 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 16(3); 2024 > Article
- Original article Micronutrient deficiencies in copper, zinc, and vitamin D as predictors of clinical outcomes in critically ill surgical patients in Korea: a retrospective cohort study
-
Jiae Kim1
 , Yanghee Jun2, Ye Rim Chang2, Jong-Kwan Baek2, Hak-Jae Lee2, Hyewon Han1, Suk-Kyung Hong2
, Yanghee Jun2, Ye Rim Chang2, Jong-Kwan Baek2, Hak-Jae Lee2, Hyewon Han1, Suk-Kyung Hong2 -
Annals of Clinical Nutrition and Metabolism 2024;16(3):158-167.
DOI: https://doi.org/10.15747/ACNM.2024.16.3.158
Published online: December 1, 2024
1Department of Pharmacy, Asan Medical Center, Seoul, Korea
2Department of Acute Care Surgery, Asan Medical Center, Seoul, Korea
- Corresponding author: Jiae Kim, email: liberty062@gmail.com
• Received: November 12, 2024 • Revised: November 24, 2024 • Accepted: November 24, 2024
© 2024 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 9,674 Views
- 94 Download
Abstract
-
Purpose To investigate the prevalence of copper, zinc, and vitamin D deficiencies in surgical intensive care unit (SICU) patients and the associations between those deficiencies and clinical outcomes.
-
Methods We conducted a retrospective study of 210 patients admitted to the SICU of Asan Medical Center between June 2020 and June 2022. Micronutrient levels were measured within 7 days of SICU admission. Primary outcomes were the mortality rate, length of SICU stay, hospital stay duration, and mechanical ventilation duration.
-
Results Copper deficiency was found in 35% (68/193), zinc deficiency in 52% (100/193), and severe vitamin D deficiency in 46% (82/179) of patients. Copper-deficient patients showed a significantly higher mortality rate (25.0% vs. 12.8%, P=0.044), longer hospital stays (57.8±47.0 vs. 45.2±36.6 days, P=0.041), and extended mechanical ventilation duration (26.9±23.3 vs. 18.8±15.7 days, P=0.012). Zinc deficiency was associated with higher C-reactive protein levels (16.2±9.5 vs. 11.5±8.8 mg/dL, P=0.001) and lower prealbumin levels (6.5±2.8 vs. 9.9±5.6 mg/dL, P<0.001). Severe vitamin D deficiency (<10 ng/mL) was not significantly associated with mortality or other clinical outcomes (mortality <10 ng/mL vs. ≥10 ng/mL, 13% vs. 18%, P=0.583).
-
Conclusion Micronutrient deficiencies are prevalent in SICU patients. Copper deficiency significantly correlated with poor clinical outcomes, and zinc deficiency showed a strong association with inflammatory markers. Early assessment and supplementation of micronutrients could be beneficial for critically ill surgical patients.
Introduction
Micronutrient requirements are relatively elevated in critically ill patients, who not only have a higher prevalence of malnutrition but also an increased need for nutrients to support recovery [1]. In critically ill surgical patients, trace elements become particularly important due to several factors: increased metabolic demands during critical illness [2], potential losses through surgical wounds and drainage [3], decreased absorption due to gastrointestinal dysfunction [4], and altered distribution due to inflammatory responses [5].
Copper serves as a crucial cofactor in various enzymatic processes, including antioxidant defense through Cu/Zn-superoxide dismutase, collagen formation via lysyl oxidase, and immune system function [6]. In surgical patients, adequate copper status is essential for wound healing, immune response, and protection against oxidative stress. Recent studies have shown that copper deficiency is associated with increased mortality and infection rates in patients with advanced liver disease [7] and adverse outcomes in critically ill patients with coronavirus disease 2019 (COVID-19) [8]. Zinc is fundamental for proper immune function, wound healing, and protein synthesis [9]. It acts as a cofactor for more than 300 enzymes and plays a vital role in maintaining the integrity of both innate and adaptive immunity [10,11]. Selenium, as a component of selenoproteins, is essential for antioxidant defense and immune function [12]. Manganese, although less studied than other trace elements, is crucial for wound healing and immune function through its role in superoxide dismutase and various metabolic processes [13]. However, manganese deficiency is relatively rare in Korean populations [14].
Vitamin D is also an essential micronutrient that plays important roles in immune function and inflammation [15]. Several studies have reported associations between vitamin D deficiency and poor clinical outcomes—including increased COVID-19-related mortality and increased lengths of stay in surgical intensive care units (SICUs) [16,17]. However, the therapeutic benefit of vitamin D supplementation in critically ill patients remains controversial. A landmark randomized controlled trial (VITdAL-ICU) showed that high-dose vitamin D3 supplementation did not improve hospital length of stay or overall mortality rates in critically ill patients, although some benefits were observed in the severe vitamin D deficiency subgroup (≤12 ng/mL) [18].
Our aim in this study was to investigate the prevalence of deficiencies in key micronutrients—copper (Cu), zinc (Zn), and vitamin D—and assess the clinical impact of those deficiencies on the outcomes of patients in the SICU [14].
Methods
The study was approved by the Institutional Review Board of Asan Medical Center (IRB No. 2023-1414). Due to the retrospective nature of this study, the requirement for informed patient consent was waived.
It is a retrospective cohort study. It was described according to the STOBE statement, which is available at: https://www.strobe-statement.org/
This retrospective cohort study was conducted at the SICU of Asan Medical Center, Seoul, from June 2020 to June 2022.
Nutritional support protocol
Standard nutritional support in our SICU follows a stepwise protocol. After hemodynamic stabilization, enteral nutrition is initiated within 24 hours of admission unless contraindicated (e.g., gastrointestinal perforation, obstruction, or bleeding). Enteral feeding starts at 20 mL/h using a fiber-free ready-to-hang formula, with continuous feeding through 24 hours. The feeding rate is increased by 10 mL/h every 12 hours or 20 mL/h every 24 hours. The target caloric requirement is set at 20 kcal/kg/d.
Supplemental parenteral nutrition is initiated if enteral intake fails to reach 60% of the target caloric requirement by day 7 in well-nourished patients or by day 3 in malnourished patients. Additional protein supplementation is provided using amino acid solutions (50 g/500 mL): daily when caloric intake exceeds 20 kcal/kg/d and every other day when caloric intake is below 20 kcal/kg/d. Special considerations are made for patients with renal or hepatic dysfunction.
For patients who showed micronutrient deficiencies in their initial laboratory tests, supplementation was provided through intravenous trace element preparations that follow the American Society for Parenteral and Enteral Nutrition (ASPEN)/ESPEN guidelines.
We included patients aged 18 years or older who had at least one measurement of copper, zinc, or vitamin D levels within 7 days of ICU admission. Among the 383 patients screened for eligibility, 210 patients who had at least one measured value for copper, zinc, or vitamin D within 7 days of ICU admission were included in the final analysis (Fig. 1).
The primary outcomes were the mortality rate, 30-day mortality, length of ICU stay, hospital length of stay, and duration of mechanical ventilation. Additional comparisons between the deficient and normal groups considered laboratory values (C-reactive protein [CRP], prealbumin) and nutritional status. We also analyzed the relationships among micronutrient levels and their associations with CRP.
