 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > J Clin Nutr > Volume 9(2); 2017 > Article
- Original Article Determination of the Stress Factor Calculated from the Changes in the Measured Resting Energy Expenditure with Indirect Calorimetry in Patients Undergoing Pancreaticoduodenectomy
- Seon Hyeong Kim1,2, Baik Hwan Cho1,3, Sook Bae Kim2, Mi Jin Jeong1, Hee Chul Yu1,3
- 췌십이지장절제술 환자의 간접열량측정기로 측정한 휴식대사량 변화를 이용한 스트레스 계수의 산정
- 김선형1,2, 조백환1,3, 김숙배2, 정미진1, 유희철1,3
-
Journal of the Korean Society for Parenteral and Enteral Nutrition 2017;9(2):62-67.
DOI: https://doi.org/10.15747/jcn.2017.9.2.62
Published online: December 31, 2017
Nutrition Support Team, Chonbuk National University Hospital, Jeonju, Korea
Department of Food Science and Human Nutrition, Chonbuk National University, Jeonju, Korea
Department of Surgery, Chonbuk National University Medical School, Jeonju, Korea
- Correspondence to Hee Chul Yu Department of Surgery, Chonbuk National University Medical School, 20 Geonji-ro, Deokjin-gu, Jeonju 54907, Korea Tel: +82-63-250-1604, Fax: +82-63-250-1604, E-mail: hcyu@jbnu.ac.kr
• Received: June 13, 2017 • Revised: August 23, 2017 • Accepted: September 27, 2017
Copyright: © Korean Society for Parenteral and Enteral Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 10,488 Views
- 124 Download
Abstract
-
Purpose To predict the energy expenditure using the stress factor representing the ratio of the metabolic variation between pre-operation and post-operation in a pancreaticoduodenectomy (PD).
-
Methods This was a prospective study conducted on 17 patients (11 males and 6 females) who underwent PD at Chonbuk National University Hospital between March 2010 and October 2011. The rest energy expenditure was measured by indirect calorimetry 1 day before and 3 days after surgery. The height, weight, and fat free mass were also measured 1 day before surgery.
-
Results The mean measured rest energy expenditure 1 day before PD (mREEpre) and 3 days after PD (mREEpost) were significantly different (16.8±2.6 vs. 18.8±3.5 kcal/kg/d, P=0.0076). The stress factor, representing the ratio of the metabolic changes between pre- and post-PD, was 1.12±0.17. The recommended energy requirement for PD patients is estimated to be 23∼24 kcal/ideal body weight/d [determined from the measured preoperative rest energy expenditure (16.8±2.6 kcal/kg/d)×activity factor (1.2∼1.3)×stress factor (1.12)].
-
Conclusion PD patients maintained a hypermetabolic status and the applicable stress factor was 1.12.
INTRODUCTION
The nutritional status of surgical patients affects postoperative complications, morbidity, length of hospital stay, and prognosis. Energy deficiency delays healing of the surgical site and wounds, causes weakened immune function, and extends the duration of dependence on mechanical ventilators. Conversely, energy overload can cause complications such as hyperglycemia, hyperlipidemia, imbalance of electrolytes, and pulmonary dysfunction. Proper nutritional intervention based on an accurate calculation of energy requirements is an important component of treatment in surgical patients.1,2
Pancreaticoduodenectomy (PD) is a surgical procedure that involves resection and reconstruction of a functional organ directly related to nutrient absorption and digestion. Recent studies show that nutritional interventions shorten the length of bowel resting time, hospital stay, and the recovery period after hospital discharge.3,4 To increase the effectiveness of treatment in PD patients, appropriate nutrition management of energy is required.
The gold standard to determine energy expenditure is indirect calorimetry (IC), but this method is expensive, labor-intensive, limitations of time and space, and difficulty handling procedure.5 In clinics, simple, cost-effective and easy-to-use formulas are commonly applied instead of IC. Energy expenditure can be calculated by multiplying activity and stress factors with the basal metabolic rate obtained from the Harris-Benedict equation.6 The metabolic stress factor is affected by illness, fever, trauma, and surgery. Evaluating energy requirements with the optimal stress coefficient can prevent complications resulting from energy imbalance during the postoperative recovery period.
