oil by Phaffia rhodozyma
Shirley Denisse Ccori Ponce, Luiz Henrique Han, Luiz Antonio de Almeida Pinto, Carlos André Veiga Burkert, Janaina Fernandes de Medeiros Burkert
Bioprocess and Biosystems Engineering.2026;[Epub] CrossRef - The impact of Lactiplantibacillus plantarum on the cream composition: Insight into changes of vitamin D3 content and fatty acid composition
Tetiana Dyrda-Terniuk, Viorica Railean, Aleksandra Bogumiła Florkiewicz, Justyna Walczak-Skierska, Mateusz Kolankowski, Joanna Rudnicka, Dorota Białczak, Paweł Pomastowski
International Dairy Journal.2025; 161: 106118. CrossRef - Palmitoleic and oleic fatty acids as biomarkers for coronary heart disease: A predictive model
Guangzhou Wang, Lin Zhou, Zhengfang Wang, Asmaa Ali, Liang Wu
Irish Journal of Medical Science (1971 -).2025; 194(1): 59. CrossRef - Macrophages: their role in immunity and their relationship with fatty acids in health and disease
Mayte Rueda-Munguía, Luis Alberto Luévano-Martínez, Gerardo García-Rivas, Elena Cristina Castillo, Omar Lozano
Frontiers in Immunology.2025;[Epub] CrossRef - Evaluation of the Nutritional Value of Prunus dulcis Blossoms and the Antioxidant Compounds of Their Extracted Oil Using Green Extraction Method
Theodoros Chatzimitakos, Vassilis Athanasiadis, Konstantina Kotsou, Ioannis Makrygiannis, Eleni Bozinou, Stavros I. Lalas
Applied Sciences.2024; 14(5): 2001. CrossRef - Oleic Acid and Succinic Acid: A Potent Nutritional Supplement in Improving Hepatic Glycaemic Control in Type 2 Diabetic Sprague–Dawley Rats
Kemmoy G. Lattibeaudiere, Ruby Lisa Alexander-Lindo, Mozaniel Oliveira
Advances in Pharmacological and Pharmaceutical Sciences.2024;[Epub] CrossRef
 Cite
CiteEfficacy of monounsaturated fatty acids in reducing risk of the cardiovascular diseases, cancer, inflammation, and insulin resistance: a narrative review
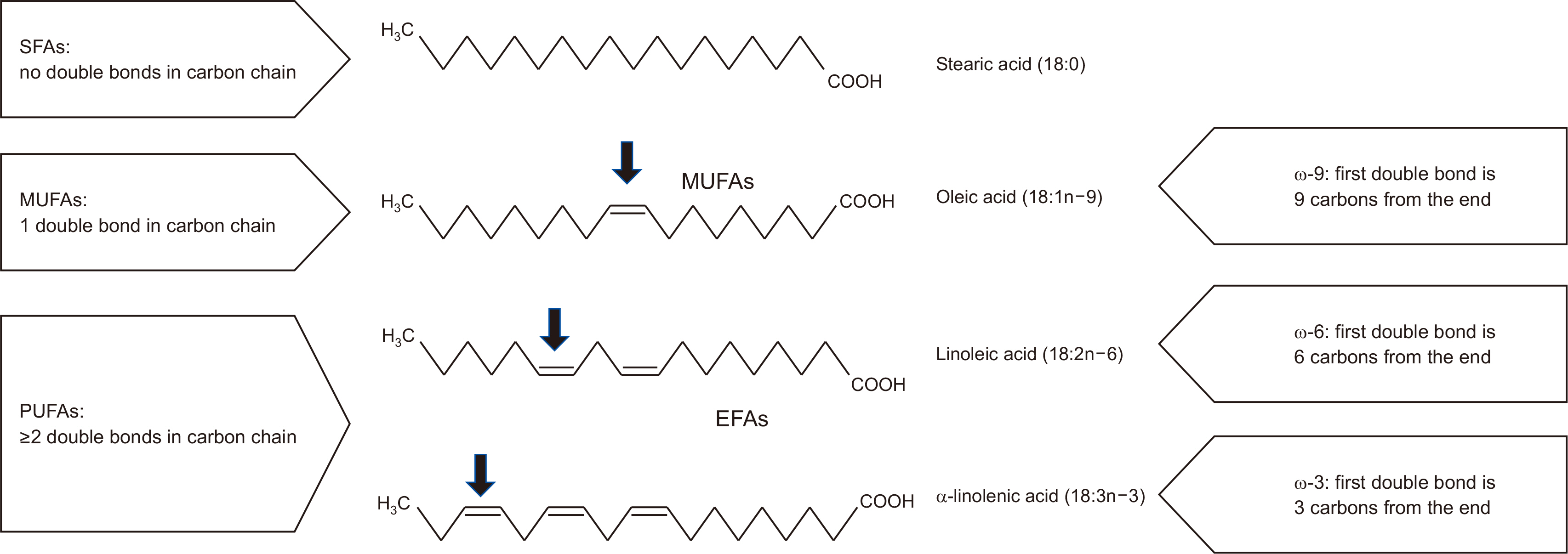
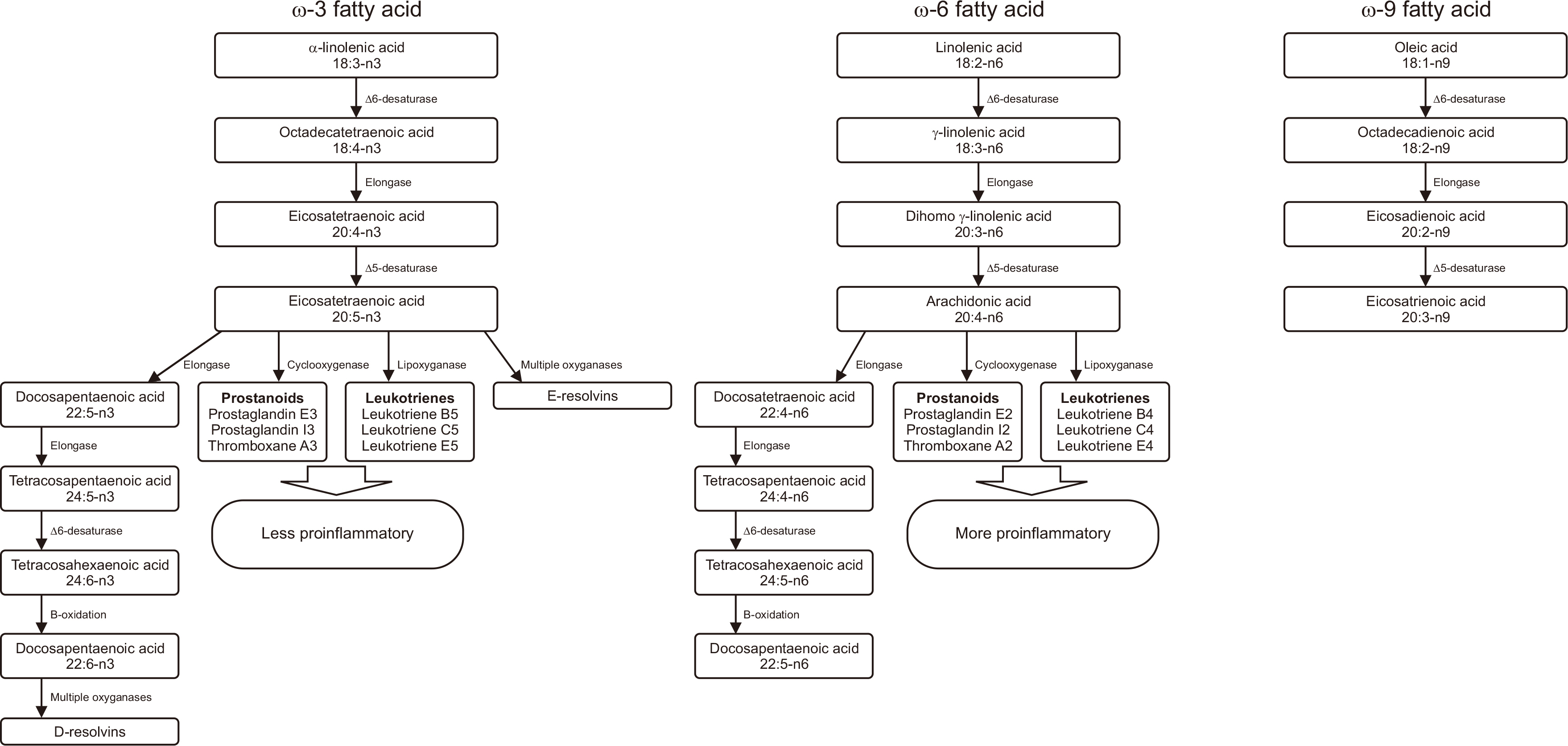
Fig. 1
Structure and naming of selected 18-carbon fatty acids (drawing by the authors).
The black arrows indicate the first double bond.