The following data were collected through a retrospective review of electronic medical records: demographic and clinical characteristics (age, sex, and ICU admission diagnosis); micronutrient levels (copper, zinc, and vitamin D) within 7 days of ICU admission; CRP as an inflammatory marker; and prealbumin as a specific nutritional biomarker.
Blood samples were obtained via arterial lines for the micronutrient analysis. Our ICU protocol requires the measurement of copper, zinc, and vitamin D levels as part of the initial nutritional assessment for all patients, but only measurements taken within 7 days of ICU admission were included in this study. Due to this time constraint, some patients had missing vitamin D values, resulting in different sample sizes for each micronutrient analysis (copper: n=193, zinc: n=193, vitamin D: n=179).
Micronutrient levels are measured weekly during ICU stays, but only the initial measurements (first measurement after ICU admission) were used for our outcome analysis. Serum copper and zinc levels were measured using inductively coupled plasma mass spectrometry at the Department of Laboratory Medicine, Asan Medical Center. Vitamin D (25-hydroxyvitamin D) levels were measured using a radioimmunoassay.
Micronutrient deficiencies were defined based on laboratory reference ranges (Green Cross Laboratories reference values) and European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines [19]: zinc (66–110 g/dL), copper (76.4–145.0 g/dL). Deficiency was defined as any value below the lower limit of those ranges. For vitamin D, given the high prevalence of deficiency in our critically ill patient population, we used a cut-off value of 10 ng/mL to define severe deficiency, which allowed us to evaluate the clinical impact of profound vitamin D deficiency in this population.
Upon ICU admission, nutritional status was assessed by a dietitian according to the ASPEN criteria [20], which considers six characteristics: insufficient energy intake, weight loss, loss of muscle mass, loss of subcutaneous fat, fluid accumulation, and diminished functional status as measured by handgrip strength. The presence of two or more characteristics classifies a patient as malnourished. In this study, patients who met the criteria for moderate malnutrition or severe malnutrition were all classified as malnourished.
Because all target subjects were included, there is no selection bias.
No sample size estimation was required, since all target subjects were included.
Laboratory parameters (copper, zinc, vitamin D, CRP, and prealbumin) and clinical parameters (length of hospital stay, ICU stay duration, mechanical ventilation duration) are presented as mean±standard deviation and were analyzed using Student’s t-test. Categorical variables (mortality, nutritional status assessments) are presented as numbers with percentages and were analyzed using the chi-square test. Statistical significance was set at P<0.05. All statistical analyses were performed using IBM SPSS Statistics version 21.0 (IBM Corp.).
Results
Of the 383 patients screened for eligibility, 210 patients who had at least one measured value for copper, zinc, or vitamin D within 7 days of ICU admission were included in this study (Table 1). The mean age of the study population was 67.9±12.6 years (range, 19–91 years), and 64% were male. The mean length of hospital stay was 48.3±39.9 days (range, 8–235 days), and the mean length of ICU stay was 23.5±22.3 days (range, 6–189 days). The mean duration of mechanical ventilation was 21.1±18.6 days (range, 0–92 days). The overall mortality rate was 16% (34 patients), with 30-day mortality at 10% (21 patients).
The most common ICU admission diagnoses were cancer (38%), peritonitis (25%; caused by bowel ischemia, perforation, obstruction, and intra-abdominal abscess), trauma (8%), abdominal aortic aneurysm (AAA) (7%), and transplantation (5%). Miscellaneous conditions accounted for 24% of admissions and included pneumonia, Fournier’s gangrene, and necrotizing pancreatitis. Regarding nutritional status, 81% (151/186) of the patients were classified as malnourished according to the ASPEN criteria, with both moderate and severe malnutrition included in this category.
The prevalence of micronutrient deficiencies was notable: 35% (68/193) of patients were copper deficient, 52% (100/193) had zinc deficiency, and 46% (82/179) exhibited severe vitamin D deficiency (<10 ng/mL). The mean serum concentrations were 89.5±29.8 μg/dL for copper, 69.1±21.7 μg/dL for zinc, and 12.8±8.0 ng/mL for 25-(OH) vitamin D (Table 2).
Our analysis of the relationships among the micronutrients and inflammatory markers revealed several significant correlations (Fig. 2). The strongest correlation was observed between zinc levels and CRP, which showed a significant negative correlation (r=–0.281, P<0.01), indicating that higher CRP levels were associated with lower zinc concentrations.
Copper and CRP also had a negative correlation (r=–0.148), but it did not reach statistical significance (P=0.053). Zinc and copper levels showed a very weak positive correlation (r=0.029) that was not statistically significant (P=0.689).
When comparing baseline characteristics between the copper-deficient (n=68) and normal groups (n=125), age (66.1±14.4 vs. 69.8±11.0 years, P=0.071) and sex (male: 66% vs. 62%, P=0.193) were similar. The distribution of admission diagnoses was comparable between the groups: peritonitis (20 vs. 28 patients), cancer (28 vs. 48 patients), AAA (3 vs. 10 patients), transplantation (2 vs. 9 patients), trauma (5 vs. 10 patients), and miscellaneous conditions (14 vs. 26 patients), with no significant differences in any disease category (Table 3).
Copper-deficient patients (n=68) showed significantly poorer clinical outcomes than those with normal copper levels (n=125; Table 3). The overall mortality rate was significantly higher in the copper-deficient group (25.0% vs. 12.8%, P=0.044), although 30-day mortality rates were similar between groups (8.8% vs. 10.4%, P=0.805).
Hospital length of stay was significantly longer in copper-deficient patients (57.8±47.0 vs. 45.2±36.6 days, P=0.041), as was the duration of mechanical ventilation (26.9±23.3 vs. 18.8±15.7 days, P=0.012). ICU stay duration showed a trend toward being longer in the copper-deficient group, but the difference did not reach statistical significance (28.3±28.3 vs. 21.8±19.6 days, P=0.060).
Laboratory parameters showed some differences between groups, with vitamin D levels being significantly lower in copper-deficient patients (10.6±6.5 vs. 13.6±8.1 ng/mL, P=0.017). However, CRP (15.2±11.0 vs. 13.5±8.5 mg/dL, P=0.333), prealbumin (8.4±4.4 vs. 8.0±4.8 mg/dL, P=0.625), and zinc levels (70.3±28.2 vs. 68.4±17.4 μg/dL, P=0.597) did not differ significantly between the copper-deficient and copper-normal groups. Nutritional status was also similar between groups, with malnourished patients accounting for 86.9% vs. 79.8% (P=0.301) in the copper-deficient and normal groups, respectively.
The baseline characteristics comparison showed no significant differences between the zinc-deficient (n=100) and normal groups (n=93) in terms of age (69.3±11.9 vs. 67.6±12.9 years, P=0.794) and sex (male: 61% vs. 66%, P=0.191). However, the distribution of admission diagnoses showed some differences, with a significantly higher proportion of cancer patients in the zinc-deficient group (47 vs. 29 patients, P=0.03) and a trend toward fewer peritonitis cases (19 vs. 29 patients, P=0.07). Other admission diagnoses did not differ significantly between groups: AAA (9 vs. 4 patients), transplantation (3 vs. 8 patients), trauma (6 vs. 9 patients), and miscellaneous conditions (21 vs. 19 patients).
Our analysis of outcomes based on zinc status revealed distinct patterns between the zinc-deficient (n=100) and normal zinc level (n=93) patients (Table 4). Unlike copper deficiency, zinc deficiency was not associated with an increased mortality rate; in fact, the mortality rate was lower in the zinc-deficient group, though the difference was not statistically significant (13% vs. 22%, P=0.129). Similarly, 30-day mortality did not differ significantly between groups (7% vs. 13%, P=0.227).