The purpose of this study was to evaluate stress factor representing the ratio of preoperative and postoperative metabolic variation measured with IC, and to predict energy expenditure by using of the stress factor in PD patients.
MATERIALS AND METHODS
This study included 17 patients (11 males, 6 females) who had undergone PD and consented to participate between March 2010 and October 2011 at Chonbuk National University Hospital. We excluded patients under the age of 18, with cystic fibrosis, fever, or paralysis (quadriplegia or paraplegia), and prescribed catecholamines, sedatives, or muscle relaxants because of their effect on basal metabolic rate. The current study was approved by the Chonbuk National University Hospital Institutional Review Board (CBIRB1006-74).
The rest energy expenditure (REE) was measured by IC (Vmax 29n; Sensor Medics Co., Yorba Linda, CA, USA) on preoperative day 1 and postoperative day 3. On preoperative day 1, the patient’s height, weight, and fat free mass were measured using the Bio Impedance Analyzer (Inbody720; Biospace Co., Seoul, Korea). Ideal body weight (IBW) was obtained by squared meter height multiply with 22 in male (22×m2), 21 in female (21×m2). Body mass index (BMI) was calculated as weight divided by the square of the height (kg/m2).
General characteristics such as gender, age, disease diagnosis, operation name, and drug use were collected from review of the medical records. Nutritional status was evaluated with a patient-generated subjective global assessment method on preoperative day 1.
The gas analyzer was calibrated according to the manufacturer’s standard protocol before each measurement on preoperative day 1 (mREEpre, resting energy expenditure measured by IC on preoperative day 1) and postoperative day 3 (mREEpost, resting energy expenditure measured by IC on postoperative day 3).
Fasting was maintained for 5 hours, and injected drugs and nutrients were continuously infused for at least 12 hours prior to each measurement. A rest period of 30 minutes was allowed before the measurement, and then resting energy expenditure was measured for 30 minutes with the patient in a supine position wearing a facemask at a steady state (constantly maintained state of respiratory quotient change ratio <5%, oxygen consumption and carbon dioxide production change ratio <10% for 5 minutes). One technician conducted the measurements and was dedicated to an exclusive thermoneutral ward room in the morning.7 Resting energy expenditure was calculated from the Weir equation [(3.94VO2+1.11VCO2)×1.44], and respiratory quotients were determined from inspired oxygen and expired carbon dioxide (Fig. 1).8

Statistical analysis was performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) and SAS ver. 9.2 (SAS Inc., Cary, NC, USA). Continuous variables of the study subjects were analyzed using Student’s t-test, paired t-test, and regression analysis. A P-value <0.05 was considered statistically significant.
RESULTS
In the 17 patients, the mean age was 62.2±12.8 years, actual body weight was 60.1±8.7 kg, height was 160.5±7.5 cm, IBW was 56.5±5.6 kg, and fat free mass was 44.2±8.7 kg. Mean BMI was 23.2±2.5 kg/m2 and was classified according to the criteria of the World Health Organization Asia-Pacific; 1 patient (5.9%) was underweight with a BMI <18.5 kg/m2, 5 patients (29.4%) had an adequate BMI of 18.5∼22.9 kg/m2, 6 patients (35.3%) were overweight with a BMI of 23∼24.9 kg/m2, and 5 patients (29.4%) were obese with a BMI ≥25 kg/m2. The primary diagnoses were pancreatic head carcinoma in 5 patients, ampulla of Vater carcinoma in 5 patients, and distal common bile duct carcinoma in 7 patients. Out of the 17 total patients, 11 subjects (64.7%) underwent pylorus preserving PD, 6 subjects (35.3%) done with Whipple’s operation. Our result from the nutritional assessment showed that 14 patients (82.4%) were well nourished, 3 patients (17.6%) had moderate malnutrition, and none had severe malnutrition. General demographic and anthropometric data are shown in Table 1.
