 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > J Clin Nutr > Volume 12(2); 2020 > Article
- Original Article Effect of Nutritional Intervention by the Nutrition Support Team on Postnatal Growth in Preterm Infants
-
So Jin Yoon1,2
 , Joo Hee Lim1,2, Soon Min Lee1,2, Sun Jung Kim3, Sun Kyung Lee4, Soo Min Lee4
, Joo Hee Lim1,2, Soon Min Lee1,2, Sun Jung Kim3, Sun Kyung Lee4, Soo Min Lee4 - 미숙아에서 영양지원팀에 의한 영양중재가 출생 후 성장에 미치는 영향
-
윤소진1,2, 임주희1,2, 이순민1,2, 김선정3, 이선경4, 이수민4
-
Journal of Clinical Nutrition 2020;12(2):26-33.
DOI: https://doi.org/10.15747/jcn.2020.12.2.26
Published online: December 31, 2020
1Department of Pediatrics, Yonsei University College of Medicine, Seoul, Korea
2Department of Pediatrics, Gangnam Severance Hospital, Seoul, Korea
3Department of Nutrition, Gangnam Severance Hospital, Seoul, Korea
4Department of Pharmacy, Gangnam Severance Hospital, Seoul, Korea
- Correspondence to Soon Min Lee https://orcid.org/0000-0003-0174-1065 Department of Pediatrics, Yonsei University College of Medicine, Gangnam Severance Hospital, 211 Eonjuro, Gangnamgu, Seoul 06273, Korea Tel: +82-2-2019-3350, Fax: +82-2-2019-4881, E-mail: smlee@yuhs.ac
• Received: October 21, 2020 • Revised: November 27, 2020 • Accepted: December 1, 2020
© 2020, The Korean Society for Parenteral and Enteral Nutrition. All Rights Reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,898 Views
- 3 Download
- 1 Crossref
Abstract
-
Purpose Nutritional intervention by an interdisciplinary nutrition support team (NST) can potentially improve postnatal growth outcomes in preterm infants. This study aimed to measure the growth impact of a nutritional intervention package performed by an NST in a quality improvement effort in a neonatal intensive care unit (NICU).
-
Methods Fifty-two infants born below 2,000 g and admitted to NICU participated in the Quality Improvement (QI) program between March 2016 and February 2017. The nutritional intervention was applied according to newly established nutritional guidelines on parenteral and enteral nutrition, and an NST performed a weekly nutritional assessment. The Z-scores of weight, height, and head circumference were calculated according to the gestational age and sex. The clinical impact on postnatal growth was compared between the QI and pre-QI groups. The pre-QI group included 69 infants admitted in the same NICU between 2014 and 2015.
-
Results The time to the initiation of enteral nutrition decreased significantly (P<0.001). Changes in weight (P=0.027), head circumference (P=0.003), Z-scores between birth, and 40 weeks postconceptional age (PCA) were significantly larger in the QI than the pre-QI group. The percentage of infants weighing below the 10th percentile at one month after birth and at 40 weeks PCA was higher in the pre-QI than the QI group.
-
Conclusion The implementation of evidence-based best practices for preterm nutrition resulted in significant improvements in the growth outcomes in preterm infants.
INTRODUCTION
The nutritional goal with preterm infants is to support them to grow at a rate similar to intrauterine fetuses. However, preterm infants experience severe growth restriction during the postnatal intensive care period. Despite aggressive treatment, chronic nutritional deprivation and growth failure in preterm infants continues to be a problem.1 The more immature the infant, the greater the degree of postnatal growth failure.2,3 Furthermore, the growth velocity of extremely low birth weight infants during neonatal intensive care unit (NICU) hospitalization exerts a significant effect on the neurodevelopmental and growth outcomes at 18 to 22 months corrected age.4
Active nutritional intervention improves growth and morbidity. Applying a comprehensive nutrition bundle to very low birth weight (VLBW) infants improved growth of length and head circumference, reduced severe growth restriction, and decreased the incidence of necrotizing enterocolitis (NEC) and sepsis.5 The modification of nutritional strategy in a study from South Korea showed an improvement in average growth rates for weight and height from the commencement of full enteral feeding to 40 weeks postconceptional age (PCA). Furthermore, it showed a trend for the incidence of weight, height, and head circumference below the 10th percentile to decrease at 40 weeks.6 In another study, a high enteral feeding volume regimen was associated with low rates of in-hospital growth restriction and good head growth, which improved language development.7
National support for NICU nutritional support team (NST) configuration began in South Korea in April 2015 for promoting recovery and proper growth by providing appropriate nutritional support. However, the quality of NST practices has been variable, and the discussion of NST rounds, patient case analysis, nutritional assessment, and nutritional prescriptions has been limited.
This study aimed to measure the growth impact of a nutritional intervention package implemented by a multidisciplinary NST as a quality improvement effort for preterm infants. Proving the effectiveness of NSTs would be helpful for expanding the activity nationally.
MATERIALS AND METHODS
A multidisciplinary NST comprising a neonatologist, a pharmacist, a dietitian, and nurse has conducted Quality Improvement (QI) project in Gangnam Severance Hospital for a year since March, 2016. The QI project was included to review the evidence-based practices and to evaluate factors contributing to preterm nutrition to address the most important causes of postnatal growth failure in our center. Fishbone diagram depicting causes of poor growth was implemented (Fig. 1). Finally we implemented a nutritional intervention package to aim reducing the incidence of weight below the 10th percentile to less than 50% at 1 month after birth and to less than 30% at 40 weeks PCA. All preterm infants below 35 weeks of gestational age and 2,000 g admitted to Gangnam Severance Hospital NICU and participated in the QI project were included. The infants with prospective data collected between March 2016 and February 2017 were classified as the QI group. Preterm infants admitted between January 2015 and December 2015 were classified as pre-QI group to compare the effects of QI on the growth.
Nutritional intervention package was as follows; An enteral nutrition (EN) regimen included minimal enteral feeding from the first day, feeding initiation and advancement according to birth weight, and achievement of full enteral feeding (>100 mL/kg/day) within 2 weeks of birth. Protein was supplied from the first day using commercial parenteral nutrition (PN) when preparation PN was not available. In case of poor weight gain, energy supply less than caloric requirements, or a decrease in weight percentile compared to that at birth, a dietitian recommended additional caloric supplements according to the nutritional intervention package. The 16% concentration of premature infant formula was applied. In addition, adjusting the dose of vitamins and trace elements according to body weight, and controlling the supply of trace element by monitoring levels in long-term PN supply and ileostomy.