Length of ICU stay (25.78±23.7 vs. 22.3±22.0 days, P=0.289), hospital stay duration (50.4±37.2 vs. 60.5±121.6 days, P=0.429), and mechanical ventilation duration (22.8±21.5 vs. 20.4±16.1 days, P=0.379) showed no significant differences between groups.
However, zinc deficiency showed significant associations with inflammatory and nutritional markers. Zinc-deficient patients had significantly higher CRP levels (16.2±9.5 vs. 11.5±8.8 mg/dL, P=0.001) and lower prealbumin levels (6.5±2.8 vs. 9.9±5.6 mg/dL, P<0.001) than patients with normal zinc levels. Neither copper levels (86.3±26.6 vs. 92.9±32.9 μg/dL, P=0.132), nor 25-(OH) vitamin D levels (12.2±8.8 vs. 13.1±6.3 ng/mL, P=0.420) differed significantly between the zinc groups. Nutritional status distribution was similar between groups, with malnourished patients accounting for 80% vs. 85% (P=0.553) in the zinc-deficient and normal groups, respectively.
Baseline characteristics were similar between the severe vitamin D deficiency (<10 ng/mL, n=82) and non-severe groups (≥10 ng/mL, n=97), with no significant differences in age (65.4±13.2 vs. 69.7±11.5 years, P=0.087) or sex (male: 62% vs. 64%, P=0.639). The distribution of admission diagnoses was peritonitis (25 vs. 17 patients), cancer (36 vs. 32 patients), AAA (5 vs. 8 patients), transplantation (5 vs. 7 patients), trauma (8 vs. 6 patients), and miscellaneous conditions (22 vs. 18 patients), with no significant differences between groups.
The analysis of outcomes based on vitamin D status showed no significant differences between patients with severe deficiency (<10 ng/mL, n=82) and those with higher levels (≥10 ng/mL, n=97; Table 5). Mortality rates were 13% vs. 18% (P=0.583), and the 30-day mortality rates were 4.9% vs. 11.3% (P=0.176) in the severe deficiency and higher level groups, respectively.
Length of ICU stay (23.7±17.5 vs. 21.9±22.7 days, P=0.560), hospital stay duration (52.8±44.1 vs. 43.2±34.8 days, P=0.115), and mechanical ventilation duration (23.4±20.2 vs. 18.4±15.4 days, P=0.065) showed no statistically significant differences between the groups, either.
Additional laboratory parameters were also similar between groups: CRP (14.7±9.3 vs. 12.9±8.3 mg/dL, P=0.212) and prealbumin (7.7±4.1 vs. 8.5±4.7 mg/dL, P=0.243). The vitamin D groups did not differ significantly in zinc (66.7±24.2 vs. 71.4±18.8 μg/dL, P=0.172) or copper levels (88.2±32.5 vs. 94.9±26.7 μg/dL, P=0.147). The nutritional status distribution was also similar, with malnourished patients accounting for 78% vs. 80% (P=0.844) in the severe deficiency and higher level groups, respectively.
Discussion
Our study reveals several significant findings about micronutrient deficiencies in SICU patients. The high prevalence of deficiencies—copper (35%), zinc (52%), and vitamin D (46%)—emphasizes the critical importance of monitoring micronutrient status in critically ill surgical patients. Among those deficiencies, copper deficiency demonstrated the strongest association with adverse clinical outcomes.
The significant association between copper deficiency and increased mortality rates (25.0% vs. 12.8%, P=0.044) in our study is particularly noteworthy and aligns with recent findings in various critical care settings [7,8]. The markedly higher mortality rate in copper-deficient patients suggests that copper plays a crucial role in critical illness outcomes. This association can be understood through copper’s essential roles in antioxidant defense, collagen formation, and immune function. The prolonged hospital stays (57.8 vs. 45.2 days, P=0.041) and extended mechanical ventilation duration (26.9 vs. 18.8 days, P=0.012) in copper-deficient patients further emphasize the potential impact of copper status on recovery from critical illness. In surgical patients specifically, copper’s role in wound healing and infection prevention could be crucial during the post-operative period.
The relationship between zinc deficiency and clinical outcomes showed a distinct and intriguing pattern. Although zinc deficiency was not associated with the mortality rate or length of stay, it demonstrated significant associations with inflammatory and nutritional markers. The strong negative correlation between zinc levels and CRP (r=–0.281, P<0.01) provides important insights into zinc’s role in inflammation regulation. This finding aligns with zinc’s known functions in immune modulation and inflammatory response [10,11]. The notably lower prealbumin levels in zinc-deficient patients (6.5 vs. 9.9 mg/dL, P<0.001) suggest a close relationship between zinc status and overall nutritional status. The relationships among zinc status, inflammation, and nutrition markers emphasize the importance of considering zinc monitoring as part of nutritional assessment in critically ill surgical patients.
The absence of significant associations between vitamin D deficiency and clinical outcomes in our study is interesting, especially given previous conflicting reports in the literature. This finding differs from some earlier studies [17] but aligns with the results of the VITdAL-ICU trial [18]. This discrepancy might reflect the complex role of vitamin D in critical illness, suggesting that acute vitamin D levels might not accurately reflect tissue-level vitamin D activity or that the relationship between vitamin D status and outcomes might be influenced by other factors not captured in our analysis.
Several mechanisms could contribute to the micronutrient deficiencies we found in SICU patients. These include increased metabolic demands during critical illness, potential losses through surgical wounds and drainage, decreased absorption due to gastrointestinal dysfunction, and altered distribution due to inflammatory responses [2-5]. The high prevalence of malnutrition (81%) in our study population, as defined by the ASPEN criteria, warrants particular attention and could be attributable to several factors. First, our SICU population included a large proportion of cancer patients (38%) who often present with pre-existing malnutrition. Second, the comprehensiveness of the ASPEN criteria, which include both biochemical and functional parameters, might capture subtle manifestations of malnutrition that other assessment tools miss. Third, critical illness itself, combined with surgical stress, likely contributes to a rapid deterioration of nutritional status.
Several limitations of our study should be acknowledged. First, as a single-center retrospective study, our findings might not be generalizable to all SICU populations. Second, we were unable to adjust for illness severity scores (such as APACHE II or SOFA scores) in our analysis, which could have provided important context for interpreting the relationship between micronutrient deficiencies and outcomes. Third, we faced several limitations with our micronutrient measurements: (a) the timing of measurements within the 7-day window might have influenced our results because the levels might fluctuate during critical illness; (b) we lacked data on pre-admission nutritional supplementation or dietary patterns, which could have affected baseline status; and (c) the single measurement point for each patient limits our understanding of how micronutrient levels change over the course of an ICU stay. Fourth, although we observed associations between micronutrient status and various outcomes, we cannot rule out the influence of unmeasured confounding factors, and thus cannot establish direct causality between micronutrient deficiencies and clinical outcomes. Fifth, we did not assess the impact of micronutrient supplementation on outcomes.
Future studies should address those limitations through: (1) prospective designs; (2) adjustment for illness severity scores; (3) serial measurements of micronutrient levels throughout the ICU stay; (4) collection of detailed pre-admission nutritional data; and (5) evaluation of the impact of standardized supplementation protocols. These approaches could establish causal relationships between micronutrient deficiencies and clinical outcomes in SICU patients.
