 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > J Clin Nutr > Volume 13(1); 2021 > Article
- Original Article Vitamin D Deficiency is Prevalent in Short Bowel Syndrome Patients on Long-Term Parenteral Nutrition Support
-
SungHyo An1
 , Sanghoon Lee1,2, Hyun-Jung Kim2, Hyo Jung Park2, Jeong-Meen Seo1,2
, Sanghoon Lee1,2, Hyun-Jung Kim2, Hyo Jung Park2, Jeong-Meen Seo1,2 - 단장증후군으로 장기간 정맥영양공급을 받는 환자에서 비타민 D 결핍
-
안성효1, 이상훈1,2, 김현정2, 박효정2, 서정민1,2
-
Journal of Clinical Nutrition 2021;13(1):12-16.
DOI: https://doi.org/10.15747/jcn.2021.13.1.12
Published online: June 30, 2021
1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Intestinal Rehabilitation Team, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- Correspondence to Sanghoon Lee https://orcid.org/0000-0002-5086-1461Department of Surgery, Samsung Medical Center, Sungkyunkwan UniversitySchool of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, KoreaTel: +82-2-3410-4025, Fax: +82-2-3410-0040, E-mail: hooni4@skku.edu
• Received: June 20, 2021 • Accepted: June 23, 2021
© 2021, The Korean Society for Parenteral and Enteral Nutrition. All Rights Reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,031 Views
- 8 Download
- 1 Crossref
Abstract
-
Purpose Short bowel syndrome (SBS) is the most common etiology for intestinal failure (IF) and these patients are at high risk of developing micronutrient deficiencies. This study aimed at assessing the level of vitamins in adult SBS patients at different stages of their disease before the initiation of multidisciplinary intestinal rehabilitation.
-
Methods Patient data from November 2015 to March 2017 were retrospectively reviewed. Adult patients who underwent extensive bowel resection and were classified as SBS-IF were selected. Clinical data including age, sex, etiology of IF, biochemical data, nutritional status, nutrition support, and outcome of intestinal rehabilitation were analyzed.
-
Results Nine patients with SBS-IF were included in the analysis. There were 6 male patients and 3 female patients, with a median age of 55.0 years. Vitamin levels were analyzed at 306 days (median) after the development of SBS. At the time of vitamin levels screening, 4 patients were receiving daily intravenous vitamin supplementation. Five patients were not receiving vitamin supplementations, either intravenously or orally. Vitamin B12 was within the normal range in 6 patients and higher than normal in 3 patients. Vitamin D was within the normal range in 3 patients and lower than normal in 6 patients. Vitamin E was within the normal range in 7 patients and higher than normal in 2 patients. Folate was within the normal range in 8 patients (not checked in 1 patient). Ambulatory patients had significantly higher vitamin D levels compared to hospitalized patients (P=0.015).
-
Conclusion Vitamin D levels had decreased in 67% of patients with SBS in Korea, while vitamin B12, folate, and vitamin E deficiencies were rarely seen.
INTRODUCTION
Short bowel syndrome (SBS) is a state of malabsorption and malnutrition as a result of extensive bowel resection due to various causes, including volvulus or thrombosis of mesenteric vessels and recurrent bowel resection for conditions such as Crohn’s disease.1,2 SBS is the most common etiology for intestinal failure in adults and these patients require parenteral nutrition (PN) support to sustain adequate body weight and water balance.2,3 Even with sufficient nutrition support including PN, these patients are at high risk of developing micronutrient deficiencies.4
Vitamins are an essential part of nutrition and is profoundly involved in maintaining homeostasis in areas such as bone mineral metabolism and hematopoiesis.5 Deficiencies in specific vitamins deficiencies may lead to osteopenia, muscle weakness, and fractures. SBS patients exhibit suboptimal levels of vitamins and micronutrient at a high rate during intestinal rehabilitation.6,7 The aim of this study is to assess the level of vitamins in adult SBS patients at different stages of their disease prior to initiation of multidisciplinary intestinal rehabilitation.
MATERIALS AND METHODS
Patient data from the Intestinal Rehabilitation Team (IRT) database at Samsung Medical Center (Seoul, Korea) from November 2015 to March 2017 were retrospectively reviewed. Adult patients who underwent extensive bowel resection and classified as SBS-intestinal failure (IF) were selected. Clinical data including age, sex, etiology of IF, biochemical data, nutritional status, nutrition support, and outcome of intestinal rehabilitation were analyzed.