Table 1
Demographic and anthropometric data (n=17)
| Measurements | Data |
|---|---|
| Sex (male/female) | 11/6 |
| Age (y) | 62.2±12.8 |
| Weight (kg) | 60.1±8.7 |
| Height (cm) | 160.5±7.5 |
| Ideal body weight (kg)a | 56.5±5.6 |
| Fat free mass (kg) | 44.2±8.7 |
| BMI (kg/m2) | 23.2±2.5 |
| Underweightb | 1 (5.9) |
| Adequate | 5 (29.4) |
| Overweight | 6 (35.3) |
| Obese | 5 (29.4) |
| Diagnosis | |
| Pancreatic head carcinoma | 5 (29.4) |
| Ampulla of Vater carcinoma | 5 (29.4) |
| Distal common bile duct carcinoma | 7 (41.2) |
| Operation procedure | |
| Pylorus preserving pancreaticoduodenectomy | 11 (64.7) |
| Whipple’s procedure | 6 (35.3) |
| Nutritional status | |
| Well-nourished | 14 (82.4) |
| Moderate malnutrition | 3 (17.6) |
| Severe malnutrition | 0 (0) |
Values are presented as number only, mean±standard deviation, or number (%).
aIdeal body weight was calculated by squared meter height multiply with 22 in male (22×m2), 21 in female (21×m2).
bClassified according to the criteria of the World Health Organization Asia-Pacific, body mass index (BMI)<18.5 kg/m2 is underweight, BMI 18.5∼22.9 kg/m2 is adequate, BMI 23.0∼24.9 kg/m2 is overweight, BMI>25.0 kg/m2 is obese.
On the day before surgery, 12 patients received only parenteral nutrition, 5 patients were fasted (without receiving parenteral nutrition) and energy intakes of 12 patients who received parenteral nutrition was 14.5±4.7 kcal/kg/d. On postoperative day 3, 14 patients were on a regimen of combined oral intake with parenteral nutrition and the mean energy intakes was 17.4±5.3 kcal/kg/d. Three subjects had not received any nutrition by either oral intake or parenteral nutrition (Table 2).
Table 2
Nutrition route and energy intake (n=17)
| Nutrition route | Preoperative day 1 | Postoperative day 3 |
|---|---|---|
| Only parenteral | 12 | 0 |
| Parenteral+oral | 0 | 14 |
| NPO | 5 | 3 |
| Energy intake (kcal/kg/d)a | 14.5±4.7 | 17.4±5.3 |
Based on regression analysis of mREE and fat free mass, the correlation rate for mREEpost was R2=0.484 (P=0.003) and for mREEpre was 0.457 (P=0.002), significant values means that there is a positive correlation between fat free mass and mREE (Fig. 2).
Fig. 2
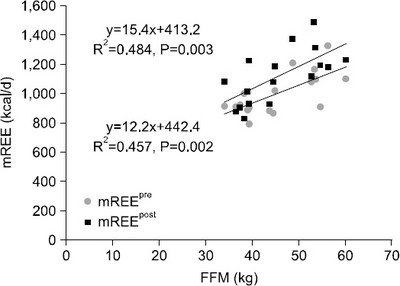
Changes in measured resting energy expenditure (mREE) after pancreaticoduodenectomy. FFM = fat free mass, mREEpre = resting energy expenditure measured with indirect calorimetry on preoperative day 1, mREEpost = resting energy expenditure measured with indirect calorimetry on postoperative day 3.
Three of the subjects (17.6%) had lower mREEpost than mREEpre, while 14 patients (82.4%) had higher mREEpost than mREEpre. The mean mREEpre was significant lower than mREEpost (1,000.24±143.08 vs. 1,113.82±184.93 kcal/d, P=0.0095). mREEpost per actual weight was statistically higher than mREEpre per actual weight (18.8±3.5 vs. 16.8± 2.6 kcal/kg/d, P=0.0076) (Fig. 3). The calculated stress factor expressed as the ratio of energy metabolic change pre- and post-PD was 1.12±0.17.
Fig. 3
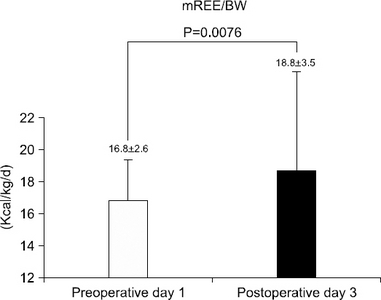
Change in measured resting energy expenditure (mREE) on preoperative day 1 and postoperative day 3 after pancreaticoduodenectomy. BW = body weight.