In order to evaluate the effect of nutritional intervention on the growth of premature infants, we measured weight daily, and height and head circumference weekly, during the admission period. Z-scores of body weight, height, and head circumference were calculated at birth, one month after birth and 40 weeks PCA adjusted for gestational age with reference to the Fenton 2013 preterm growth chart.8 The change of Z-score between birth and one month after birth, and between birth and 40 weeks PCA were calculated.
Nutritional and clinical data were collected via reviews of the patients’ electronic medical records. Small for gestational age (SGA) was defined as below 10 percentiles of birth weight for adjusting for gestational age and postnatal growth restriction was defined as having a growth value <10th percentile for PCA at the time of discharge.4 The nutritional data included the daily intake of energy, protein, lipids, and glucose during the first 7 days of life, the number of days to the initiation of enteral feeding, the number of days to reach full enteral feeding, and the number of days on PN. The amount of energy intake was calculated by adding both non-protein and protein calories. The parenteral intake and the enteral intake were added to determine the total intake per day.
The following definitions were applied in identifying comorbid conditions: patent ductus arteriosus (PDA), if surgery or medication was needed; hyaline membrane disease, if exogenous surfactant was administered; bronchopulmonary dysplasia (moderate or severe), if oxygen was used at 36 weeks PCA9; severe intraventricular hemorrhage (IVH), if grade 3 or 4 IVH identified from cranial imaging performed before 28 days of life10; periventricular leukomalacia (PVL), if evidence of PVL on cranial imaging found at any time; NEC, if clinical and radiographic findings indicated ≥stage 2 NEC11; severe retinopathy of prematurity (ROP), if disease stage ≥3 identified, treatment with retinal ablation surgery performed, or anti-vascular endothelial growth factor drug administered; cholestasis, if direct bilirubin >2 mg/dL; sepsis, if cultures positive for bacteria or fungi identified, and antibiotic therapy administered for ≥5 days.12,13
Independent t-tests were used to analyze continuous variables and chi-square tests were used for categorical variables. A P-value<0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS Statistics version 22 (IBM Co., Armonk, NY, USA). The study was registered with and approved by the hospital QI committee and ethics committee (Gangnam Severance Hospital Institutional Review Board number: 3-2019-0210).
RESULTS
Total 52 infants were included in QI group, and 69 infants were in the pre-QI group. There was no difference in gestational age at birth (30.8±2.7 vs. 31.1±3.0 weeks, P=0.624) or birth weight (1,457±382 vs. 1,528±340 g, P=0.293) between the pre-QI and QI groups (Table 1). The percentage of SGA infants was higher in the QI group than in the pre-QI group (19.2 vs. 5.8%, P=0.041).
As a result of applying the nutritional intervention package, significantly more protein and lipids were supplied on the first and second days of life, and significantly more cumulative energy, protein, and lipids were supplied during the first week, in the QI group than in the pre-QI group (Table 2 and Fig. 2).
Table 3 showed the growth outcomes between QI and pre-QI group. The difference in weight Z-score between 40 weeks PCA and at birth was significantly larger in the QI group than in the pre-QI group (P=0.027). There was a significantly higher percentage of SGA infants at birth in the QI group than in the pre-QI group, but the difference was reversed at one month after birth and at 40 weeks PCA. The increase in percentage of postnatal growth restricted (weight <10th percentile) infants was higher in the pre-QI group than in the QI group at the first month of life and at 40 weeks PCA. The difference in head circumference Z-score between 40 weeks PCA and at birth was significantly larger in the QI group than in the pre-QI group (P=0.003), so it is indicating a meaningful consequence of the between-group difference in the increasing percentage of SGA infants.
The incidence of treated PDA (14.5 vs. 36.2%, P=0.007), IVH (3.6 vs. 15.9%, P=0.037), and PVL (0 vs. 11.6%, P=0.009) was significantly lower in the QI group than in the pre-QI group. Further, cholestasis was not higher in the QI then in the pre-QI group (12.7 vs. 4.3%, P=0.107) despite more aggressive parenteral nutritional support (Table 1).
DISCUSSION
Inadequate nutritional intake aggravates the occurrence of postnatal growth restriction in VLBW infants. It is important to provide stable and adequate nutrients not only in the first weeks of life, but throughout the hospital stay.14 This study confirmed that QI for NST implementation improves growth outcomes of preterm babies in South Korea.
We confirmed that NST implementation improves weight gain between birth and 40 weeks PCA and suppresses an increased incidence of postnatal growth restricted premature infants at one month after birth. The initial goal of this QI exercise was to decrease the incidence of weights below the 10th percentile to less than 50% at one month after birth, and to less than 30% at 40 weeks PCA, in preterm infants weighing below 2,000 g. At one month after birth, the goal was achieved, but at 40 weeks PCA the percentage of preterm infants weighing below the 10th percentile was 32.7%. Compared to the pre-QI group, the incidence of premature infants weighing below the 10th percentile was significantly decreased, but the goal was nevertheless not achieved.
A significant relationship has been reported between the incidence of extrauterine growth retardation (EUGR) and NST availability, showing NSTs reduced the risk of EUGR by a magnitude of 0.47.15 Other studies have reported how a greater weight gain from birth to discharge was attained following NST implementation.16 In another South Korean study, NST intervention in an NICU resulted in improved clinical outcomes, such as increased weight gain and reduced length of hospital day.17 The advantage of the present study is the significant effect of NST intervention on weight Z-score changes, even though the incidence of IUGR was increasing.
Another report showed that the implementation of a nutrition bundle did not improve growth, but did decrease the incidence of NEC and sepsis/sepsis-like episodes.5 Also, practice changes, including the early supply of parenteral amino acids, resulted in decreasing EUGR at 36 weeks and a significant reduction in combined morbidity and mortality. In this study, we show a decreasing incidence of PDA, IVH, and PVL.