Our findings suggest the need for an individualized approach to micronutrient management in SICU patients. The strong associations between copper deficiency and clinical outcomes and between zinc deficiency and inflammatory markers indicate that early screening and appropriate supplementation of these micronutrients might be beneficial. This is particularly relevant for copper, given its significant associations with the mortality rate and other key clinical outcomes.
Micronutrient deficiencies are prevalent in SICU patients, with copper deficiency significantly associated with poor clinical outcomes and zinc deficiency strongly correlated with inflammatory markers. These findings suggest that early assessment and supplementation of micronutrients could be beneficial in critically ill surgical patients. Further prospective studies are warranted to evaluate the efficacy of micronutrient supplementation at improving clinical outcomes.
Acknowledgments
None.
Authors’ contribution
Conceptualization: JK, SKH. Data curation: YJ. Formal analysis: JK. Funding acquisition: JK. Investigation: JK, YJ. Methodology: JK. Project administration: JKB, YRC, HJL. Supervision: SKH. Writing – original draft: JK, HH. Writing – review & editing: all authors.
Conflict of interest
Suk-Kyung Hong is the Editor-in-Chief and Hak-Jae Lee is an editorial board member of the journal; however, they were not involved in the review process of this manuscript. Otherwise, there is no conflict of interest to disclose.
Funding
This research was supported by a grant from the Korean Society for Parenteral and Enteral Nutrition (KSPEN).
Data availability
Contact the corresponding author for data availability.
Supplementary materials
None.
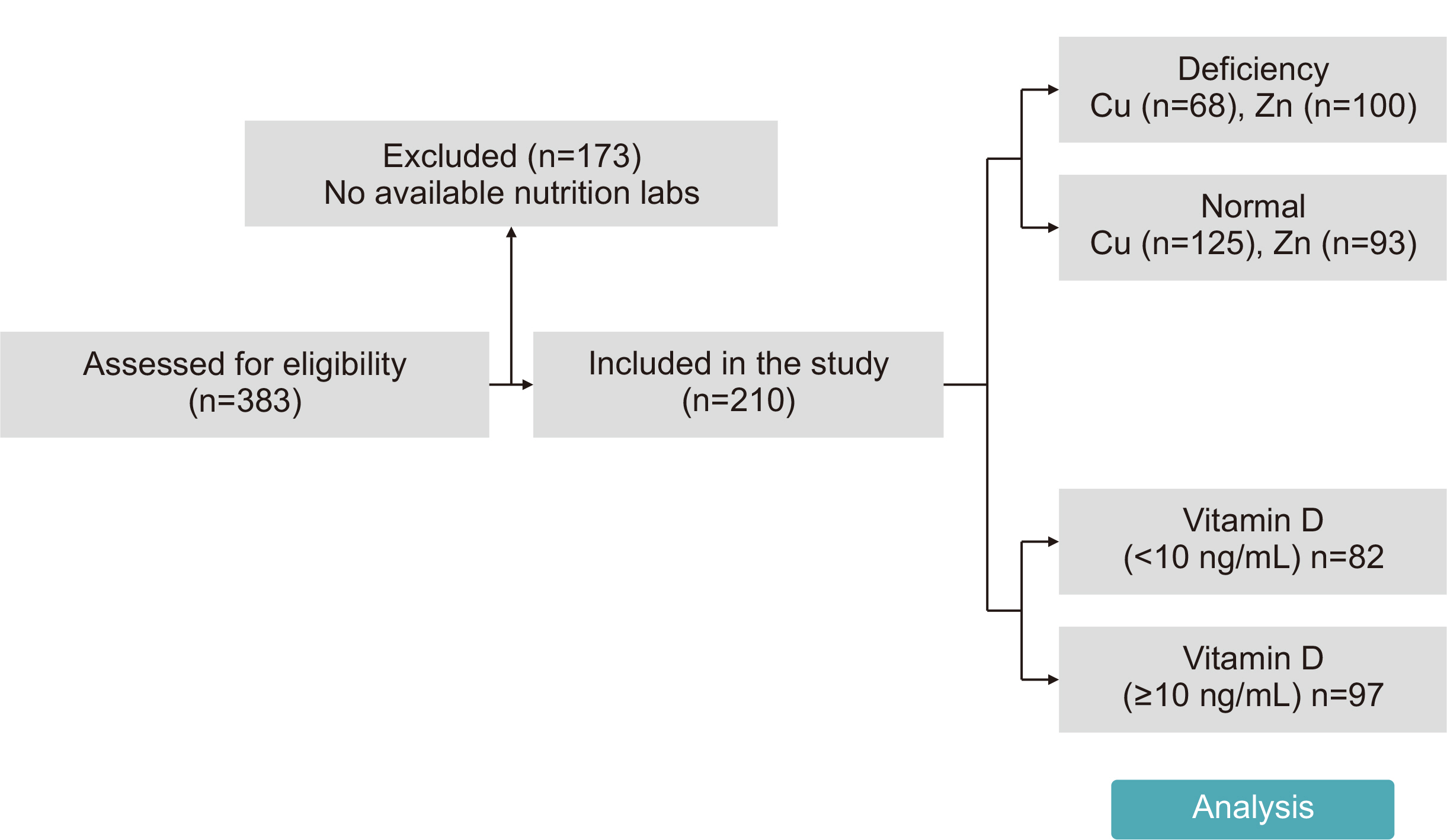
Fig. 2
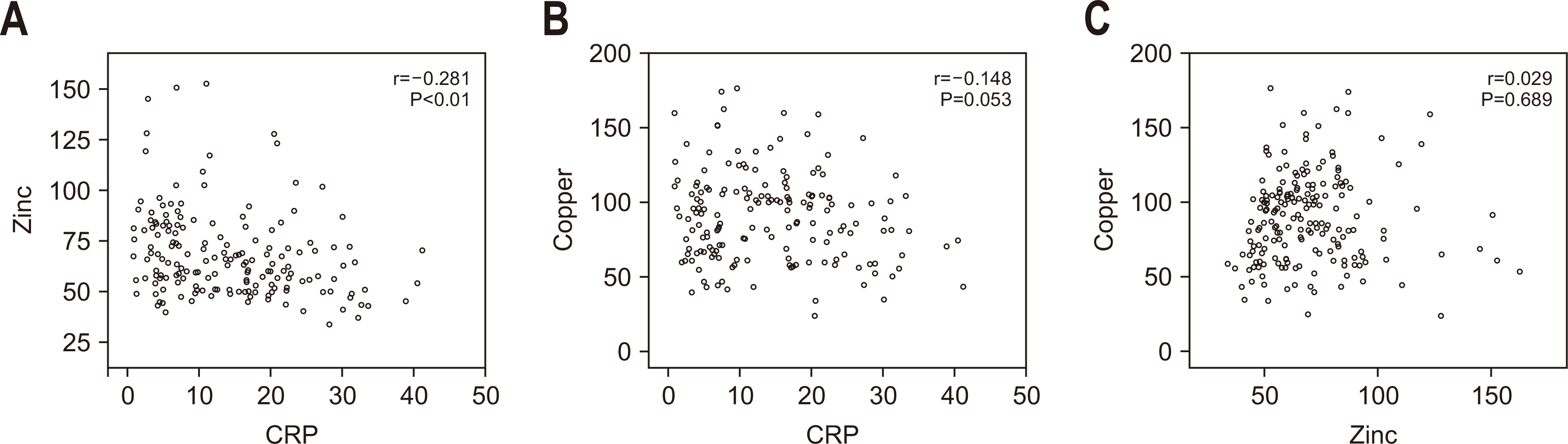
Correlations among zinc, copper, and C-reactive protein (CRP). (A) CRP and zinc: there is a significant negative correlation (r=–0.281, P<0.01). (B) CRP and copper: there is a negative correlation (r=–0.148), but it is not statistically significant (P=0.053). (C) Zinc and copper: there is a very weak positive correlation (r=0.029), but it is not statistically significant (P=0.689).
