 E-submission
E-submission
Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 17(1); 2025 > Article
- Original Article Impact of postoperative nutritional status on the patients’ clinical outcomes and knee biomechanics following total knee arthroplasty in Japan: a prospective cohort study
-
Kenichi Kono1,2
 , Tetsuya Tomita3,4, Takaharu Yamazaki5, Masashi Tamaki3, Shuji Taketomi2, Ryota Yamagami2, Reo Inoue1, Yuki Taniguchi1,2, Sakae Tanaka2, Kazuhiko Fukatsu1
, Tetsuya Tomita3,4, Takaharu Yamazaki5, Masashi Tamaki3, Shuji Taketomi2, Ryota Yamagami2, Reo Inoue1, Yuki Taniguchi1,2, Sakae Tanaka2, Kazuhiko Fukatsu1 -
Annals of Clinical Nutrition and Metabolism 2025;17(1):50-57.
DOI: https://doi.org/10.15747/ACNM.24.019
Published online: April 1, 2025
1Surgical Center, The University of Tokyo Hospital, Tokyo, Japan
2Department of Orthopedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan
3Department of Orthopedic Biomaterial Science, Osaka University Graduate School of Medicine, Suita, Japan
4Master Course of Health Sciences, Graduate School of Health Sciences, Morinomiya University of Medical Sciences, Osaka, Japan
5Department of Information Systems, Faculty of Engineering, Saitama Institute of Technology, Fukaya, Japan
- Corresponding author: Kenichi Kono, email: kkouno_tki@yahoo.co.jp
• Received: November 18, 2024 • Revised: November 29, 2024 • Accepted: December 24, 2024
© 2025 Korean Society of Surgical Metabolism and Nutrition · Korean Society for Parenteral and Enteral Nutrition · Asian Society of Surgical Metabolism and Nutrition · Japanese Society for Surgical Metabolism and Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 172 Views
- 5 Download
Abstract
-
Purpose The impact of postoperative nutritional status on clinical outcomes and biomechanics following total knee arthroplasty remains largely unknown. This study aimed to assess this question using the prognostic nutritional index to evaluate the nutritional status of orthopedic participants.
-
Methods Patients with knee osteoarthritis who underwent total knee arthroplasty (n=49) in Japan were divided into two groups based on their 1-week postoperative prognostic nutritional index. Group L patients had a prognostic nutritional index <40, whereas Group H comprised patients with a prognostic nutritional index ≥40. Postoperative improvements in Knee Injury and Osteoarthritis Outcome Score were evaluated. The patients performed squats under single-fluoroscopic surveillance in the sagittal plane for biomechanical evaluation. A two-dimensional/three-dimensional registration technique was employed to measure the tibiofemoral kinematics. The axial rotation of the femoral component relative to the tibial component and the anteroposterior translation of the medial and lateral femorotibial contact points were measured.
-
Results Group H showed significantly higher pain scores than Group L at 12 and 36 months postoperatively and a significantly higher symptom score at 36 months postoperatively. The kinematic comparison revealed that the axial external rotation in Group L was larger than that in Group H from 70° to 80° with flexion. Moreover, in the medial anteroposterior translation, Group L was more anteriorly located than Group H, with flexion beyond 30°.
-
Conclusion The results suggest that a high postoperative nutritional status significantly improved pain and other symptoms and was associated with better knee biomechanics following total knee arthroplasty.
Graphical abstract
Introduction
Malnutrition induces postoperative complications in total knee arthroplasty (TKA) and leads to sarcopenia. Resistance exercises such as squats are recommended to improve sarcopenia [1,2]. Moreover, combining resistance exercise with proper nutrition provides greater improvement in patients with sarcopenia [1,2]. In TKA, the force of the leg muscles, such as the quadriceps, plays a significant role in predicting postoperative functional prognosis and patient satisfaction [3]. Resistance exercises are effective in rehabilitation following TKA [4]; therefore, it is important to evaluate both the nutritional status and resistance exercises to determine the impact on postoperative outcomes following TKA. Recent studies have reported that TKA kinematics are related to clinical outcomes, such as patient-reported outcome measures (PROMs) [5-7]. However, the impact of postoperative nutritional status on clinical outcomes and biomechanics remains largely unknown.
There are various methods for evaluating the nutritional status [8-11]; Onodera’s prognostic nutritional index (PNI) can be easily calculated using simple, low-cost blood tests [8,12]. The PNI is a strong prognostic indicator after surgery [12,13]. In orthopedic surgeries such as TKA, most patients exhibit early recovery postoperatively. Therefore, simple blood tests are typically performed. Thus, the PNI serves as a useful evaluation tool after orthopedic surgery.
This study was designed to evaluate the effects of postoperative nutritional status on clinical outcomes and biomechanics after TKA using PNI. We hypothesized that the postoperative nutritional status affects the improvement of PROMs and knee biomechanics.
Methods
This study was approved by the University of Tokyo Institutional Ethics Review Board (number: 10462-(1)), and performed in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all the participants included in the study. The patients provided informed consent for publication of their data and photographs.
It was a prospective cohort study. It was described according to the STOBE statement, which is available at: https://www.strobe-statement.org/.
All patients in this study were evaluated at The University of Tokyo Hospital between October 2015 and December 2019.
Patients (n=49) with knee osteoarthritis who underwent TKA using the Journey Ⅱ BCS system (Smith & Nephew) were recruited for the study. Patients were divided into two groups based on their 1-week postoperative PNI to exclude the effects of fasting and supplementation.
Dependent variables were Knee Injury and Osteoarthritis Outcome Score (KOOS) as a clinical outcome and knee biomechanics values. Independent variable was Onodera’s PNI as a postoperative nutritional status.
There was no selection bias since all target patients were recruited.
Data were from the patient’s medical records, measurement score, and X-ray images
The PNI was calculated from the serum albumin level and lymphocyte count as described previously: 10×albumin (g/dL)+0.005×total lymphocyte count (/mm3) [8,13]. PNI scores lower than 40 are associated with poor postoperative longevity [8]. Therefore, patients were divided according to PNI with a threshold of 40. Group L (n=20) had a PNI <40, while Group H (n=29) had a PNI ≥40. The mean PNI in Groups L and H were 36.4±1.9 and 43.1±2.2, respectively. The neutrophil-to-lymphocyte ratio (NLR) was calculated as the total neutrophil count (/mm3)/total lymphocyte count (/mm3) [12,14].