In this study, the incidence of cholestasis was not significantly different between groups, but showed an increasing trend. There was no difference in PN duration or time to reach full enteral feeding, so more monitoring is necessary to fully investigate the effect of aggressive PN on cholestasis.18 Some authors have reported a reduction in time to full enteral feeding and PN duration, without any difference in cholestasis incidence and with a significant reduction in the incidence of sepsis, possibly attributable to earlier discontinuation of a central line after the implementation of nutritional support.5,19
Infants born SGA or following IUGR are at risk of neurodevelopmental delay and developing cardiometabolic diseases in adulthood.20 A significant proportion of children born prematurely with severe EUGR show growth retardation in childhood, thus suggesting the need for close clinical follow-up to determine their growth potential and to implement effective intervention strategies.21 In this study, although long-term neurodevelopmental outcome was not analyzed, favorable outcomes, such as greater head circumference Z-score at one month after birth and at 40 weeks PCA in the QI group compared to the pre-QI group, were demonstrated, and also changes in head circumference showed significant improvement. This result is promising in terms of neurodevelopmental advantages in infancy and later childhood.
Premature infants are more vulnerable to inadequate nutrient supply and that leads to poor growth. Our nutritional intervention package included the evidence-based practice of enteral feedings being initiated on the first day of life, and trophic enteral feedings and PN being initiated earlier and advancing faster. There are many systemic and psychological barriers to providing EN and PN from the first day of life. However, through the QI effort, the achievement rate of trophic feeding from the first day of birth gradually increased and reached 100%. As for PN, to meet the caloric and lipid demand in the early stage,22,23 commercial PN products were used at the first day of life, overcoming the limitation of preparation PN.
Micronutrients have also been reported to affect the growth and development of newborns.24 With limitation of knowledge, multivitamins and micronutrients were recommended to adjust according to body weight.25 The zinc deficiency in long-term PN-provided patients and an impact on the excretion of copper and manganese in cholestasis patients were reported.26-28 Therefore, we reduced the supply of trace elements to PN-induced cholestasis patients by regularly monitoring serum Cu, Mn, and Zn levels.