Management of all patients was done by a multidisciplinary IRT consisting of surgeons, nutritionists, and pharmacists. When a patient is referred to the IRT, the length and structure of remaining bowel, nutritional status of the patient were assessed. The composition and volume of macronutrients, electrolytes, micronutrients to provide to each patient was determined by assessing the malabsorption status of each patient. Oral or enteral nutrition was encouraged and provided whenever it was feasible. The composition of nutrition support and dose adjustments were carried out by the multidisciplinary IRT.
Blood samples were analyzed initially following referral to IRT for a thorough screening of deficiencies or complications related to SBS-IF, including electrolyte imbalance, anemia, hypoglycemia, vitamin deficiencies (vitamin B12, vitamin D, vitamin E, folate), intestinal failure-associated liver disease, and azotemia. When deficiencies or complications were detected, sequential tests were performed according to protocol.8
RESULTS
Nine patients with SBS-IF were included in the analysis (Table 1). There were 6 male patients and 3 female patients, with median age of 55.0 years. Patients were referred to the IRT after 108.0 days (median value) on PN support for SBS. Length of remnant small bowel was 85.0 cm (median). Four patients had end jejunostomies, 4 patients had jejunoileal anastomoses, and 1 patient had a jejunocolic anastomosis. Five patients were 100% PN dependent, while 2 patients each were receiving 80% and 50% of their calories by PN.
Results of vitamin levels screening are presented in Table 2. Vitamin levels were analyzed at 306 days (median) after development of SBS. At the time of vitamin levels screening, 4 patients were receiving daily intravenous vitamin supplementation with a multi-vitamin concentrate (Tamipool; Celltrion Pharm, Cheongju, Korea). The amount of vitamins provided by this product is shown in Table 3. Five patients were not receiving vitamin supplementations, either intravenously or orally. Vitamin B12 was within normal ranges in 6 patients and higher than normal ranges in 3 patients. Vitamin D was within normal ranges in 3 patients and lower than normal ranges in 6 patients. Vitamin E was within normal ranges in 7 patients and higher than normal ranges in 2 patients. Folate was within normal ranges in 8 patients (not checked in 1 patient). Prothrombin time (international normalized ratio) which is a surrogate marker for vitamin K level was within normal ranges in 3 patients and higher than normal ranges in 6 patients, representing low vitamin K levels in these patients (not checked in 1 patient).
Vitamin D levels were compared between patients grouped according to clinical and nutritional variables (Figure 1). Patients who are ambulatory had significantly higher vitamin D levels compared to hospitalized patients (P=0.015, Figure 1E). Vitamin D levels were not different in relation with remnant bowel anatomy, oral intake, prealbumin levels, intravenous vitamin supplementation, and duration since development of SBS.
DISCUSSION
The results of this study illustrate the high prevalence of vitamin D deficiency and relatively sufficient levels of other vitamins in SBS patients. Vitamin D deficiency was consistently seen in SBS patients irrespective of remnant bowel anatomy, oral intake, or intravenous vitamin supplementation. These findings are consistent with previous reports evaluating vitamins and micronutrient levels in SBS patients. In a study by Feng et al.,9 the authors analyzed micronutrient levels in 31 pediatric SBS patients during intestinal rehabilitation. The prevalence of vitamin D deficiency was 93.5%, while vitamin B12 and folate deficiency was not seen in any patients. Risk factor analysis for vitamin D deficiency was done and revealed that remaining bowel length, age, presence of ileocecal valve, duration of PN, and vitamin D supplementation were not significant factors. A study by Ubesie et al.4 included 449 vitamin D measurements in 123 SBS children undergoing intestinal rehabilitation. The prevalence of vitamin D deficiency was 39.8%. The authors also presented bone mineral density measurements data which showed 12.5% prevalence of reduced bone mass.
Patients with intestinal failure due to SBS are a diverse population with much variation in the underlying pathology, remnant intestinal anatomy, and degree of malnutrition. This clinicopathologic diversity leads to a high degree of variation in nutritional demand and a one-size-fits-all approach in management is not sufficient in most cases. Patients’ nutritional management must be tailored to the demands of each patient and provided by a multidisciplinary team of experts.10,11 The positive effects of this multidisciplinary intestinal rehabilitation was elucidated in the study by Feng et al.9 that followed patients with serial vitamin D measurements during an 8-month span. Vitamin D levels significantly improved through the 8-month period and prevalence of vitamin D deficiency among patients decreased. Intensive intestinal rehabilitation and nutritional support by an experienced team of multidisciplinary specialists is believed to be a major contributing factor in these patients’ improvement in micronutrient status.