A medial parapatellar surgical approach in which the patella was not everted was used. The distal femur and proximal tibia were incised using a navigation system (Precision N; Stryker Orthopedics). The femur was aligned at 90° to the mechanical axis in the frontal plane with 4° flexion in the sagittal plane, and the tibia was aligned at 90° to the mechanical axis in the frontal plane with a posterior slope of 3° in the sagittal plane. The femoral rotation was determined using the average rotational axis of the transepicondylar axis and the axis perpendicular to the Whiteside axis, whereas the tibial rotation was determined using the range of motion technique [15,16].
The postoperative improvement in PROMs using the KOOS was evaluated. The KOOS is a self-reported questionnaire with 42 items comprising five separately analyzed subscales of pain; symptoms; and activities of daily living (ADL) for physical function, sport/recreation function, and knee-related quality of life (QOL). Each of the five scores is calculated as the sum of the items included, and the scores are then transformed to a 0- to 100-point scale, with 0 points representing extreme knee problems and 100 points representing no knee problems [17]. KOOS was measured at 3, 6, 12, 24, and 36 months after TKA (Table 1).
Patients who could safely perform deep-standing squats after surgery were evaluated (Fig. 1). Each patient was asked to perform deep-standing squats at a natural pace under single-fluoroscopic surveillance in the sagittal plane. The squats were performed from full extension to maximum flexion. The participants practiced the motion several times before being recorded as sequential digital radiographic images (1024×1024×12 bits/pixel, 7.5-Hz serial spot images in a DICOM file) using a 17-inch flat panel detector system (ZEXIRA DREX-ZX80; Toshiba). All images were processed using dynamic-range compression for edge enhancement.
To estimate the spatial position and orientation of the femoral and tibial components, a 2D-to-3D registration technique was used [18,19]. This technique is designed on a contour-based registration algorithm that uses single-view fluoroscopic images and 3D computer-aided design models. The margin of error of the estimated relative motion between the metal components was ≤0.5° for rotation and ≤0.4° for translation. The following variables were measured: knee range of motion, varus-valgus alignment, axial rotation of the femoral component relative to the tibial component, and anteroposterior (AP) translation of the medial and lateral femorotibial contact points. A local coordinate system for the femoral component was used according to previously described methods [18,20]. Knee flexion and rotation angles were described using the joint rotational convention method described by Grood and Suntay [21]. Flexion and external rotation of the femoral component relative to the tibial component are denoted as positive values. Positive and negative AP translation values are defined as those anterior and posterior to the axes of the tibial component, respectively. The femorotibial contact point is defined as the region on the insertion surface where the proximity of the component surfaces is less than the 0.5-mm threshold.
The primary endpoint of this study was the comparison of knee biomechanics between Group H and Group L. Since all target participants had been recruited prior to the study, a prospective sample size calculation was not feasible. Therefore, a post-hoc power analysis was conducted using G*Power to evaluate the statistical power for detecting differences in knee biomechanics between the groups. Based on a two-tailed test, an effect size of 0.375, sample sizes of 20 in Group H and 29 in Group L, and a correlation of 0.72 among repeated measures [22], the calculated statistical power (1−β error probability) was 0.941.
Statistical analyses were conducted using SPSS version 25 (IBM Corp.). For correlated observations, such as PROMs and knee biomechanics, repeated-measures analysis of variance was applied. The model included time as a within-subjects factor and group (Groups H and L) as a between-subjects factor, followed by Bonferroni correction for multiple comparisons. Only inter-group effects were evaluated. The Mann–Whitney U test was used to compare white blood cell count, C-reactive protein (CRP) levels, NLR, age, body mass index, fluoroscopic follow-up distance, and sex ratio between Groups H and L. A P-value of <0.05 was considered statistically significant. Data are presented as means±standard deviations.
Results
The patients’ demographic findings and clinical characteristics are presented in Table 2. The postoperative white blood cell count, CRP level, and NLR are shown. CRP levels and NLR in Group L were significantly higher than those in Group H. There were no significant differences between the groups regarding age, body mass index, fluoroscopic follow-up distance, or sex ratio.
The KOOS scores gradually improved in both groups. However, the KOOS-pain score in Group H was significantly higher than in Group L at 12 and 36 months. Additionally, the KOOS-symptoms score was significantly higher in Group H than that in Group L at 36 months. There were no significant differences between the two groups in terms of KOOS-ADL, sports/recreation, or QOL (Fig. 2, Supplement 1).
The axial external rotation in Group L was greater than that in Group H from 70° to 80° with flexion (Fig. 3, Supplement 2). In medial AP translation, Group L was located more anteriorly than Group H, beyond 30° with flexion. In contrast, there was no significant difference in the lateral AP translation between the two groups (Fig. 4, Supplement 3).
Discussion
The most important finding of this study was that high nutritional status can improve PROMs and knee kinematics after TKA. The KOOS-pain and KOOS-symptoms scores in Group H were significantly higher compared to those in Group L. In particular, improvements were seen beyond 1 year after surgery.
This finding suggests that the perioperative nutritional status affects midterm clinical outcomes. Several studies have reported that appropriate nutrition has anti-inflammatory effects and improves pain [23,24]. Therefore, early nutritional improvement may provide postoperative pain relief.
In this study, femoral external rotation in Group L was larger than that in Group H at mid-flexion. In addition, the medial AP translation in Group L was more anteriorly located than that in Group H beyond early flexion. A previous study reported that, after TKA, the low PROMs groups exhibited excessive femoral external rotation [6]. Patients with malnutrition such as those in Group L could easily perform external femoral rotation according to the implant’s guided motion design. In addition, excessive femoral external rotation can lead to iliotibial band traction syndrome, which causes poor clinical outcomes [25]. Another study reported that, after TKA, the low PROMs group displayed medial anterior translation with flexion [5]. These findings suggest that a high postoperative nutritional status might improve knee biomechanics. Several studies have demonstrated that a combination of nutrition and resistance exercise results in greater improvement in patients with sarcopenia [1,2]. Moreover, muscle-loaded stability reflects knee stability after TKA [26-29]. Therefore, not only patients with sarcopenia but general patients after TKA might require a combination of nutrition and resistance exercises, such as squats, to improve postoperative clinical outcomes.
The postoperative (1 week after surgery) CRP level and NLR were significantly higher in Group L than those in Group H. A high postoperative NLR is associated with poor prognosis after surgery [30,31]. These findings suggest that prolonged postoperative inflammation may result in poor clinical outcomes and knee kinematics.