The strength of this study is that it demonstrates how standardized nutritional protocol and practice have an effect on the growth of preterm babies, especially in terms of suppressing the increasing rate of postnatal growth restricted infants. While this study is of clinical interest, it has several limitations. First, we did not conduct a detailed investigation of which nutritional factors have a major impact on growth. The EN supply was analyzed without distinguishing between formula milk and breast milk. Furthermore, we did not conduct any evaluation of long-term neurodevelopmental outcomes.
CONCLUSION
In conclusion, the implementation of evidence-based best practice for preterm nutrition demonstrates the benefits of the early initiation of enteral feeding and faster and more rapidly advancing parenteral nutrition. These practice changes with active NST approach result in significant improvements in growth outcomes such as weight and head circumference in preterm infants.
ACKNOWLEDGMENTS
We would like to thank all nutritional support team members in Gangnam Severance Hospital.
This work was supported by the Clinical Research Program funded by the 2019 Korean Society for Parenteral and Enteral Nutrition. This study was supported by a research grant of Korean Society for Parenteral and Enteral Nutrition (2018).
Conflict of interest: None.
AUTHOR CONTRIBUTIONS
Investigation: Yoon SJ
Methodology: Yoon SJ, Lim JH, Lee Soon Min
Validation: Kim SJ, Lee Soo Min
Conceptualization: Lee Soon Min, Kim SJ, Lee Soo Min
Supervision: Lee Soon Min
Software: Yoon SJ, Lee Soon Min
Writing - original draft: Yoon SJ, Lee Soon Min
Writing - review & editing: Lee Soon Min
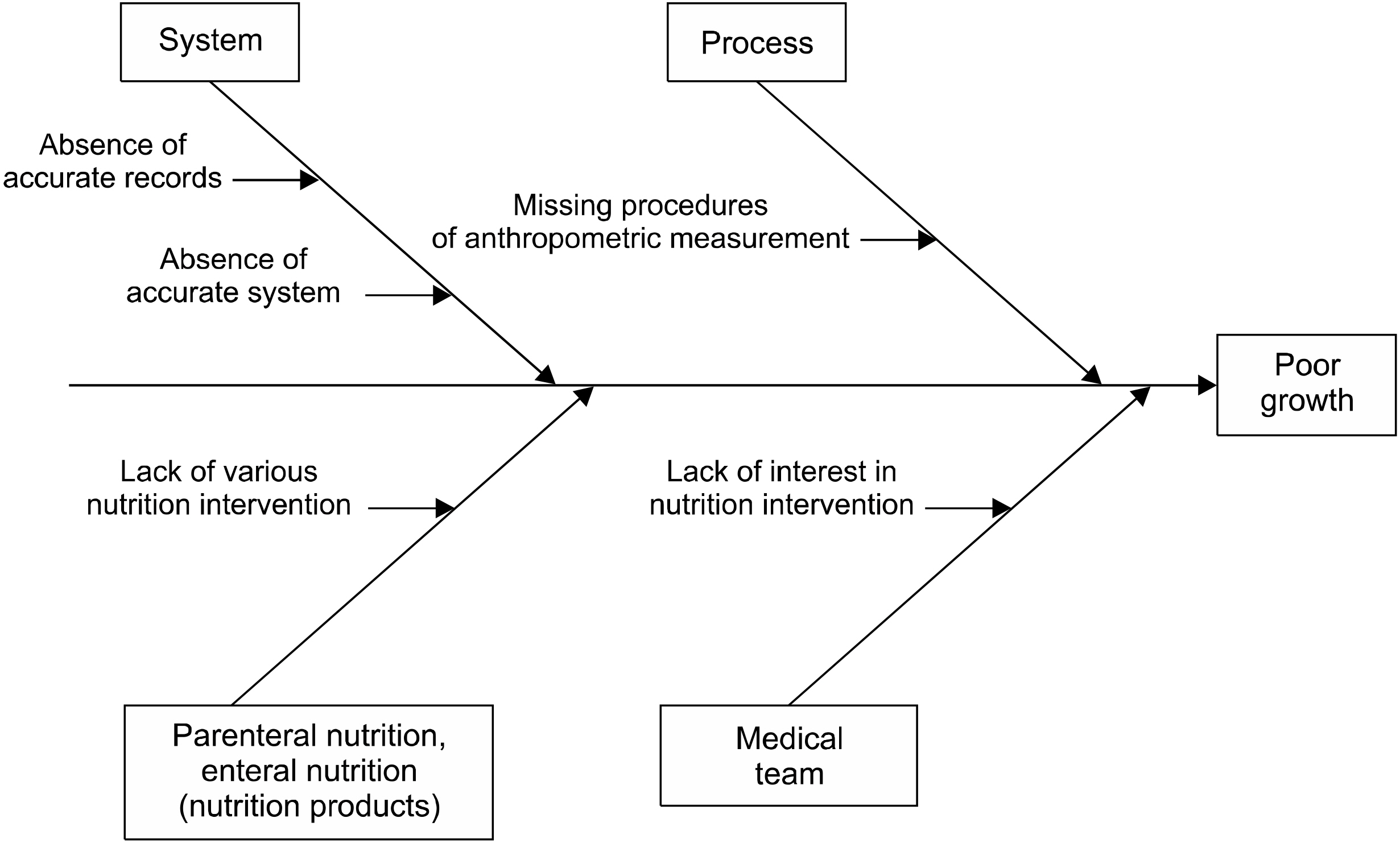
Fig. 2
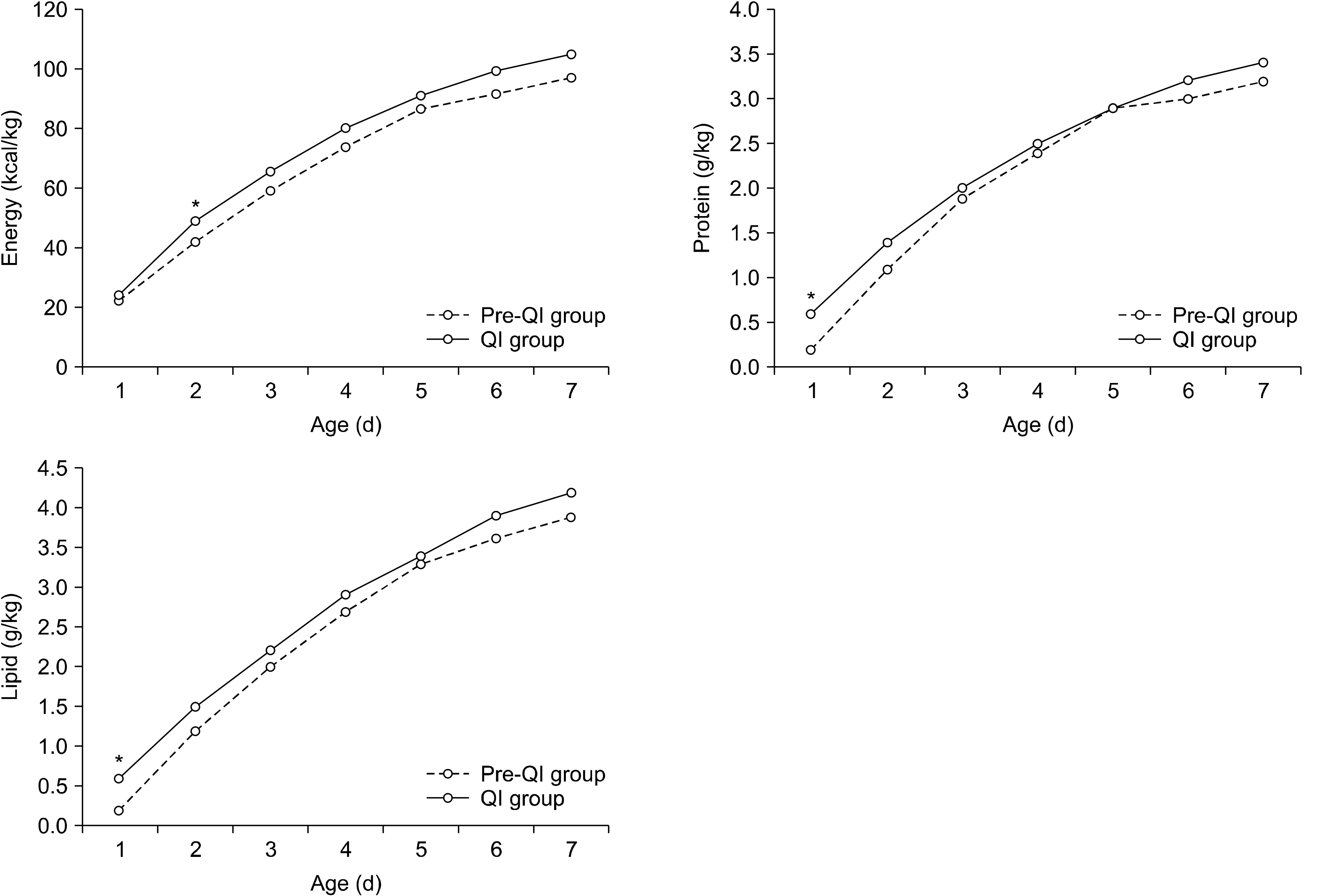
Comparisons of nutrition components during 1st week after birth between QI and pre-QI groups. QI = quality improvement.
Table 1
Patient characteristics and co-morbidities between pre-QI and QI group
| Variable | Pre-QI group (N=69) | QI group (N=52) | P-value |
|---|---|---|---|
| Gestational age (wk) | 30.8±2.7 | 31.1±3.0 | 0.624 |
| Birth weight (g) | 1,457±382 | 1,528±340 | 0.293 |
| Male, n (%) | 37 (53.6) | 26 (50.0) | 0.693 |
| Cesarean section | 50 (72.5) | 45 (86.5) | 0.062 |
| SGA | 4 (5.8) | 10 (19.2) | 0.041* |
| PROM | 16 (23.5) | 9 (17.3) | 0.406 |
| Chorioamnionitis | 6 (12.2) | 10 (19.2) | 0.599 |
| PIH | 4 (5.8) | 7 (13.5) | 0.203 |
| Maternal DM | 3 (4.3) | 7 (13.5) | 0.097 |
| Prenatal steroid | 19 (35.8) | 14 (26.9) | 0.513 |
| Apgar score 1 min | 4.6±1.8 | 5.0±1.3 | 0.127 |
| Apgar score 5 min | 6.7±1.4 | 6.8±1.2 | 0.686 |
| RDS | 54 (78.3) | 36 (69.2) | 0.260 |
| PDA | 25 (36.2) | 8 (14.5) | 0.007 |
| BPD | 23 (56.1) | 18 (43.9) | 0.943 |
| NEC | 0 | 0 | - |
| Cholestasis | 3 (4.3) | 7 (12.7) | 0.107 |
| Rickets | 7 (10.1) | 6 (10.9) | 0.890 |
| IVH | 11 (15.9) | 2 (3.6) | 0.037 |
| PVL | 8 (11.6) | 0 (0) | 0.009 |
| ROP | 13 (18.8) | 11 (20.0) | 0.871 |
| Sepsis | 5 (7.2) | 1 (1.8) | 0.226 |
| Hospital stay (d) | 52.0±47.4 | 51.5±42.6 | 0.950 |
Values are presented as mean±standard deviation or number (%).