The mean preoperative measured respiratory quotient (mRQ) and the postoperative mRQ were not significantly different (0.76±0.11 vs. 0.74±0.11, P=0.549) (Fig. 4).
Fig. 4
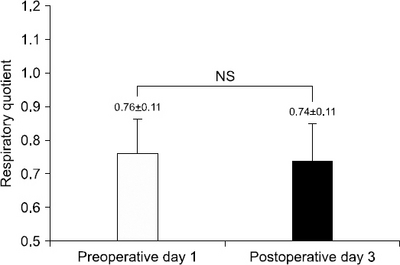
Change in measured respiratory quotient on preoperative day 1 and postoperative day 3 after pancreaticoduodenectomy. NS = non significant.
DISCUSSION
The prevalence of malnutrition in preoperative abdominal surgical patients has been reported to be as high as 40% and was greater than 80% before surgery in patients with gastrointestinal cancer.9-11 After surgery, maintenance of a hypermetabolic state due to the inflammatory response caused increase in the secretion of cytokines and stress hormones. In adults, trauma or surgery causes a brief, 2∼4 hours “ebb” period of a depressed metabolic rate followed by a 2∼7 days, “flow phase” characterized by an increase in oxygen consumption to support the massive exchanges of substrate between organs.12 There is hypermetabolic in energy expenditure in the first 5 to 7 days after an operation.13 It has been reported that the incidence of malnutrition in surgical patients ranges from 9%∼44%.14 In this study, 17.6% of the subjects were malnourished on preoperative day 1.
Pancreatic endocrine dysfunctions increase the risk of metabolic abnormalities and insulin resistance in PD. Caloric overfeeding can also lead to metabolic complications, and negative energy balance is an important limiting factor in wound healing and surgical recovery. Calculation of the appropriate energy expenditure in surgical patients is inevitable for nutrional management. Although the use of IC is recommended for more accurate calculation of energy expenditure, clinics commonly use equations that applied indicators are easier to collect.
When energy expenditure is determined using a formula, it is often calculated by multiplying the activity and stress factor with the basal metabolic expenditure obtained by the Harris-Benedict equation. Stress factor values can vary widely based on the patient’s condition. The American Society for Parenteral and Enteral Nutrition (ASPEN) recommends the following stress factor values for different conditions: 0.85 in simple starvation, 1.05 to 1.15 in surgery, 1.20 to 1.4 in sepsis, 1.3 in head injury, 1.4 in multiple trauma, 1.5 in systemic inflammation, and 2.0 in severe burns.15
Based on the results of previous studies on the rate of variation in the metabolism of surgical patients, Calvin recommended a stress coefficient of 1.2 for planned surgical patients without complications,16 while Rutten recommended a coefficient of 1.75 to 2.0.17 Farhi recommended a stress factor around 1.1∼1.2 after extensive surgery,18 and Sasaki recommended a stress factor increase of 12% after PD.19 Most research has shown that the increase in postoperative from preoperative mREE was about 10%.16-20 In this study, the stress factor represented by the mREEpost/mREEpre ratio was 1.12, and the energy expenditure increased 12% after PD.
In view of present study, we recommended energy requirement for PD patients is 23∼24 kcal/IBWkg daily, by an activity factor of 1.2 to 1.3 according to the ASPEN guidelines (mean mREEpre/body weight 16.8 kcal/kg×activity factor 1.2∼1.3×stress factor 1.12=23∼24 kcal/kg).21 The many of patients were overweight (35.3%) and obese (29.4%) so we were recommended as the IBW.
The Spanish Society of Intensive Care Medicine and Coronary Units-Spanish Society of Parenteral and Enteral Nutrition recommends 25∼30 kcal/kg/d for surgical patients in the intensive care unit, 20∼25 kcal/kg/d for hyperglycemic patients, and 20∼25 kcal/kg for patients in a catabolic state, with a gradual increase to 25∼30 kcal/kg/d but not exceeding 2,000 kcal daily for patients in an anabolic state.22
The European Society of Parenteral And Enteral Nutrition recommends approximately 25 kcal/kg (IBW) in surgical patients and 30 kcal/kg/d in severe stress states.23 Walker and Heuberger24 didn’t recommend against calculating energy expenditure with merely the patient’s weight. It is desirable to use IC to determine energy requirements in PD, but it should be consider of the stress factor in case of IC is not available.