First, we evaluated only the perioperative nutritional status. Further studies are required to assess the nutritional status during long-term follow-up. Second, only one type of implant was evaluated, and other implants may exhibit different biomechanical properties. Third, we did not analyze the kinematics preoperatively to minimize X-ray exposure. Therefore, this study did not directly compare the pre- and postoperative kinematics. Hence, we cannot rule out the possibility that the preoperative knee kinematics affected the postoperative kinematics. Additionally, for variables 10°, 20°, and 30°, the sample size was insufficient; therefore, future studies focusing specifically on the variables with low power would need larger sample sizes to achieve adequate statistical power.
This study demonstrated that postoperative nutritional status significantly influences clinical outcomes and knee biomechanics following TKA. Patients with higher prognostic nutritional indices experienced superior pain relief, symptom improvement, and more favorable knee kinematics than patients with low indices. These findings stress the importance of optimizing nutritional status, potentially in combination with resistance exercises, to enhance recovery.
Authors’ contribution
Conceptualization: KK. Methodology: TT, TY, MT, Shuji Taketomi, RI, YT, Sakae Tanaka, KF. Formal analysis/validation: KK, RY. Project administration: KK. Funding acquisition: Not applicable. Writing – original draft: KK. Writing – review & editing: all authors. All authors read and approved the final manuscript.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
None.
Data availability
Research data are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Dr. Yuhei Saito and Dr. Hiroshi Okawa, Surgical Center, The University of Tokyo Hospital, Tokyo, Japan; Shoji Konda, Department of Health and Sport Sciences, Osaka University Graduate School of Medicine, Osaka, Japan; Teruya Ishibashi, Department of Orthopaedic Biomaterial Science, Osaka University Graduate School of Medicine, Osaka, Japan; and Tomofumi Kage and Takahiro Arakawa, Department of Orthopaedic Surgery, Faculty of Medicine The University of Tokyo, Tokyo, Japan for providing advice on the kinematic data.
Supplementary materials
Fig. 1.
Patient who could safely perform deep-standing squats after surgery for fluoroscopic analysis.
Fig. 2.
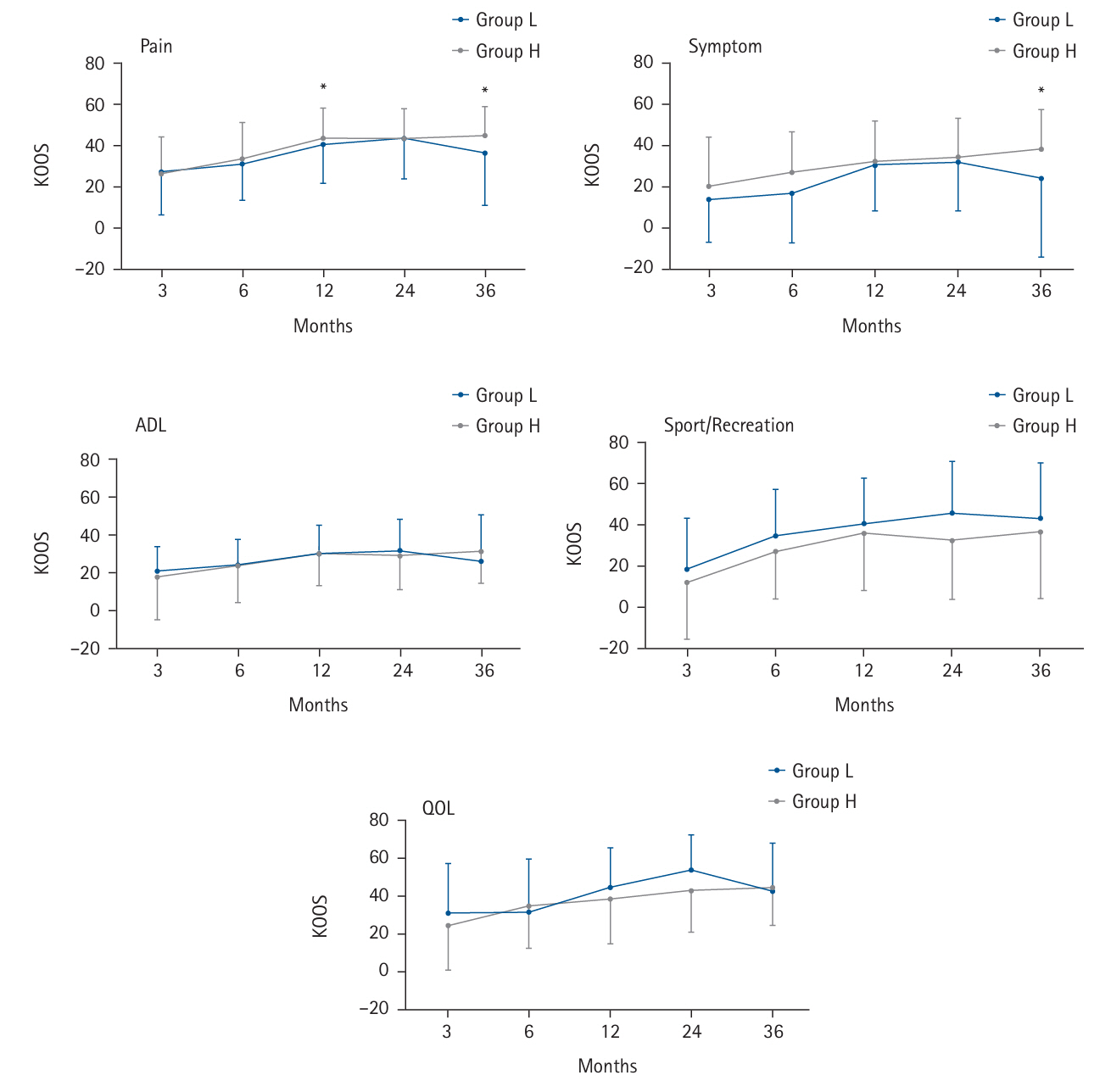
Comparison of patient-reported outcome measures (Knee Injury and Osteoarthritis Outcome Score, KOOS) between Groups L and H. Group L had a Prognostic Nutritional Index (PNI) <40, while Group H had a PNI ≥40. The five graphs show the subscales of KOOS. The KOOS-pain score in Group H was significantly higher than that in Group L at 12 and 36 months. Additionally, the KOOS-symptoms score was significantly higher in Group H than that in Group L at 36 months. *Significant difference between Group L and Group H (P<0.05). ADL, activities of daily living; QOL, quality of life.