- = not available; QI = quality improvement; SGA = small for gestational age; PROM = premature rupture of amniotic membrane; PIH = pregnancy-induced hypertension; DM = diabetes mellitus; RDS = respiratory distress syndrome; PDA = patent ductus arteriosus; BPD = bronchopulmonary dysplasia; IVH = intraventricular hemorrhage greater or equal to grade 3; PVL = periventricular leukomalacia; NEC = necrotizing enterocolitis; ROP = retinopathy of prematurity.
*P-value<0.05.
Table 2
Comparisons of nutrition components during 1st week after birth between QI and pre-QI groups
Table 3
Comparisons of nutrition and growth outcome between QI and pre-QI groups
- 1. Park JS, Han J, Shin JE, Lee SM, Eun HS, Park MS, et al. 2017;Postdischarge growth assessment in very low birth weight infants. Korean J Pediatr 60(3):64-9. ArticlePubMedPMCPDF
- 2. Embleton NE, Pang N, Cooke RJ. 2001;Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants? Pediatrics 107(2):270-3. ArticlePubMedPDF
- 3. Clark RH, Thomas P, Peabody J. 2003;Extrauterine growth restriction remains a serious problem in prematurely born neonates. Pediatrics 111(5 Pt 1):986-90. ArticlePubMedPDF
- 4. Ehrenkranz RA, Dusick AM, Vohr BR, Wright LL, Wrage LA, Poole WK. 2006;Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics 117(4):1253-61. ArticlePubMedPDF
- 5. Stefanescu BM, Gillam-Krakauer M, Stefanescu AR, Markham M, Kosinski JL. 2016;Very low birth weight infant care: adherence to a new nutrition protocol improves growth outcomes and reduces infectious risk. Early Hum Dev 94:25-30. ArticlePubMed
- 6. Choi AY, Lee YW, Chang MY. 2016;Modification of nutrition strategy for improvement of postnatal growth in very low birth weight infants. Korean J Pediatr 59(4):165-73. ArticlePubMedPMC
- 7. Klingenberg C, Muraas FK, Isaksen CE, Nilsen T, Torgersen M, Melum-Hansen C. 2019;Growth and neurodevelopment in very preterm infants receiving a high enteral volume-feeding regimen - a population-based cohort study. J Matern Fetal Neonatal Med 32(10):1664-72. ArticlePubMed
- 8. Fenton TR, Kim JH. 2013;A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr 13:59.ArticlePubMedPMCPDF
- 9. Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, et al. 2005;Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics 116(6):1353-60. ArticlePubMedPDF
- 10. Papile LA, Burstein J, Burstein R, Koffler H. 1978;Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr 92(4):529-34. ArticlePubMed
- 11. Walsh MC, Kliegman RM. 1986;Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am 33(1):179-201. ArticlePubMedPMC
- 12. Stoll BJ, Hansen NI, Sánchez PJ, Faix RG, Poindexter BB, Van Meurs KP, et al. 2011;Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics 127(5):817-26. PubMedPMC
- 13. Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. 2002;Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 110(2 Pt 1):285-91. ArticlePubMedPDF