This study’s first limitation is small sample size, with only 17. In several studies examining postoperative metabolic changes, the amount of time to reach metabolic stabilized states differed depending on surgery type, extension, and basic disease.25 Digestive tract surgery patients without complications achieved hemodynamic stable states and fluid balance within 1∼3 days after surgery.26 In this study, REE was measured on postoperative day 3; however, these measurements were obtained in a small number of subjects. Several patients who agreed to participate before PD dropped out of the study because they did not achieve medical stabilization on postoperative day 3. The second limitation of this research is the short length of the study period, we were unable to examine the time patients to achive a postoperative metabolically stable state. In the future, a prospective trial comparing mREEpre with mREEpost in PD is needed that a large number of participants with a longer study period. Despite the above limitations, this prospective study is a comparative analysis of pre- and post-energy expenditure with IC and obtained referral data that can be used to determine the appropriate energy expenditure for PD patients.
CONCLUSION
The current study showed that undergoing PD patient maintained hypermetabolic state and the stress factor measured by IC was 1.12. We recommended careful monitoring of indicators affect the stress factor when determine energy expenditure with a stress factor.
- 1. Kemper M, Weissman C, Hyman AI. Caloric requirements and supply in critically ill surgical patients. Crit Care Med 1992;20(3):344-8. ArticlePubMed
- 2. Auxiliadora Martins M, Menegueti MG, Nicolini EA, Picolo MF, Lago AF, Martins Filho OA, et al. Energy expenditure in critically ill surgical patients. Comparative analysis of predictive equation and indirect calorimetry. Acta Cir Bras 2011;26(Suppl2):51-6. Article
- 3. Pappas S, Krzywda E, McDowell N. Nutrition and pancreaticoduodenectomy. Nutr Clin Pract 2010;25(3):234-43. ArticlePubMedPDF
- 4. Lassen K, Kjaeve J, Fetveit T, Tranø G, Sigurdsson HK, Horn A, et al. Allowing normal food at will after major upper gastrointestinal surgery does not increase morbidity: a randomized multicenter trial. Ann Surg 2008;247(5):721-9. PubMed
- 5. Wooley JA. Indirect calorimetry: applications in practice. Respir Care Clin N Am 2006;12(4):619-33. PubMed
- 6. Reilly JJ Jr, Gerhardt AL. Modern surgical nutrition. Curr Probl Surg 1985;22(10):1-81. Article
- 7. Haugen HA, Chan LN, Li F. Indirect calorimetry: a practical guide for clinicians. Nutr Clin Pract 2007;22(4):377-88. ArticlePubMedPDF
- 8. Weir JB. New methods for calculating metabolic rate with special reference to protein metabolism. J Physiol 1949;109(1-2):1-9. ArticlePubMedPMC
- 9. Schiesser M, Müller S, Kirchhoff P, Breitenstein S, Schäfer M, Clavien PA. Assessment of a novel screening score for nutritional risk in predicting complications in gastro-intestinal surgery. Clin Nutr 2008;27(4):565-70. ArticlePubMed
- 10. Cerantola Y, Grass F, Cristaudi A, Demartines N, Schäfer M, Hübner M. Perioperative nutrition in abdominal surgery: recommendations and reality. Gastroenterol Res Pract 2011;doi:10.1155/2011/739347. ArticlePDF
- 11. Prieto Reyes MA, Márquez Báez MA, Vázquez Márquez L, Redel del Pueyo J, Gordón del Río A, Arévalo Jiménez E. Nutritional status of patients undergoing digestive surgery. Nutr Hosp 1993;8(2):94-6. PubMed
- 12. Hill AG, Hill GL. Metabolic response to severe injury. Br J Surg 1998;85(7):884-90. ArticlePubMedPDF
- 13. Jones MO, Pierro A, Hammond P, Lloyd DA. The metabolic response to operative stress in infants. J Pediatr Surg 1993;28(10):1258-62. ArticlePubMed
- 14. Reid CL. Nutritional requirements of surgical and critically-ill patients: do we really know what they need? Proc Nutr Soc 2004;63(3):467-72. ArticlePubMed
- 15. Sax HC, Souba WW. Nutritional goals and macronutrient requirement. The A.S.P.E.N nutrition support practice manual. 2nd ed. Silver Spring, MD: ASPEN; 1998. p. 2-3.