Fig. 3.
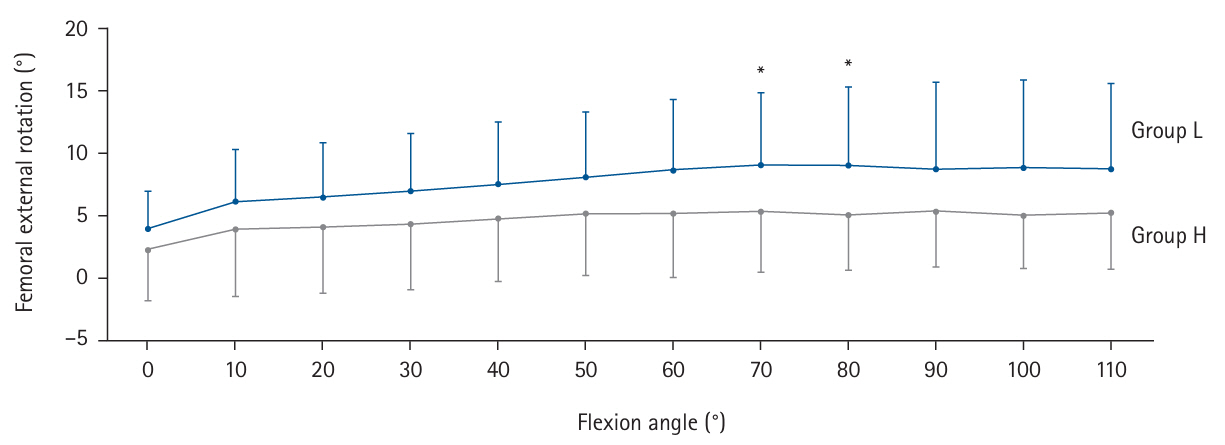
Kinematic comparison between Groups L and H with respect to axial rotation. Group L had a Prognostic Nutritional Index (PNI) <40, while Group H had a PNI ≥40. *P<0.05.
Fig. 4.
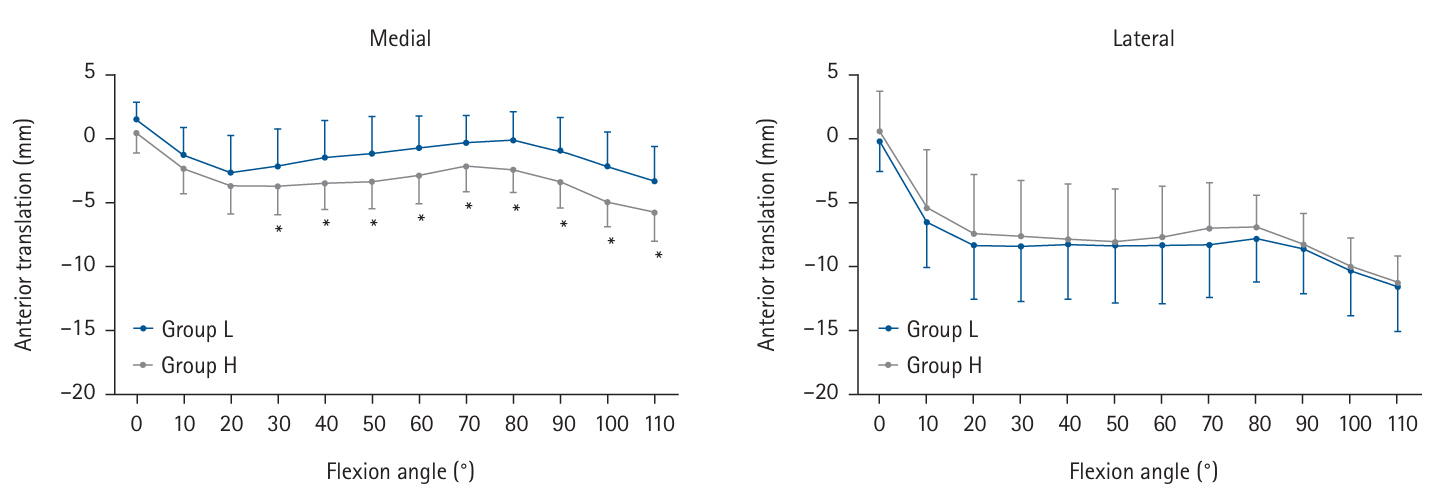
Kinematic comparison between Groups L and H regarding medial and lateral anteroposterior translation. Group L had a Prognostic Nutritional Index (PNI) <40, while Group H had a PNI ≥40. *Significant difference between Groups L and H (P<0.05).