One interesting finding in this study is the significantly higher vitamin D levels in ambulatory patients compared to hospitalized patients. This is an expected outcome regarding the importance of exposure to ultraviolet rays in sunlight in the metabolism of vitamin D in humans, but one that has been seldom analyzed as contributing factors in previous reports. Hospitalized patients are apt to spend significantly less time under exposure to direct sunlight and vitamin D synthesis would be hindered. Thus, management of SBS patients should focus on advocating enteral intake and reducing PN, so the patient does not require inpatient care, thus reducing the risk of vitamin D deficiency and bone mineral disease that may follow.
This study is the first study to present vitamin measurement results in SBS patients in Korea. Vitamin D levels were decreased in 67% of patients while vitamin B12, folate, and vitamin E deficiencies were rarely seen. Future studies should focus on assessing the metabolic effects of vitamin deficiencies in SBS patients and also on the strategies for prevention of vitamin deficiencies in SBS patients.
Fig. 1
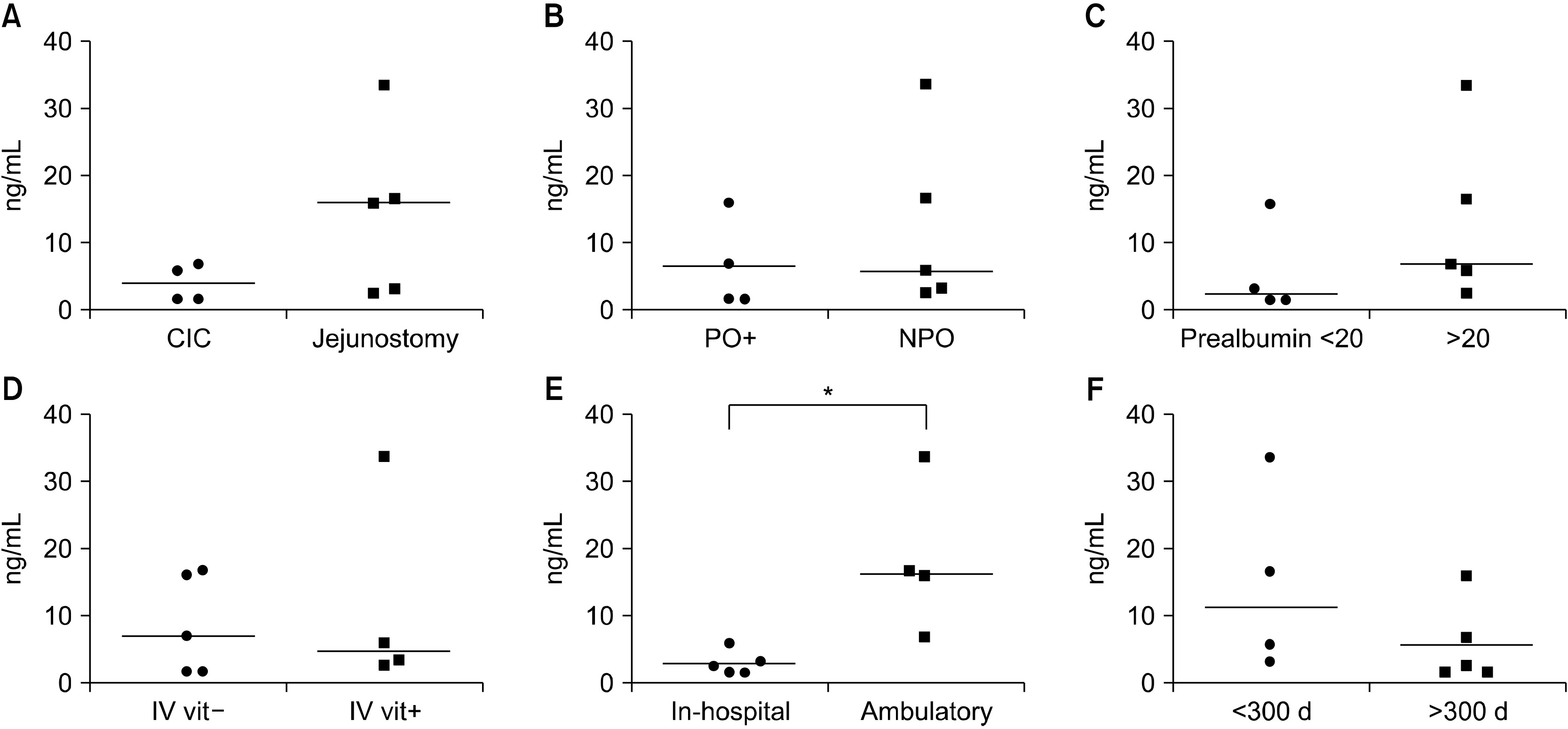
Comparison of vitamin D levels between patient groups according to clinical and nutritional factors. (A) Remnant bowel anatomy, (B) oral intake, (C) prealbumin level, (D) intravenous vitamin supplementation, (E) ambulatory status, (F) days on parenteral nutrition. CIC = colon-in-continuity; PO+ = oral intake; NPO = nothing by mouth; IV vit = intravenous vitamin. *P<0.05.