- 16. Long CL, Schaffel N, Geiger JW, Schiller WR, Blakemore WS. Metabolic response to injury and illness: estimation of energy and protein needs from indirect calorimetry and nitrogen balance. JPEN J Parenter Enteral Nutr 1979;3(6):452-6. ArticlePubMed
- 17. Rutten P, Blackburn GL, Flatt JP, Hallowell E, Cochran D. Determination of optimal hyperalimentation infusion rate. J Surg Res 1975;18(5):477-83. ArticlePubMed
- 18. Farhi LE, Rahn H. Gas stores of the body and the unsteady state. J Appl Physiol 1955;7(5):472-84. ArticlePubMed
- 19. Sasaki M, Okamoto H, Johtatsu T, Kurihara M, Iwakawa H, Tanaka T, et al. Resting energy expenditure in patients undergoing pylorus preserving pancreatoduodenectomies for bile duct cancer or pancreatic tumors. J Clin Biochem Nutr 2011;48(3):183-6. ArticlePubMedPMC
- 20. Frankentfield D. Energy dynamics. In: Matarese LE, Gottschlich MM, editors. Contemporary nutrition support practice: a clinical guide. Philadelphia: WB Saunders Co; 1998. p. 88-9.
- 21. Merritt R, DeLegge MH, Holcombe B, Mueller C, Ochoa J, Smith KR, et al. Fundamentals of nutrition support practice and management. The A.S.P.E.N nutrition support practice manual 2nd ed. Silver Spring, MD: ASPEN; 1998;45.
- 22. Sánchez Álvarez C, Zabarte Martínez de Aguirre M, BordejéLaguna L; Metabolism and Nutrition Working Group of the Spanish Society of Intensive Care Medicine and Coronary units. Guidelines for specialized nutritional and metabolic support in the critically-ill patient: update. Consensus SEMICYUC-SENPE: gastrointestinal surgery. Nutr Hosp 2011;26(Suppl2):41-5. PubMed
- 23. Braga M, Ljungqvist O, Soeters P, Fearon K, Weimann A, Bozzetti F. ESPEN ESPEN Guidelines on Parenteral Nutrition: surgery. Clin Nutr 2009;28(4):378-86. PubMed
- 24. Walker RN, Heuberger RA. Predictive equations for energy needs for the critically ill. Respir Care 2009;54(4):509-21. ArticlePubMedPDF
- 25. Ishikawa M, Nishioka M, Hanaki N, Kikutsuji T, Miyauchi T, Kashiwagi Y, et al. Postoperative metabolic and circulatory responses in patients that express SIRS after major digestive surgery. Hepatogastroenterology 2006;53(68):228-33. PubMed
- 26. Nishioka M, Ishikawa M, Hanaki N, Kashiwagi Y, Miki H, Miyake H, et al. Perioperative hemodynamic study of patients undergoing abdominal surgery using pulse dye densitometry. Hepatogastroenterology 2006;53(72):874-8. PubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteDetermination of the Stress Factor Calculated from the Changes in the Measured Resting Energy Expenditure with Indirect Calorimetry in Patients Undergoing Pancreaticoduodenectomy

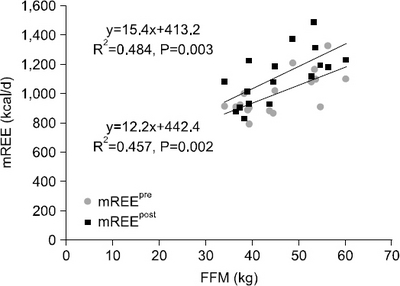
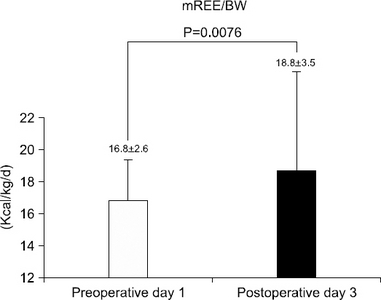
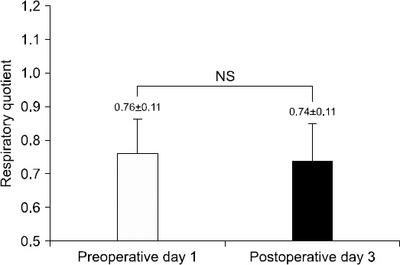
Fig. 1
Pictures of a patient and equipment used during indirect calorimetry measurement.