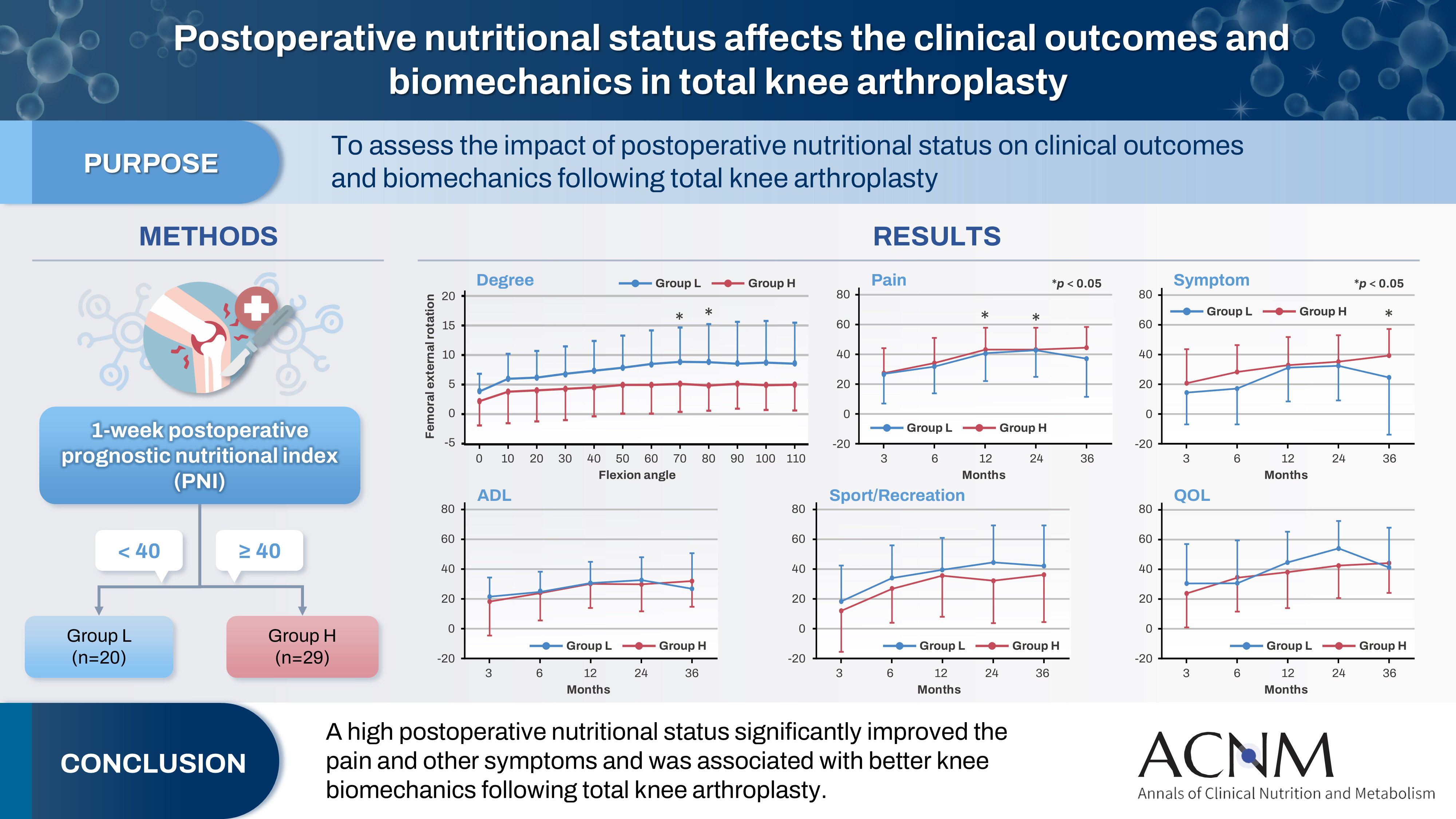
Table 1.
Knee Injury and Osteoarthritis Outcome Score (KOOS)
Table 2.
Patient characteristics of the two groups
- 1. Kim HK, Suzuki T, Saito K, Yoshida H, Kobayashi H, Kato H, et al. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: a randomized controlled trial. J Am Geriatr Soc 2012;60:16-23. ArticlePubMed
- 2. Papadopoulou SK, Papadimitriou K, Voulgaridou G, Georgaki E, Tsotidou E, Zantidou O, et al. Exercise and nutrition impact on osteoporosis and sarcopenia: the incidence of osteosarcopenia: a narrative review. Nutrients 2021;13:4499.ArticlePubMedPMC
- 3. Christensen JC, Mizner RL, Foreman KB, Marcus RL, Pelt CE, LaStayo PC. Quadriceps weakness preferentially predicts detrimental gait compensations among common impairments after total knee arthroplasty. J Orthop Res 2018;36:2355-63. ArticlePubMedPDF
- 4. Greene KA, Schurman JR. Quadriceps muscle function in primary total knee arthroplasty. J Arthroplasty 2008;23(7 Suppl):15-9. Article
- 5. Van Onsem S, Verstraete M, Van Eenoo W, Van Der Straeten C, Victor J. Are TKA kinematics during closed kinetic chain exercises associated with patient-reported outcomes? A preliminary analysis. Clin Orthop Relat Res 2020;478:255-63. ArticlePubMedPMC
- 6. Kono K, Inui H, Tomita T, Yamazaki T, Taketomi S, Yamagami R, et al. The higher patient-reported outcome measure group had smaller external rotation of the femur in bicruciate-stabilized total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2022;30:1292-9. ArticlePubMedPDF
- 7. Banks SA, Catani F, Deckard ER, Mahoney OM, Matsuda S, Meneghini RM, et al. Total knee arthroplasty kinematics predict patient-reported outcome measures: implications for clinical kinematic examinations. J Arthroplasty 2024;39(8S1):S224-9. Article
- 8. Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984;85:1001-5. PubMed
- 9. Cederholm T, Jensen GL, Correia MI, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. Clin Nutr 2019;38:1-9. ArticlePubMed
- 10. Cederholm T, Jensen GL, Correia MI, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. J Cachexia Sarcopenia Muscle 2019;10:207-17. ArticlePubMedPMCPDF
- 11. Jensen GL, Cederholm T, Correia MI, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. JPEN J Parenter Enteral Nutr 2019;43:32-40. ArticlePubMed
- 12. Tanemura A, Mizuno S, Hayasaki A, Gyoten K, Fujii T, Iizawa Y, et al. Onodera's prognostic nutritional index is a strong prognostic indicator for patients with hepatocellular carcinoma after initial hepatectomy, especially patients with preserved liver function. BMC Surg 2020;20:261.ArticlePubMedPMCPDF