- 14. Hu F, Tang Q, Wang Y, Wu J, Ruan H, Lu L, et al. 2019;Analysis of nutrition support in very low-birth-weight infants with extrauterine growth restriction. Nutr Clin Pract 34(3):436-43. ArticlePubMedPDF
- 15. Shan HM, Cai W, Cao Y, Fang BH, Feng Y. 2009;Extrauterine growth retardation in premature infants in Shanghai: a multicenter retrospective review. Eur J Pediatr 168(9):1055-9. ArticlePubMedPDF
- 16. Sneve J, Kattelmann K, Ren C, Stevens DC. 2008;Implementation of a multidisciplinary team that includes a registered dietitian in a neonatal intensive care unit improved nutrition outcomes. Nutr Clin Pract 23(6):630-4. ArticlePubMedPDF
- 17. Jeong E, Jung YH, Shin SH, Kim MJ, Bae HJ, Cho YS, et al. 2016;The successful accomplishment of nutritional and clinical outcomes via the implementation of a multidisciplinary nutrition support team in the neonatal intensive care unit. BMC Pediatr 16:113.ArticlePubMedPMCPDF
- 18. Park JA, Park JE, Jeong MJ, Kim JS, Son ES, Eun HS. 2017;Influence of fish oil-containing lipid emulsions on parenteral nutrition- associated liver disease in neonates. J Clin Nutr 9(1):21-9. Article
- 19. Stevens TP, Shields E, Campbell D, Combs A, Horgan M, La Gamma EF, et al. 2018;Statewide initiative to reduce postnatal growth restriction among infants <31 weeks of gestation. J Pediatr 197:82-9. e2. PubMed
- 20. Barker DJ. 2006;Adult consequences of fetal growth restriction. Clin Obstet Gynecol 49(2):270-83. ArticlePubMed
- 21. Pampanini V, Boiani A, De Marchis C, Giacomozzi C, Navas R, Agostino R, et al. 2015;Preterm infants with severe extrauterine growth retardation (EUGR) are at high risk of growth impairment during childhood. Eur J Pediatr 174(1):33-41. ArticlePubMedPDF
- 22. Lee BS. 2015;Nutritional strategy of early amino acid administration in very low birth weight infants. Korean J Pediatr 58(3):77-83. ArticlePubMedPMC
- 23. Dinerstein A, Nieto RM, Solana CL, Perez GP, Otheguy LE, Larguia AM. 2006;Early and aggressive nutritional strategy (parenteral and enteral) decreases postnatal growth failure in very low birth weight infants. J Perinatol 26(7):436-42. ArticlePubMedPDF
- 24. Belfort MB, Ramel SE. 2019;NICU diet, physical growth and nutrient accretion, and preterm infant brain development. Neoreviews 20(7):e385-96. ArticlePubMedPDF
- 25. American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors. 2009;Clinical guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients, 2009. JPEN J Parenter Enteral Nutr 33(3):255-9. ArticlePubMedPDF
- 26. Centers for Disease Control and Prevention (CDC). 2013;Notes from the field: zinc deficiency dermatitis in cholestatic extremely premature infants after a nationwide shortage of injectable zinc - Washington, DC, December 2012. MMWR Morb Mortal Wkly Rep 62(7):136-7. PubMedPMC