SFA = saturated fatty acid; MUFA = mono-unsaturated fatty acid; PUFA = polyunsaturated fatty acid; EFA = essential fatty acid; COOH = carboxyl group.
Fig. 2
Metabolic pathways of ω-3, ω-6, and ω-9 fatty acids (drawing by the authors).
Fig. 1
Fig. 2
Efficacy of monounsaturated fatty acids in reducing risk of the cardiovascular diseases, cancer, inflammation, and insulin resistance: a narrative review
Evolution of intravenous lipid emulsions
| Generation of ILE | Description | Potential benefits |
|---|---|---|
| First | Soybean oil or safflower oil | Information about compatibility with regularly used drugs is provided |
| Second | Two-oil formulation including soybean oil and MCT | MCTs are removed more quickly and with less peroxidation |
| Third | Two-oil ILE using soybean oil and olive oil, resulting in a reduced amount of EFA (ω-6 FAs) | Elevated doses of MUFAs produce fewer peroxides during oxidation than PUFAs Oleic acid in olive oil is not converted to inflammatory or immune mediators Patients who are at risk of immunosuppression or have impaired immune systems may benefit from this treatment |
| Fourth | Four-oil ILE of soybean oil, MCT, olive oil, and fish oil | Fish oil included for critically ill and surgical patient populations |
| Fish oil | Sources of FA and energy for infants and children with IFALD and may reverse IFALD |
Revised from the article of Mirtallo et al. (Nutr Clin Pract 2020;35:769-82) [
ILE = lipid injectable emulsion; MCT = medium-chain triglyceride; EFA = essential fatty acid; FA = fatty acid; MUFA = monounsaturated fatty acid; PUFA = polyunsaturated fatty acid; IFALD = intestinal failure-associated liver disease.
Table 1
Evolution of intravenous lipid emulsions
Revised from the article of Mirtallo et al. (Nutr Clin Pract 2020;35:769-82) [ ILE = lipid injectable emulsion; MCT = medium-chain triglyceride; EFA = essential fatty acid; FA = fatty acid; MUFA = monounsaturated fatty acid; PUFA = polyunsaturated fatty acid; IFALD = intestinal failure-associated liver disease.