- 13. Ren W, Wang H, Xiang T, Liu G. Prognostic role of preoperative Onodera's Prognostic Nutritional Index (OPNI) in gastrointestinal stromal tumors: a systematic review and meta-analysis. J Gastrointest Cancer 2023;54:731-8. ArticlePubMedPDF
- 14. Walsh SR, Cook EJ, Goulder F, Justin TA, Keeling NJ. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J Surg Oncol 2005;91:181-4. ArticlePubMed
- 15. Inui H, Taketomi S, Nakamura K, Sanada T, Tanaka S, Nakagawa T. An additional reference axis improves femoral rotation alignment in image-free computer navigation assisted total knee arthroplasty. J Arthroplasty 2013;28:766-71. ArticlePubMed
- 16. Kawaguchi K, Inui H, Yamagami R, Kenichi K, Sameshima S, Kage T, et al. A new technique for determining the rotational alignment of the tibial component during total knee arthroplasty. Knee 2021;29:323-31. ArticlePubMed
- 17. Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes 2003;1:64.ArticlePubMedPMC
- 18. Yamazaki T, Watanabe T, Nakajima Y, Sugamoto K, Tomita T, Yoshikawa H, et al. Improvement of depth position in 2-D/3-D registration of knee implants using single-plane fluoroscopy. IEEE Trans Med Imaging 2004;23:602-12. ArticlePubMed
- 19. Yamazaki T, Watanabe T, Nakajima Y, Sugamoto K, Tomita T, Maeda D, et al. Visualization of femorotibial contact in total knee arthroplasty using X-ray fluoroscopy. Eur J Radiol 2005;53:84-9. ArticlePubMed
- 20. Shimizu N, Tomita T, Yamazaki T, Yoshikawa H, Sugamoto K. The effect of weight-bearing condition on kinematics of a high-flexion, posterior-stabilized knee prosthesis. J Arthroplasty 2011;26:1031-7. ArticlePubMed
- 21. Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 1983;105:136-44. ArticlePubMedPDF
- 22. Kang H. Sample size determination for repeated measures design using G Power software. Anesth Pain Med 2015;10:6-15. Article
- 23. Tick H. Nutrition and pain. Phys Med Rehabil Clin N Am 2015;26:309-20. ArticlePubMed
- 24. Messina OD, Vidal Wilman M, Vidal Neira LF. Nutrition, osteoarthritis and cartilage metabolism. Aging Clin Exp Res 2019;31:807-13. ArticlePubMedPDF
- 25. Luyckx L, Luyckx T, Bellemans J, Victor J. Iliotibial band traction syndrome in guided motion TKA: a new clinical entity after TKA. Acta Orthop Belg 2010;76:507-12. PubMed