Table 1
Baseline characteristics of the study population
| Characteristic |
Value (n=210) |
|---|---|
| Age (yr) | 67.9±12.6 (19–91) |
| Sex, male (%) | 64 |
| Length of hospital stay (day) (n=209) | 48.3±39.9 (8–235) |
| Length of ICU stay (day) | 23.5±22.3 (6–189) |
| ICU admission diagnosis | |
| Peritonitis | 53 (25) |
| Cancer | 79 (38) |
| AAA | 14 (7) |
| Transplantation | 11 (5) |
| Trauma | 16 (8) |
| Miscellaneousa | 51 (24) |
| Mechanical ventilation (day) | 21.1±18.6 (0–92) |
| Mortality | 34 (16) |
| 30-Day mortality | 21 (10) |
| Nutritional statusb (n=186) | |
| Well nourished | 35 (19) |
| Malnourished | 151 (81) |
Values are presented as mean±standard deviation (range) or number (%).
ICU = intensive care unit; AAA = abdominal aortic aneurysm.
aPneumonia, Fournier’s gangrene, necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
bASPEN (American Society for Parenteral and Enteral Nutrition).
Table 2
Prevalence of micronutrient deficiencies in SICU patients (N=210)
| Micronutrient | Mean±SD level | Reference range |
Deficiency rate (%) (deficient [n]/atested [n]) |
|---|---|---|---|
| Copper (Cu) (μg/dL) | 89.5±29.8 | 76.4–145.0 | 35 (68/193) |
| Zinc (Zn) (μg/dL) | 69.1±21.7 | 66–110 | 52 (100/193) |
| 25-(OH) vitamin D (ng/mL) | 12.8±8.0 |
Deficiency<10.0 Insufficiency 10.0–30.0 Sufficiency 30.1–100.0 |
46 (82/179) |
Table 3
Comparison of clinical outcomes and baseline characteristics between copper-deficient and normal groups
| Copper | Low level (n=68) | Normal level (n=125) | P-value |
|---|---|---|---|
| Reference range 76.4–145.0 μg/dL | <76.4 μg/dL | 76.4–145.0 μg/dL | |
| Mortality | 17 (25.0) | 16 (12.8) | 0.044 |
| 30-Day mortality | 6 (8.8) | 13 (10.4) | 0.805 |
| ICU stay (day) | 28.3±28.3 | 21.8 ±19.6 | 0.060 |
| Hospital stay (day) | 57.8±47.0 | 45.2±36.6 | 0.041 |
| Mechanical ventilation (day) | 26.9±23.3 | 18.8±15.7 | 0.012 |
| Age (yr) | 66.1±14.4 | 69.8±11.0 | 0.071 |
| Sex, male (%) | 66 | 62 | 0.193 |
| ICU admission diagnosis | |||
| Peritonitis | 20 | 28 | 0.37 |
| Cancer | 28 | 48 | 0.82 |
| AAA | 3 | 10 | 0.55 |
| Transplantation | 2 | 9 | 0.33 |
| Trauma | 5 | 10 | >0.99 |
| Miscellaneousa | 14 | 26 | >0.99 |
| CRP (mg/dL) | 15.2±11.0 (n=58) | 13.5±8.5 (n=112) | 0.333 |
| Prealbumin (mg/dL) | 8.4±4.4 | 8.0±4.8 | 0.625 |
| Zinc (μg/dL) | 70.3±28.2 | 68.4±17.4 | 0.597 |
| Vitamin D (ng/mL) | 10.6±6.5 (n=52) | 13.6±8.1 (n=110) | 0.017 |
| Nutrition status | n=61 | n=114 | |
| Well nourished | 8 (13.1) | 23 (20.2) | 0.301 |
| Malnourished | 53 (86.9) | 91 (79.8) | 0.301 |
Values are presented as number (%), mean±standard deviation, or number only.
ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein.
aPneumonia, Fournier’s gangrene, necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Table 4
Comparison of clinical outcomes and baseline characteristics between zinc-deficient and normal groups
| Zinc | Low level (n=100) | Normal level (n=93) | P-value |
|---|---|---|---|
| Reference range 66–110 μg/dL | <66 μg/dL | 66–110 μg/dL | |
| Mortality | 13 (13) | 20 (22) | 0.129 |
| 30-Day mortality | 7 (7) | 12 (13) | 0.227 |
| ICU stay (day) | 25.78±23.7 | 22.3±22.0 | 0.289 |
| Hospital stay (day) | 50.4±37.2 | 60.5±121.6 (n=92) | 0.429 |
| Mechanical ventilation (day) | 22.8±21.5 | 20.4±16.1 | 0.379 |
| Age (yr) | 69.3±11.9 | 67.6±12.9 | 0.794 |
| Sex, male (%) | 61 | 66 | 0.191 |
| ICU admission diagnosis | |||
| Peritonitis | 19 | 29 | 0.07 |
| Cancer | 47 | 29 | 0.03 |
| AAA | 9 | 4 | 0.25 |
| Transplantation | 3 | 8 | 0.12 |
| Trauma | 6 | 9 | 0.42 |
| Miscellaneousa | 21 | 19 | >0.99 |
| CRP (mg/dL) | 16.2±9.5 (n=93) | 11.5±8.8 (n=77) | 0.001 |
| Prealbumin (mg/dL) | 6.5±2.8 | 9.9±5.6 | <0.001 |
| Copper (μg/dL) | 86.3±26.6 | 92.9±32.9 | 0.132 |
| Vitamin D (ng/mL) | 12.2±8.8 (n=83) | 13.1±6.3 (n=79) | 0.420 |
| Nutrition status | n=91 | n=84 | |
| Well nourished | 18 (20) | 13 (15) | 0.553 |
| Malnourished | 73 (80) | 71 (85) | 0.553 |
Values are presented as number (%), mean±standard deviation, or number only.
ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein.
aPneumonia, Fournier’s gangrene, Necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Table 5
Comparison of clinical outcomes and baseline characteristics between severe (<10 ng/mL) and non-severe (≥10 ng/mL) vitamin D deficiency groups
| Vitamin D | <10 (n=82) | ≥10 (n=97) | P-value |
|---|---|---|---|
| Mortality | 11 (13) | 17 (18) | 0.583 |
| 30-Day mortality | 4 (4.9) | 11 (11.3) | 0.176 |
| ICU stay (day) | 23.7±17.5 | 21.9±22.7 | 0.560 |
| Hospital stay (day) | 52.8±44.1 | 43.2±34.8 | 0.115 |
| Mechanical ventilation (day) | 23.4±20.2 | 18.4±15.4 | 0.065 |
| Age (yr) | 65.4±13.2 | 69.7±11.5 | 0.087 |
| Sex, male | 62 | 64 | 0.639 |
| ICU admission diagnosis | |||
| Peritonitis | 25 | 17 | 0.54 |
| Cancer | 36 | 32 | 0.91 |
| AAA | 5 | 8 | 0.37 |
| Transplantation | 5 | 7 | 0.54 |
| Trauma | 8 | 6 | >0.99 |
| Miscellaneousa | 22 | 18 | >0.99 |
| CRP (mg/dL) | 14.7±9.3 (n=79) | 12.9±8.3 (n=84) | 0.212 |
| Prealbumin (mg/dL) | 7.7±4.1 (n=82) | 8.5±4.7 (n=91) | 0.243 |
| Zinc (μg/dL) | 66.7±24.2 (n=75) | 71.4±18.8 (n=87) | 0.172 |
| Copper (ng/mL) | 88.2±32.5 (n=75) | 94.9±26.7 (n=87) | 0.147 |
| Nutrition status | n=72 | n=86 | |
| Well nourished | 16 (22) | 17 (20) | 0.844 |
| Malnourished | 56 (78) | 69 (80) | 0.844 |
Values are presented as number (%), mean±standard deviation, or number only.
ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein.
aPneumonia, Fournier’s gangrene, Necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
- 1. Berger MM, Pantet O, Schneider A, Ben-Hamouda N. Micronutrient deficiencies in medical and surgical inpatients. J Clin Med 2019;8:931.ArticlePubMedPMC
- 2. Singer P, Blaser AR, Berger MM, Calder PC, Casaer M, Hiesmayr M, et al. ESPEN practical and partially revised guideline: clinical nutrition in the intensive care unit. Clin Nutr 2023;42:1671-89. ArticlePubMed
- 3. Agarwal A, Khanna P, Baidya DK, Arora MK. Trace elements in critical illness. J Endocrinol Metab 2011;1:57-63. Article
- 4. Btaiche IF, Chan LN, Pleva M, Kraft MD. Critical illness, gastrointestinal complications, and medication therapy during enteral feeding in critically ill adult patients. Nutr Clin Pract 2010;25:32-49. ArticlePubMedPDF
- 5. Duncan A, Talwar D, McMillan DC, Stefanowicz F, O'Reilly DS. Quantitative data on the magnitude of the systemic inflammatory response and its effect on micronutrient status based on plasma measurements. Am J Clin Nutr 2012;95:64-71. ArticlePubMed
- 6. Tapiero H, Townsend DM, Tew KD. Trace elements in human physiology and pathology. Copper. Biomed Pharmacother 2003;57:386-98. ArticlePubMedPMC
- 7. Yu L, Yousuf S, Yousuf S, Yeh J, Biggins SW, Morishima C, et al. Copper deficiency is an independent risk factor for mortality in patients with advanced liver disease. Hepatol Commun 2023;7:e0076. ArticlePubMedPMC
- 8. Hackler J, Heller RA, Sun Q, Schwarzer M, Diegmann J, Bachmann M, et al. 2021;Relation of serum copper status to survival in COVID-19. Nutrients 13:1898.ArticlePubMedPMC
- 9. Gammoh NZ, Rink L. Zinc in infection and inflammation. Nutrients 2017;9:624.ArticlePubMedPMC
- 10. Prasad AS. Discovery of human zinc deficiency: its impact on human health and disease. Adv Nutr 2013;4:176-90. ArticlePubMedPMC
- 11. Wessels I, Maywald M, Rink L. Zinc as a gatekeeper of im이대로 내도 mune function. Nutrients 2017;9:1286.ArticlePubMedPMC
- 12. Moghaddam A, Heller RA, Sun Q, Seelig J, Cherkezov A, Seibert L, et al. Selenium deficiency is associated with mortality risk from COVID-19. Nutrients 2020;12:2098.ArticlePubMedPMC
- 13. Aschner M, Erikson K. Manganese. Adv Nutr 2017;8:520-1. ArticlePubMedPMC