Table 1
Patient demographics
Table 2
Initial vitamin analysis results
Table 3
Composition of intravenous multi-vitamin concentrate (Tamipool®) and daily requirement of vitamins
- 1. Thompson JS. 2000;Comparison of massive vs. repeated resection leading to short bowel syndrome. J Gastrointest Surg 4(1):101-4. ArticlePubMed
- 2. Pironi L, Arends J, Baxter J, Bozzetti F, Peláez RB, Cuerda C, et al. 2015;ESPEN endorsed recommendations. Definition and classification of intestinal failure in adults. Clin Nutr 34(2):171-80. ArticlePubMed
- 3. Schalamon J, Mayr JM, Höllwarth ME. 2003;Mortality and economics in short bowel syndrome. Best Pract Res Clin Gastroenterol 17(6):931-42. ArticlePubMed
- 4. Ubesie AC, Kocoshis SA, Mezoff AG, Henderson CJ, Helmrath MA, Cole CR. 2013;Multiple micronutrient deficiencies among patients with intestinal failure during and after transition to enteral nutrition. J Pediatr 163(6):1692-6. ArticlePubMedPMC
- 5. Wimalawansa SJ. 2011;Vitamin D: an essential component for skeletal health. Ann N Y Acad Sci 1240:E1-12. ArticlePubMed
- 6. Yang CF, Duro D, Zurakowski D, Lee M, Jaksic T, Duggan C. 2011;High prevalence of multiple micronutrient deficiencies in children with intestinal failure: a longitudinal study. J Pediatr 159(1):39-44.e1. ArticlePubMedPMC
- 7. Thomson P, Duerksen DR. 2011;Vitamin D deficiency in patients receiving home parenteral nutrition. JPEN J Parenter Enteral Nutr 35(4):499-504. ArticlePubMedPDF
- 8. Yoon S, Lee S, Park HJ, Kim HJ, Yoon J, Min JK, et al. 2018;Multidisciplinary intestinal rehabilitation for short bowel syndrome in adults: results in a Korean intestinal rehabilitation team. J Clin Nutr 10(2):45-50. Article