- 26. Yoshida T, Ebiko J, Sasaki K, Uchiyama E, Kura H. Recovery process of the muscle activities during walking with efficient early quadriceps training and gait exercises after total knee arthroplasty. J Bodyw Mov Ther 2022;29:49-53. ArticlePubMed
- 27. Armstrong R, Baltzopoulos V, Langan-Evans C, Clark D, Jarvis J, Stewart C, et al. An investigation of movement dynamics and muscle activity during traditional and accentuated-eccentric squatting. PLoS One 2022;17:e0276096.ArticlePubMedPMC
- 28. Kvarda P, Nuesch C, Egloff C, Appenzeller-Herzog C, Mundermann A, Ismailidis P. Hip abductor muscle strength in patients after total or unicompartmental knee arthroplasty for knee osteoarthritis or avascular necrosis: a systematic review and meta-analysis protocol. BMJ Open 2020;10:e038770.ArticlePubMedPMC
- 29. Arnout N, Victor J, Chevalier A, Bellemans J, Verstraete MA. Muscle loaded stability reflects ligament-based stability in TKA: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 2022;30:612-20. ArticlePubMedPDF
- 30. Kao DD, Ferrandino RM, Roof SA, Marshall DC, Khan MN, Chai RL, et al. Neutrophil-to-lymphocyte ratio as a predictor of surgical outcomes in head and neck cancer. Head Neck 2023;45:1903-12. ArticlePubMedPMC
- 31. Perry LA, Liu Z, Loth J, Penny-Dimri JC, Plummer M, Segal R, et al. Perioperative neutrophil-lymphocyte ratio predicts mortality after cardiac surgery: systematic review and meta-analysis. J Cardiothorac Vasc Anesth 2022;36:1296-303. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteImpact of postoperative nutritional status on the patients’ clinical outcomes and knee biomechanics following total knee arthroplasty in Japan: a prospective cohort study
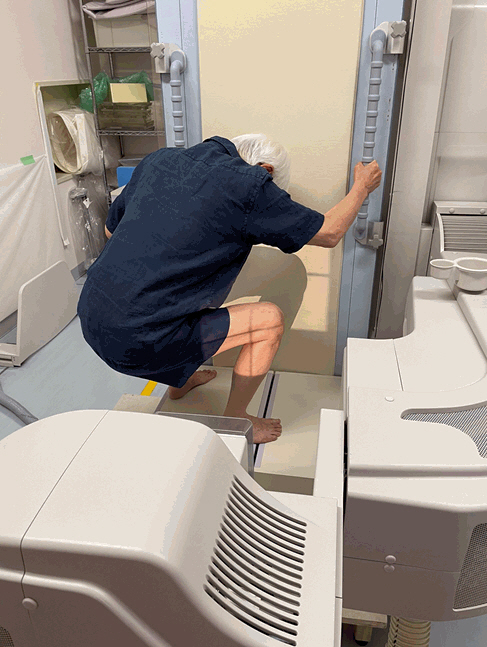
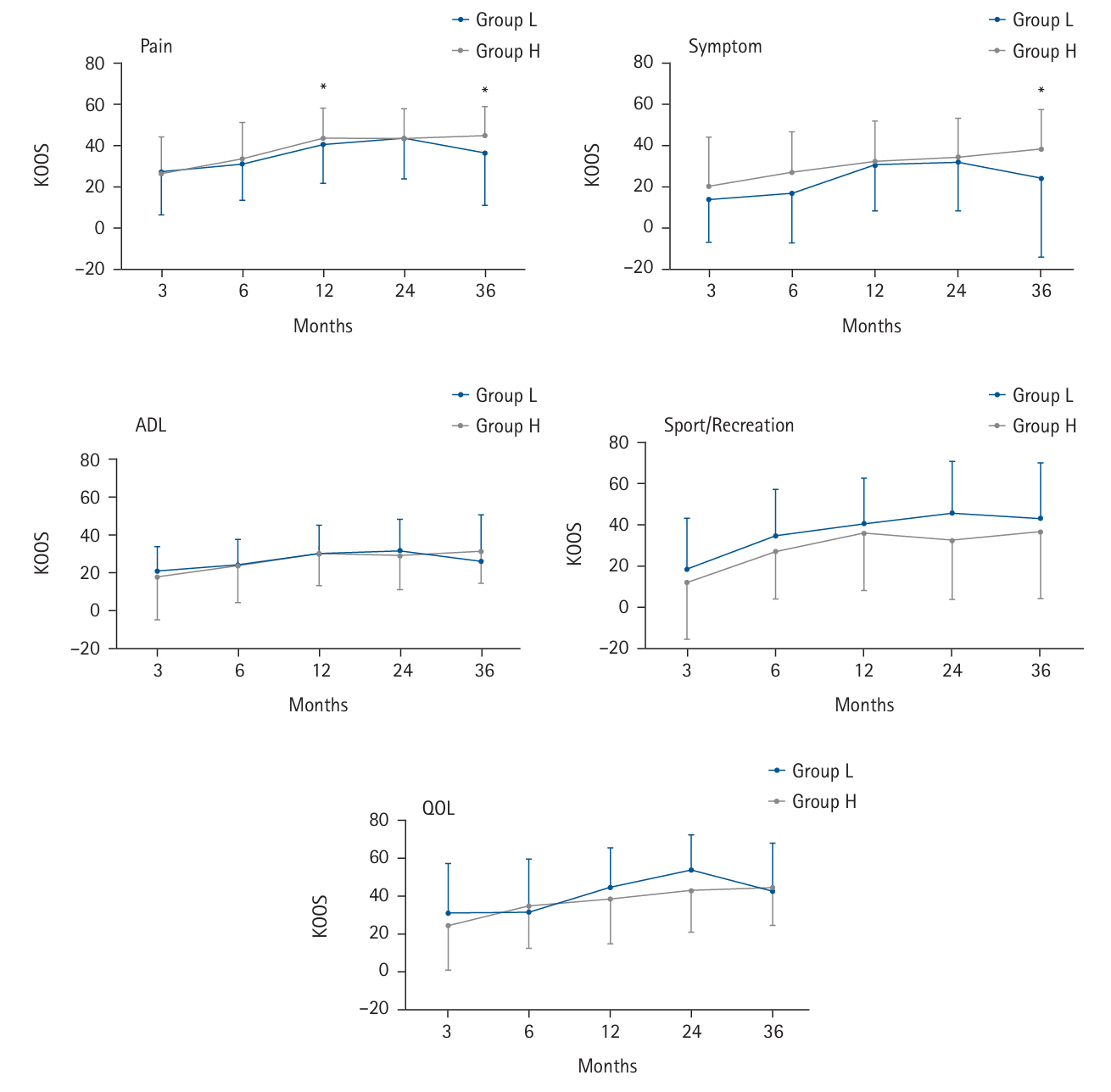
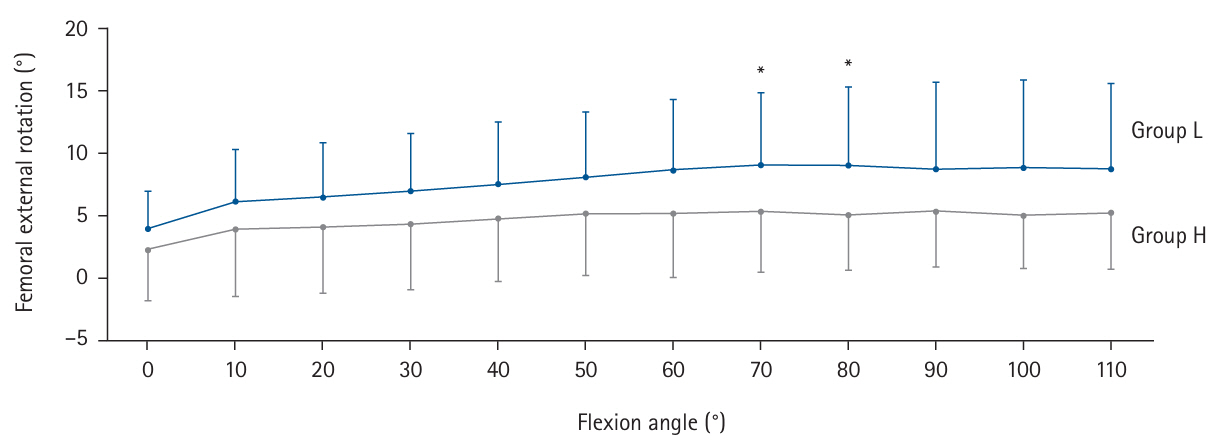
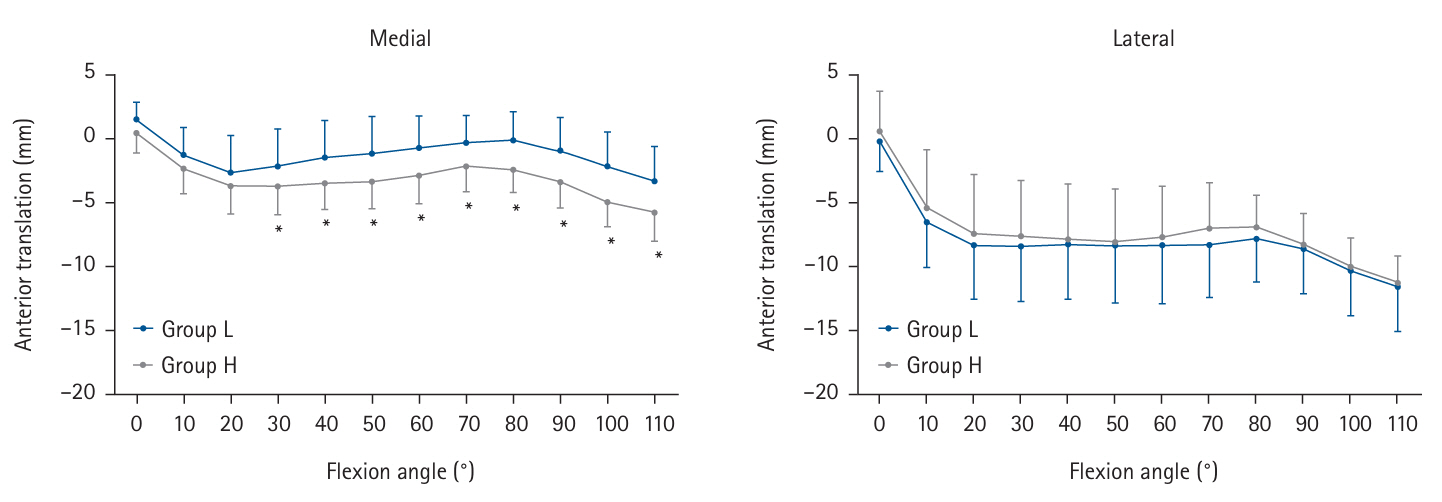
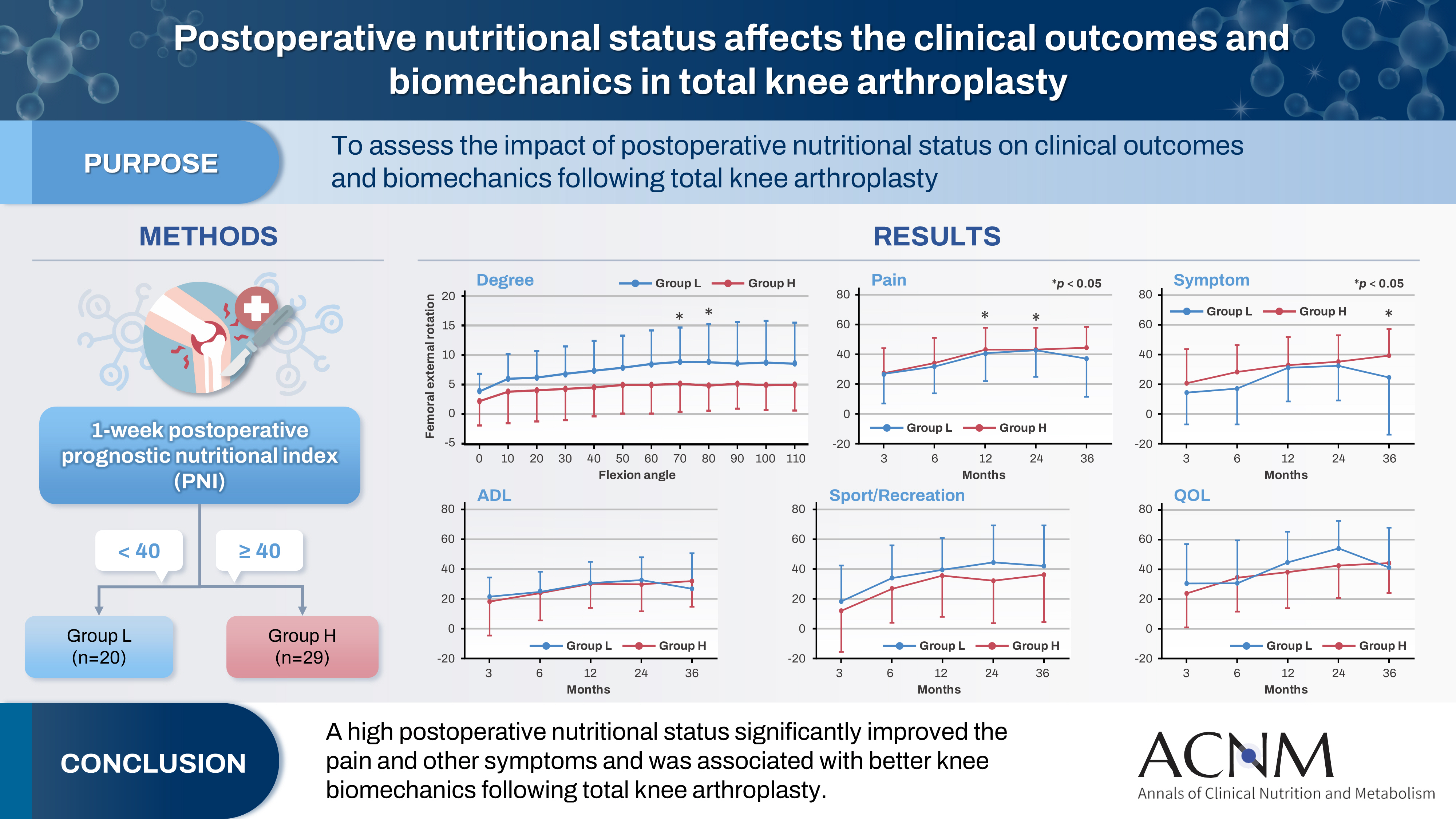
Fig. 1. Patient who could safely perform deep-standing squats after surgery for fluoroscopic analysis.
Fig. 2. Comparison of patient-reported outcome measures (Knee Injury and Osteoarthritis Outcome Score, KOOS) between Groups L and H. Group L had a Prognostic Nutritional Index (PNI) <40, while Group H had a PNI ≥40. The five graphs show the subscales of KOOS. The KOOS-pain score in Group H was significantly higher than that in Group L at 12 and 36 months. Additionally, the KOOS-symptoms score was significantly higher in Group H than that in Group L at 36 months. *Significant difference between Group L and Group H (P<0.05). ADL, activities of daily living; QOL, quality of life.