- 14. Lee YH, Bang ES, Lee JH, Lee JD, Kang DR, Hong J, et al. Serum concentrations of trace elements zinc, copper, selenium, and manganese in critically ill patients. Biol Trace Elem Res 2019;188:316-25. ArticlePubMedPDF
- 15. Charoenngam N, Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients 2020;12:2097. ArticlePubMedPMC
- 16. Kazemi A, Mohammadi V, Aghababaee SK, Golzarand M, Clark CCT, Babajafari S. 2021;Association of vitamin D status with SARS-CoV-2 infection or COVID-19 severity: a systematic review and meta-analysis. Adv Nutr 12:1636-58. ArticlePubMedPMCPDF
- 17. Matthews LR, Ahmed Y, Wilson KL, Griggs DD, Danner OK. Worsening severity of vitamin D deficiency is associated with increased length of stay, surgical intensive care unit cost, and mortality rate in surgical intensive care unit patients. Am J Surg 2012;204:37-43. ArticlePubMedPMC
- 18. Amrein K, Schnedl C, Holl A, Riedl R, Christopher KB, Pachler C, et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: the VITdAL-ICU randomized clinical trial. JAMA 2014;312:1520-30. ArticlePubMed
- 19. Berger MM, Shenkin A, Schweinlin A, Amrein K, Augsburger M, Biesalski HK, et al. ESPEN micronutrient guideline. Clin Nutr 2022;41:1357-424. PubMed
- 20. White JV, Guenter P, Jensen G, Malone A, Schofield M. Academy Malnutrition Work Group; A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J Parenter Enteral Nutr 2012;36:275-83. PubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
Cite- Figure
-
Micronutrient deficiencies in copper, zinc, and vitamin D as predictors of clinical outcomes in critically ill surgical patients in Korea: a retrospective cohort study
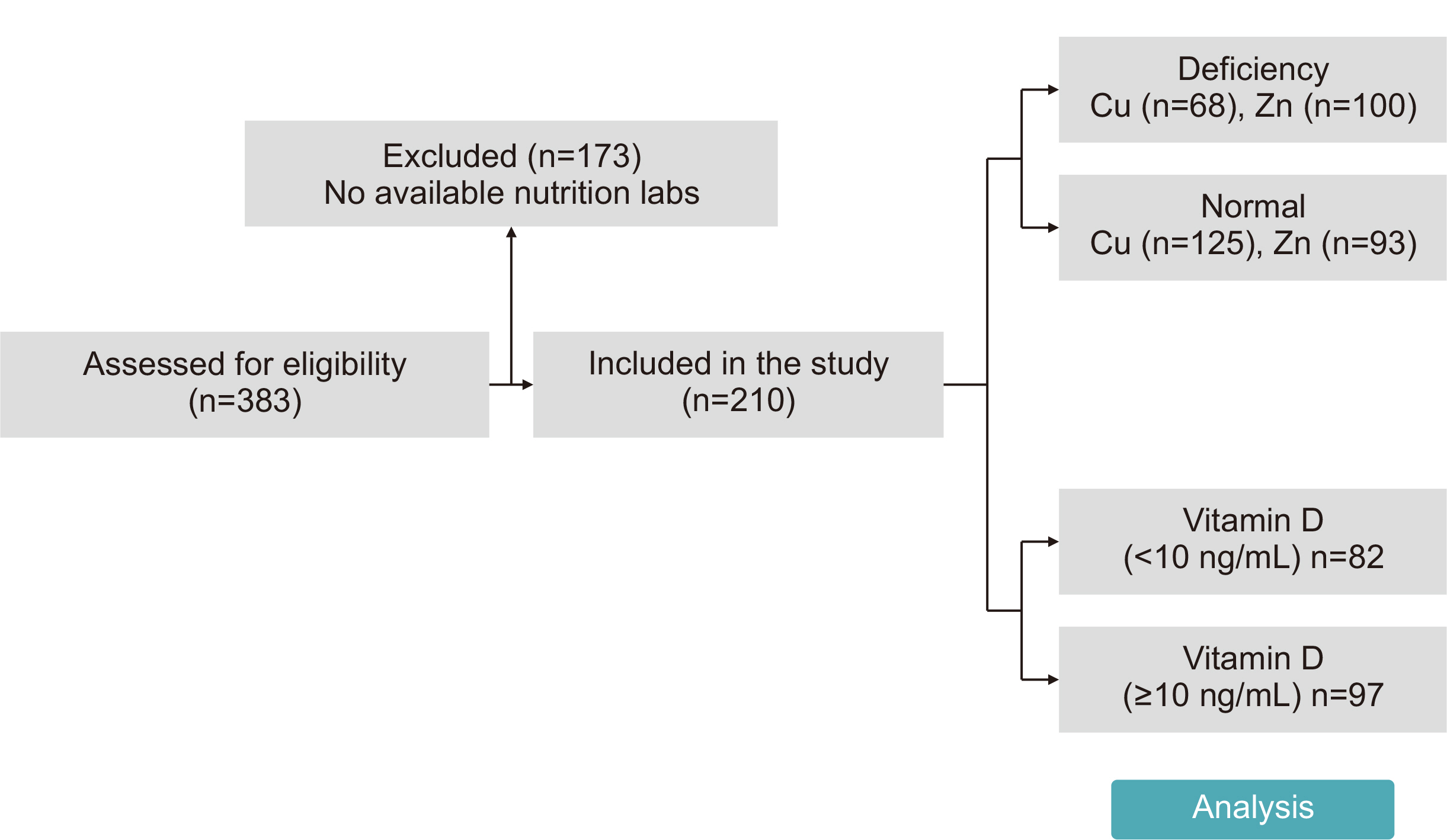
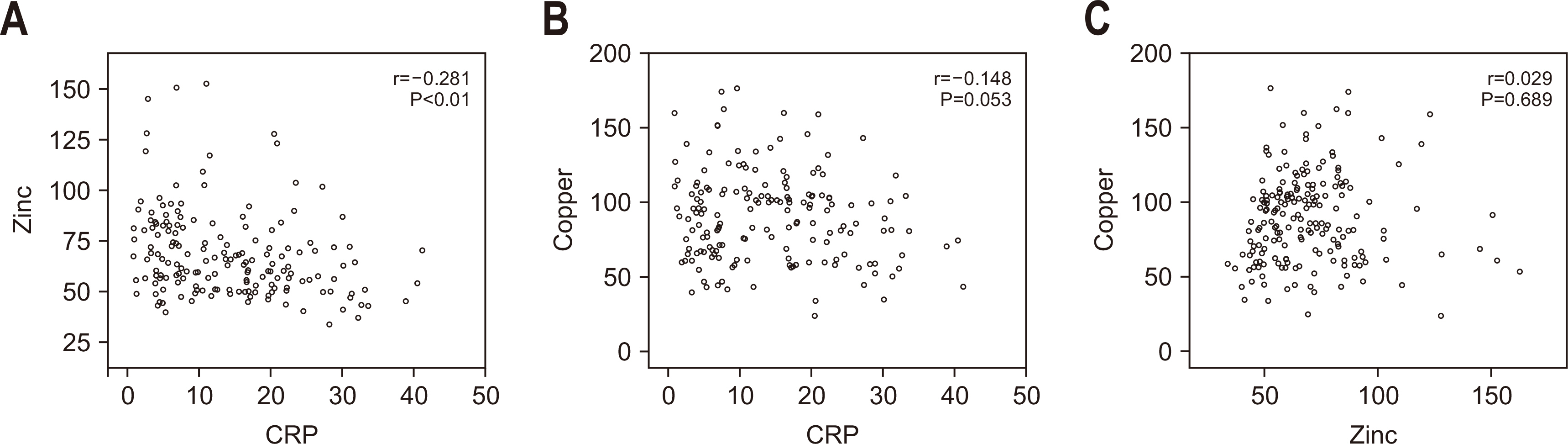
Fig. 1
Patient flow diagram.
Fig. 2
Correlations among zinc, copper, and C-reactive protein (CRP). (A) CRP and zinc: there is a significant negative correlation (r=–0.281, P<0.01). (B) CRP and copper: there is a negative correlation (r=–0.148), but it is not statistically significant (P=0.053). (C) Zinc and copper: there is a very weak positive correlation (r=0.029), but it is not statistically significant (P=0.689).
Fig. 1
Fig. 2
Micronutrient deficiencies in copper, zinc, and vitamin D as predictors of clinical outcomes in critically ill surgical patients in Korea: a retrospective cohort study
Baseline characteristics of the study population
| Characteristic | Value (n=210) |
|---|---|
| Age (yr) | 67.9±12.6 (19–91) |
| Sex, male (%) | 64 |
| Length of hospital stay (day) (n=209) | 48.3±39.9 (8–235) |
| Length of ICU stay (day) | 23.5±22.3 (6–189) |
| ICU admission diagnosis | |
| Peritonitis | 53 (25) |
| Cancer | 79 (38) |
| AAA | 14 (7) |
| Transplantation | 11 (5) |
| Trauma | 16 (8) |
| Miscellaneous |
51 (24) |
| Mechanical ventilation (day) | 21.1±18.6 (0–92) |
| Mortality | 34 (16) |
| 30-Day mortality | 21 (10) |
| Nutritional status |
|
| Well nourished | 35 (19) |
| Malnourished | 151 (81) |
Values are presented as mean±standard deviation (range) or number (%).
ICU = intensive care unit; AAA = abdominal aortic aneurysm.
aPneumonia, Fournier’s gangrene, necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
bASPEN (American Society for Parenteral and Enteral Nutrition).
Prevalence of micronutrient deficiencies in SICU patients (N=210)
| Micronutrient | Mean±SD level | Reference range | Deficiency rate (%) (deficient [n]/ |
|---|---|---|---|
| Copper (Cu) (μg/dL) | 89.5±29.8 | 76.4–145.0 | 35 (68/193) |
| Zinc (Zn) (μg/dL) | 69.1±21.7 | 66–110 | 52 (100/193) |
| 25-(OH) vitamin D (ng/mL) | 12.8±8.0 | Deficiency<10.0 Insufficiency 10.0–30.0 Sufficiency 30.1–100.0 |
46 (82/179) |
SICU = surgical intensive care unit; SD = standard deviation.
aOnly measurements performed within 7 days of ICU admission were included in the analysis.