- 27. Gupta K, Wang H, Amin SB. 2018;Copper supplementation in premature infants with parenteral nutrition-associated cholestasis. Nutr Clin Pract 33(5):718-24. ArticlePubMedPDF
- 28. Ruktanonchai D, Lowe M, Norton SA, Garret T, Soghier L, Weiss E, et al. 2014;Zinc deficiency-associated dermatitis in infants during a nationwide shortage of injectable zinc - Washington, DC, and Houston, Texas, 2012-2013. MMWR Morb Mortal Wkly Rep 63(2):35-7. PubMedPMC
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Nutrition Supply and Growth Post Nutrition Support Team Activity in Neonatal Intensive Care Unit
Hye Min Ha, Yu Jin Jung, Yoo Rha Hong, So Yoon Choi
Pediatric Gastroenterology, Hepatology & Nutrition.2024; 27(5): 313. CrossRef
 Cite
Cite- Figure
-
Effect of Nutritional Intervention by the Nutrition Support Team on Postnatal Growth in Preterm Infants
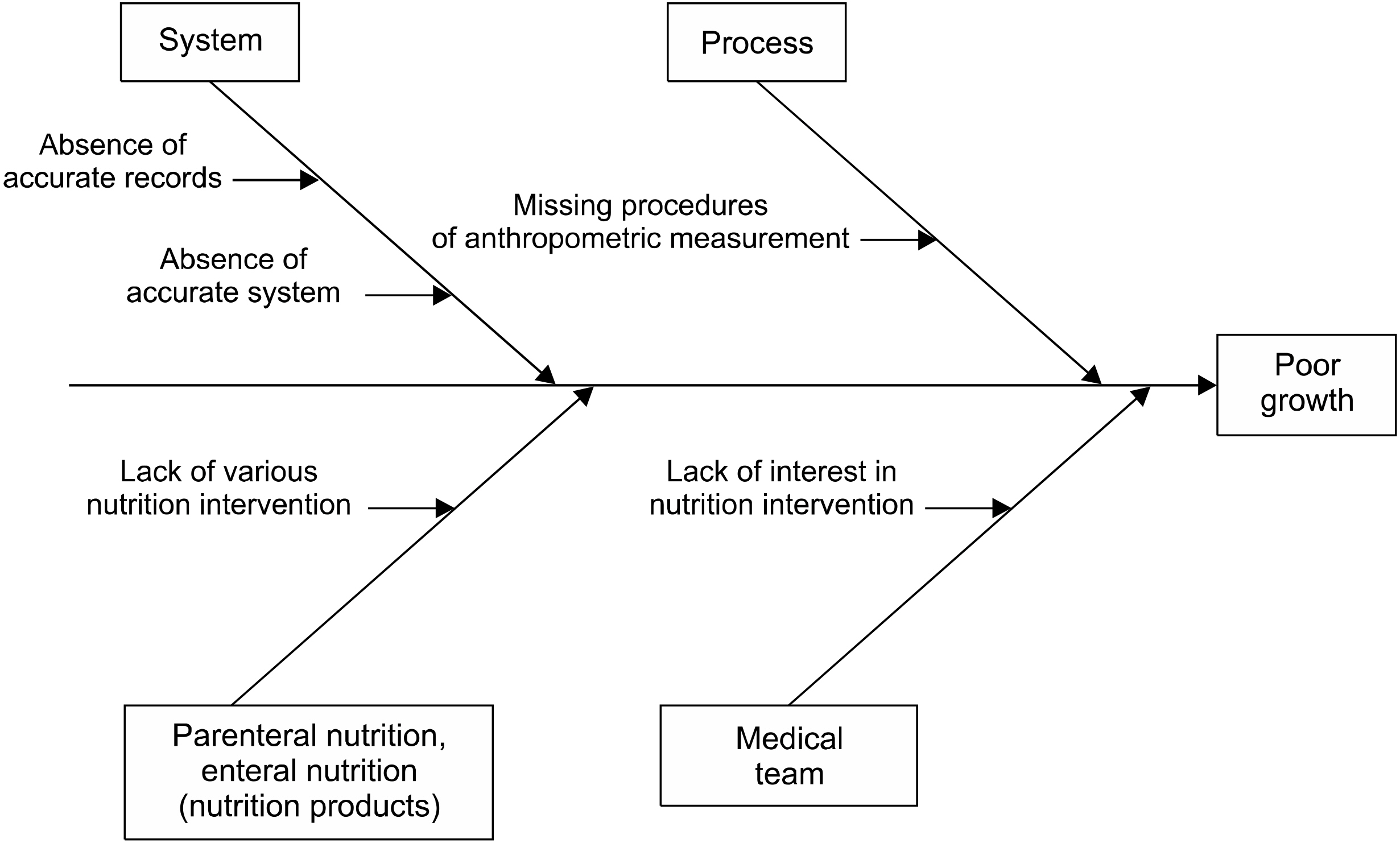
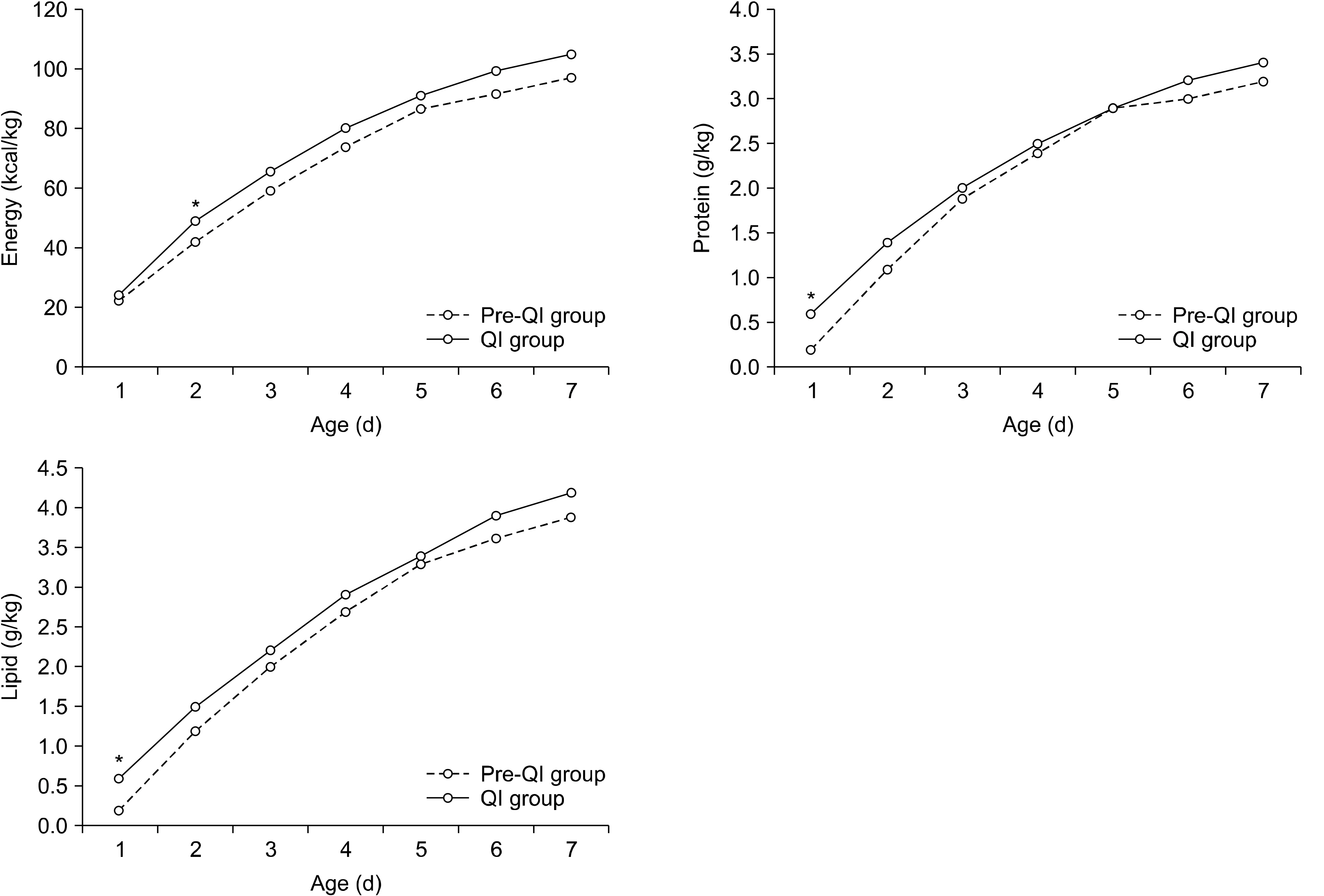
Fig. 1
Fishbone diagram depicting causes of poor growth.
Fig. 2
Comparisons of nutrition components during 1st week after birth between QI and pre-QI groups. QI = quality improvement.
Fig. 1
Fig. 2
Effect of Nutritional Intervention by the Nutrition Support Team on Postnatal Growth in Preterm Infants
Patient characteristics and co-morbidities between pre-QI and QI group
| Variable | Pre-QI group (N=69) | QI group (N=52) | P-value |
|---|---|---|---|
| Gestational age (wk) | 30.8±2.7 | 31.1±3.0 | 0.624 |
| Birth weight (g) | 1,457±382 | 1,528±340 | 0.293 |
| Male, n (%) | 37 (53.6) | 26 (50.0) | 0.693 |
| Cesarean section | 50 (72.5) | 45 (86.5) | 0.062 |
| SGA | 4 (5.8) | 10 (19.2) | 0.041 |
| PROM | 16 (23.5) | 9 (17.3) | 0.406 |
| Chorioamnionitis | 6 (12.2) | 10 (19.2) | 0.599 |
| PIH | 4 (5.8) | 7 (13.5) | 0.203 |
| Maternal DM | 3 (4.3) | 7 (13.5) | 0.097 |
| Prenatal steroid | 19 (35.8) | 14 (26.9) | 0.513 |
| Apgar score 1 min | 4.6±1.8 | 5.0±1.3 | 0.127 |
| Apgar score 5 min | 6.7±1.4 | 6.8±1.2 | 0.686 |
| RDS | 54 (78.3) | 36 (69.2) | 0.260 |
| PDA | 25 (36.2) | 8 (14.5) | 0.007 |
| BPD | 23 (56.1) | 18 (43.9) | 0.943 |
| NEC | 0 | 0 | - |
| Cholestasis | 3 (4.3) | 7 (12.7) | 0.107 |
| Rickets | 7 (10.1) | 6 (10.9) | 0.890 |
| IVH | 11 (15.9) | 2 (3.6) | 0.037 |
| PVL | 8 (11.6) | 0 (0) | 0.009 |
| ROP | 13 (18.8) | 11 (20.0) | 0.871 |
| Sepsis | 5 (7.2) | 1 (1.8) | 0.226 |
| Hospital stay (d) | 52.0±47.4 | 51.5±42.6 | 0.950 |
Values are presented as mean±standard deviation or number (%).
- = not available; QI = quality improvement; SGA = small for gestational age; PROM = premature rupture of amniotic membrane; PIH = pregnancy-induced hypertension; DM = diabetes mellitus; RDS = respiratory distress syndrome; PDA = patent ductus arteriosus; BPD = bronchopulmonary dysplasia; IVH = intraventricular hemorrhage greater or equal to grade 3; PVL = periventricular leukomalacia; NEC = necrotizing enterocolitis; ROP = retinopathy of prematurity.