Fig. 2
Changes in measured resting energy expenditure (mREE) after pancreaticoduodenectomy. FFM = fat free mass, mREEpre = resting energy expenditure measured with indirect calorimetry on preoperative day 1, mREEpost = resting energy expenditure measured with indirect calorimetry on postoperative day 3.
Fig. 3
Change in measured resting energy expenditure (mREE) on preoperative day 1 and postoperative day 3 after pancreaticoduodenectomy. BW = body weight.
Fig. 4
Change in measured respiratory quotient on preoperative day 1 and postoperative day 3 after pancreaticoduodenectomy. NS = non significant.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Determination of the Stress Factor Calculated from the Changes in the Measured Resting Energy Expenditure with Indirect Calorimetry in Patients Undergoing Pancreaticoduodenectomy
Demographic and anthropometric data (n=17)
| Measurements | Data |
|---|---|
| Sex (male/female) | 11/6 |
| Age (y) | 62.2±12.8 |
| Weight (kg) | 60.1±8.7 |
| Height (cm) | 160.5±7.5 |
| Ideal body weight (kg) |
56.5±5.6 |
| Fat free mass (kg) | 44.2±8.7 |
| BMI (kg/m2) | 23.2±2.5 |
| Underweight |
1 (5.9) |
| Adequate | 5 (29.4) |
| Overweight | 6 (35.3) |
| Obese | 5 (29.4) |
| Diagnosis | |
| Pancreatic head carcinoma | 5 (29.4) |
| Ampulla of Vater carcinoma | 5 (29.4) |
| Distal common bile duct carcinoma | 7 (41.2) |
| Operation procedure | |
| Pylorus preserving pancreaticoduodenectomy | 11 (64.7) |
| Whipple’s procedure | 6 (35.3) |
| Nutritional status | |
| Well-nourished | 14 (82.4) |
| Moderate malnutrition | 3 (17.6) |
| Severe malnutrition | 0 (0) |
Values are presented as number only, mean±standard deviation, or number (%).
aIdeal body weight was calculated by squared meter height multiply with 22 in male (22×m2), 21 in female (21×m2).
bClassified according to the criteria of the World Health Organization Asia-Pacific, body mass index (BMI)<18.5 kg/m2 is underweight, BMI 18.5∼22.9 kg/m2 is adequate, BMI 23.0∼24.9 kg/m2 is overweight, BMI>25.0 kg/m2 is obese.
Nutrition route and energy intake (n=17)
| Nutrition route | Preoperative day 1 | Postoperative day 3 |
|---|---|---|
| Only parenteral | 12 | 0 |
| Parenteral+oral | 0 | 14 |
| NPO | 5 | 3 |
| Energy intake (kcal/kg/d) |
14.5±4.7 | 17.4±5.3 |
NPO = nil per os (nothing by mouth and no parenteral nutrition).
aMean energy intake of subjects with provided nutritional support.
Table 1 Demographic and anthropometric data (n=17)
Values are presented as number only, mean±standard deviation, or number (%). Ideal body weight was calculated by squared meter height multiply with 22 in male (22×m2), 21 in female (21×m2). Classified according to the criteria of the World Health Organization Asia-Pacific, body mass index (BMI)<18.5 kg/m2 is underweight, BMI 18.5∼22.9 kg/m2 is adequate, BMI 23.0∼24.9 kg/m2 is overweight, BMI>25.0 kg/m2 is obese.
Table 2 Nutrition route and energy intake (n=17)
NPO = nil per os (nothing by mouth and no parenteral nutrition). Mean energy intake of subjects with provided nutritional support.