Comparison of clinical outcomes and baseline characteristics between copper-deficient and normal groups
| Copper | Low level (n=68) | Normal level (n=125) | P-value |
|---|---|---|---|
| Reference range 76.4–145.0 μg/dL | <76.4 μg/dL | 76.4–145.0 μg/dL | |
| Mortality | 17 (25.0) | 16 (12.8) | 0.044 |
| 30-Day mortality | 6 (8.8) | 13 (10.4) | 0.805 |
| ICU stay (day) | 28.3±28.3 | 21.8 ±19.6 | 0.060 |
| Hospital stay (day) | 57.8±47.0 | 45.2±36.6 | 0.041 |
| Mechanical ventilation (day) | 26.9±23.3 | 18.8±15.7 | 0.012 |
| Age (yr) | 66.1±14.4 | 69.8±11.0 | 0.071 |
| Sex, male (%) | 66 | 62 | 0.193 |
| ICU admission diagnosis | |||
| Peritonitis | 20 | 28 | 0.37 |
| Cancer | 28 | 48 | 0.82 |
| AAA | 3 | 10 | 0.55 |
| Transplantation | 2 | 9 | 0.33 |
| Trauma | 5 | 10 | >0.99 |
| Miscellaneous |
14 | 26 | >0.99 |
| CRP (mg/dL) | 15.2±11.0 (n=58) | 13.5±8.5 (n=112) | 0.333 |
| Prealbumin (mg/dL) | 8.4±4.4 | 8.0±4.8 | 0.625 |
| Zinc (μg/dL) | 70.3±28.2 | 68.4±17.4 | 0.597 |
| Vitamin D (ng/mL) | 10.6±6.5 (n=52) | 13.6±8.1 (n=110) | 0.017 |
| Nutrition status | n=61 | n=114 | |
| Well nourished | 8 (13.1) | 23 (20.2) | 0.301 |
| Malnourished | 53 (86.9) | 91 (79.8) | 0.301 |
Values are presented as number (%), mean±standard deviation, or number only.
ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein.
aPneumonia, Fournier’s gangrene, necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Comparison of clinical outcomes and baseline characteristics between zinc-deficient and normal groups
| Zinc | Low level (n=100) | Normal level (n=93) | P-value |
|---|---|---|---|
| Reference range 66–110 μg/dL | <66 μg/dL | 66–110 μg/dL | |
| Mortality | 13 (13) | 20 (22) | 0.129 |
| 30-Day mortality | 7 (7) | 12 (13) | 0.227 |
| ICU stay (day) | 25.78±23.7 | 22.3±22.0 | 0.289 |
| Hospital stay (day) | 50.4±37.2 | 60.5±121.6 (n=92) | 0.429 |
| Mechanical ventilation (day) | 22.8±21.5 | 20.4±16.1 | 0.379 |
| Age (yr) | 69.3±11.9 | 67.6±12.9 | 0.794 |
| Sex, male (%) | 61 | 66 | 0.191 |
| ICU admission diagnosis | |||
| Peritonitis | 19 | 29 | 0.07 |
| Cancer | 47 | 29 | 0.03 |
| AAA | 9 | 4 | 0.25 |
| Transplantation | 3 | 8 | 0.12 |
| Trauma | 6 | 9 | 0.42 |
| Miscellaneous |
21 | 19 | >0.99 |
| CRP (mg/dL) | 16.2±9.5 (n=93) | 11.5±8.8 (n=77) | 0.001 |
| Prealbumin (mg/dL) | 6.5±2.8 | 9.9±5.6 | <0.001 |
| Copper (μg/dL) | 86.3±26.6 | 92.9±32.9 | 0.132 |
| Vitamin D (ng/mL) | 12.2±8.8 (n=83) | 13.1±6.3 (n=79) | 0.420 |
| Nutrition status | n=91 | n=84 | |
| Well nourished | 18 (20) | 13 (15) | 0.553 |
| Malnourished | 73 (80) | 71 (85) | 0.553 |
Values are presented as number (%), mean±standard deviation, or number only.
ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein.
aPneumonia, Fournier’s gangrene, Necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Comparison of clinical outcomes and baseline characteristics between severe (<10 ng/mL) and non-severe (≥10 ng/mL) vitamin D deficiency groups
| Vitamin D | <10 (n=82) | ≥10 (n=97) | P-value |
|---|---|---|---|
| Mortality | 11 (13) | 17 (18) | 0.583 |
| 30-Day mortality | 4 (4.9) | 11 (11.3) | 0.176 |
| ICU stay (day) | 23.7±17.5 | 21.9±22.7 | 0.560 |
| Hospital stay (day) | 52.8±44.1 | 43.2±34.8 | 0.115 |
| Mechanical ventilation (day) | 23.4±20.2 | 18.4±15.4 | 0.065 |
| Age (yr) | 65.4±13.2 | 69.7±11.5 | 0.087 |
| Sex, male | 62 | 64 | 0.639 |
| ICU admission diagnosis | |||
| Peritonitis | 25 | 17 | 0.54 |
| Cancer | 36 | 32 | 0.91 |
| AAA | 5 | 8 | 0.37 |
| Transplantation | 5 | 7 | 0.54 |
| Trauma | 8 | 6 | >0.99 |
| Miscellaneous |
22 | 18 | >0.99 |
| CRP (mg/dL) | 14.7±9.3 (n=79) | 12.9±8.3 (n=84) | 0.212 |
| Prealbumin (mg/dL) | 7.7±4.1 (n=82) | 8.5±4.7 (n=91) | 0.243 |
| Zinc (μg/dL) | 66.7±24.2 (n=75) | 71.4±18.8 (n=87) | 0.172 |
| Copper (ng/mL) | 88.2±32.5 (n=75) | 94.9±26.7 (n=87) | 0.147 |
| Nutrition status | n=72 | n=86 | |
| Well nourished | 16 (22) | 17 (20) | 0.844 |
| Malnourished | 56 (78) | 69 (80) | 0.844 |
Values are presented as number (%), mean±standard deviation, or number only.
ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein.
aPneumonia, Fournier’s gangrene, Necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Table 1
Baseline characteristics of the study population
Values are presented as mean±standard deviation (range) or number (%). ICU = intensive care unit; AAA = abdominal aortic aneurysm. aPneumonia, Fournier’s gangrene, necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis. bASPEN (American Society for Parenteral and Enteral Nutrition).
Table 2
Prevalence of micronutrient deficiencies in SICU patients (N=210)
SICU = surgical intensive care unit; SD = standard deviation. aOnly measurements performed within 7 days of ICU admission were included in the analysis.
Table 3
Comparison of clinical outcomes and baseline characteristics between copper-deficient and normal groups
Values are presented as number (%), mean±standard deviation, or number only. ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein. aPneumonia, Fournier’s gangrene, necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Table 4
Comparison of clinical outcomes and baseline characteristics between zinc-deficient and normal groups
Values are presented as number (%), mean±standard deviation, or number only. ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein. aPneumonia, Fournier’s gangrene, Necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.
Table 5
Comparison of clinical outcomes and baseline characteristics between severe (<10 ng/mL) and non-severe (≥10 ng/mL) vitamin D deficiency groups
Values are presented as number (%), mean±standard deviation, or number only. ICU = intensive care unit; AAA = abdominal aortic aneurysm; CRP = C-reactive protein. aPneumonia, Fournier’s gangrene, Necrotizing pancreatitis, subglottic stenosis, bladder perforation, urosepsis, CPCR (cardio-pulmonary cerebral resuscitation) survivor, gallbladder perforation, cytomegalovirus esophagitis, deep neck infection, graft failure, biliary sepsis.