Fig. 3. Kinematic comparison between Groups L and H with respect to axial rotation. Group L had a Prognostic Nutritional Index (PNI) <40, while Group H had a PNI ≥40. *P<0.05.
Fig. 4. Kinematic comparison between Groups L and H regarding medial and lateral anteroposterior translation. Group L had a Prognostic Nutritional Index (PNI) <40, while Group H had a PNI ≥40. *Significant difference between Groups L and H (P<0.05).
Graphical abstract
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Graphical abstract
Impact of postoperative nutritional status on the patients’ clinical outcomes and knee biomechanics following total knee arthroplasty in Japan: a prospective cohort study
| Detailed information |
|---|
| The KOOS uses data on five knee-specific patient-centered outcomes: |
| (1) Pain |
| (2) Other symptoms such as swelling, restricted range of motion, and mechanical symptoms |
| (3) Disability at the level of activities of daily living (ADL) |
| (4) Disability at a level physically more demanding than ADL |
| (5) Mental and social aspects such as awareness and lifestyle changes |
| The KOOS is self-administered and filled out by the patient: |
| (1) The five patient-relevant subscales of KOOS are scored separately: Pain (9 items); Symptoms (7 items); ADL (17 items); Sport and Recreation (5 items); Quality of Life (4 items). |
| (2) A Likert scale is used, and all items have five possible answers scored from 0 (no problems) to 4 (extreme problems); each of the five scores is calculated as the sum of the items included. Scores are transformed to a 0–100 scale, with zero representing extreme knee problems and 100 representing no knee problems. |
| Variable | Group L (n=20) | Group H (n=29) | P-value |
|---|---|---|---|
| Age (yr) | 76.6±6.2 | 74.6±6.4 | 0.27 |
| Body mass index (kg/m2) | 26.7±3.4 | 26.7±4.3 | 0.81 |
| Fluoroscopic follow-up time (mo) | 15.0±7.8 | 12.4±7.5 | 0.06 |
| Sex (female:male) | 16:4 | 25:4 | 0.71 |
| WBC (/μL) | 6,830±1,661 | 6,424±1,367 | 0.42 |
| CRP (mg/L) | 5.7±3.2 | 3.8±3.7 | 0.01 |
| NLR | 4.3±2.1 | 2.7±1.1 | <0.01 |
Table 1. Knee Injury and Osteoarthritis Outcome Score (KOOS)
Table 2. Patient characteristics of the two groups
Values are presented as mean ±standard deviation. Group L had a prognostic nutritional index (PNI) <40, while Group H had a PNI ≥40. WBC, white blood cell count; CRP, C-reactive protein; NLR, neutrophil-to-lymphocyte ratio.