*P-value<0.05.
Comparisons of nutrition components during 1st week after birth between QI and pre-QI groups
| Nutrition | PND | Pre-QI group (N=78) | QI group (N=64) | P-value |
|---|---|---|---|---|
| Energy (kcal/kg) | 1 | 22.4±7.7 | 24.5±14.5 | 0.341 |
| 2 | 42.2±9.9 | 49.6±9.6 | <0.001 | |
| 3 | 59.4±11.7 | 65.9±12.0 | 0.003 | |
| 4 | 74.0±14.4 | 80.3±13.7 | 0.015 | |
| 5 | 87.0±16.1 | 91.2±15.5 | 0.147 | |
| 6 | 91.5±14.2 | 99.8±17.9 | 0.006 | |
| 7 | 97.5±16.0 | 105.3±17.0 | 0.011 | |
| Total | 473.9±69.3 | 516.6±61.1 | 0.001 | |
| Protein (g/kg) | 1 | 0.2±0.4 | 0.6±0.4 | <0.001 |
| 2 | 1.1±0.5 | 1.4±0.3 | 0.003 | |
| 3 | 1.9±0.4 | 2.0±0.5 | 0.246 | |
| 4 | 2.4±0.5 | 2.5±0.5 | 0.076 | |
| 5 | 2.9±0.5 | 2.9±0.6 | 0.708 | |
| 6 | 3.0±0.5 | 3.2±0.6 | 0.107 | |
| 7 | 3.2±0.5 | 3.4±0.5 | 0.056 | |
| Total | 14.7±2.5 | 16.0±2.4 | 0.004 | |
| Lipid (g/kg) | 1 | 0.2±0.4 | 0.6±0.5 | <0.001 |
| 2 | 1.2±0.6 | 1.5±0.4 | 0.001 | |
| 3 | 2.0±0.5 | 2.2±0.6 | 0.119 | |
| 4 | 2.7±0.7 | 2.9±0.7 | 0.057 | |
| 5 | 3.3±0.8 | 3.4±0.8 | 0.534 | |
| 6 | 3.6±0.8 | 3.9±1.0 | 0.098 | |
| 7 | 3.9±1.0 | 4.2±1.0 | 0.071 | |
| Total | 16.9±3.8 | 18.7±3.5 | 0.007 |
Values are presented as mean±standard deviation.
PND = postnatal day; QI = quality improvement.
Comparisons of nutrition and growth outcome between QI and pre-QI groups
| Nutrition and growth outcomes | Pre-QI group (N=69) | QI group (N=52) | P-value |
|---|---|---|---|
| Time to initiation of enteral feedings (d) | 3.1±2.8 | 1.4±1.6 | <0.001 |
| PN duration (d) | 26.0±29.7 | 24.2±23.1 | 0.711 |
| Time to reach full enteral feedings (d) | 20.0±16.6 | 20.7±19.2 | 0.830 |
| Full EN within 2 weeks, n (%) | 35 (50.7) | 30 (57.7) | 0.447 |
| Birth weight recovery within 2 weeks, n (%) | 50 (72.5) | 39 (75.0) | 0.754 |
| SGA at birth, n (%) | 4 (5.8) | 10 (19.2) | 0.041 |
| Weight <10th percentile at 1 month, n (%) | 25 (36.2) | 16 (30.8) | 0.530 |
| Weight <10th percentile at PCA 40 week, n (%) | 31 (44.9) | 17 (32.7) | 0.173 |
| Weight Z-score at admission | –0.18±0.81 | –0.29±1.25 | 0.603 |
| Height Z-score at admission | –0.31±0.90 | –0.66±1.47 | 0.140 |
| Head circumference Z-score at admission | –0.13±0.93 | –0.44±1.56 | 0.211 |
| Weight Z-score at 1 month | –0.98±1.04 | –0.96±0.98 | 0.904 |
| Height Z-score at 1 month | –2.02±1.55 | –1.73±1.41 | 0.301 |
| Head circumference Z-score at 1 month | –2.51±1.26 | –2.27±1.35 | 0.323 |
| Weight Z-score at PCA 40 week | –1.15±1.18 | –0.73±1.37 | 0.074 |
| Height Z-score at PCA 40 week | –0.84±1.58 | –0.75±1.48 | 0.738 |
| Head circumference Z-score at PCA 40 week | –2.25±1.07 | –1.56±1.20 | 0.005 |
| Changes of weight Z-score at PCA 40 week | –0.97±1.26 | –0.45±1.29 | 0.027 |
| Changes of weight Z-score PCA 1 month | –0.80±0.95 | –0.67±1.18 | 0.516 |
| Changes of height Z-score at PCA 40 week | –0.53±1.46 | –0.09±1.58 | 0.117 |
| Changes of head circumference Z-score at PCA 40 week | –2.06±1.26 | –1.11±1.70 | 0.003 |
Values are presented as mean±standard deviation or number (%).
QI = quality improvement; PN = parenteral nutrition; EN = enteral nutrition; PCA = post conceptional age; SGA = small for gestational age.
Table 1
Patient characteristics and co-morbidities between pre-QI and QI group
Values are presented as mean±standard deviation or number (%). - = not available; QI = quality improvement; SGA = small for gestational age; PROM = premature rupture of amniotic membrane; PIH = pregnancy-induced hypertension; DM = diabetes mellitus; RDS = respiratory distress syndrome; PDA = patent ductus arteriosus; BPD = bronchopulmonary dysplasia; IVH = intraventricular hemorrhage greater or equal to grade 3; PVL = periventricular leukomalacia; NEC = necrotizing enterocolitis; ROP = retinopathy of prematurity. *P-value<0.05.
Table 2
Comparisons of nutrition components during 1st week after birth between QI and pre-QI groups
Values are presented as mean±standard deviation. PND = postnatal day; QI = quality improvement.
Table 3
Comparisons of nutrition and growth outcome between QI and pre-QI groups
Values are presented as mean±standard deviation or number (%). QI = quality improvement; PN = parenteral nutrition; EN = enteral nutrition; PCA = post conceptional age; SGA = small for gestational age.