- 9. Feng H, Zhang T, Yan W, Lu L, Tao Y, Cai W, et al. 2020;Micronutrient deficiencies in pediatric short bowel syndrome: a 10-year review from an intestinal rehabilitation center in China. Pediatr Surg Int 36(12):1481-7. ArticlePubMedPDF
- 10. Modi BP, Langer M, Ching YA, Valim C, Waterford SD, Iglesias J, et al. 2008;Improved survival in a multidisciplinary short bowel syndrome program. J Pediatr Surg 43(1):20-4. ArticlePubMedPMC
- 11. Diamond IR, de Silva N, Pencharz PB, Kim JH, Wales PW. 2007;Neonatal short bowel syndrome outcomes after the establishment of the first Canadian multidisciplinary intestinal rehabilitation program: preliminary experience. J Pediatr Surg 42(5):806-11. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- A narrative inquiry into the disease adaptation experience of long-term follow-up patients with short bowel syndrome in Korea
Eun-Mi Seol, Eunjung Kim
Ann Clin Nutr Metab.2025; 17(3): 188. CrossRef
 Cite
CiteVitamin D Deficiency is Prevalent in Short Bowel Syndrome Patients on Long-Term Parenteral Nutrition Support
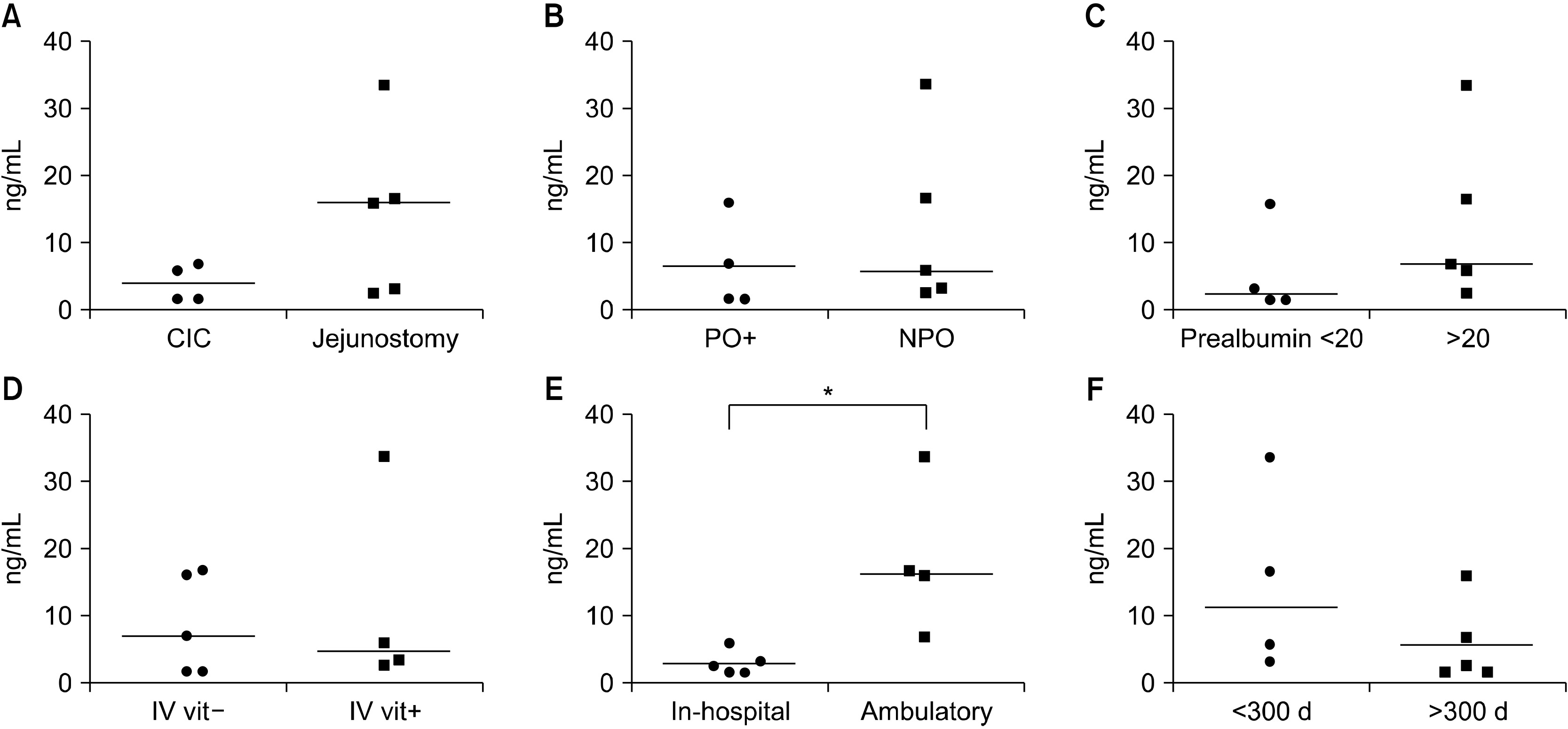
Fig. 1
Comparison of vitamin D levels between patient groups according to clinical and nutritional factors. (A) Remnant bowel anatomy, (B) oral intake, (C) prealbumin level, (D) intravenous vitamin supplementation, (E) ambulatory status, (F) days on parenteral nutrition. CIC = colon-in-continuity; PO+ = oral intake; NPO = nothing by mouth; IV vit = intravenous vitamin. *P<0.05.
Fig. 1
Vitamin D Deficiency is Prevalent in Short Bowel Syndrome Patients on Long-Term Parenteral Nutrition Support
Patient demographics
| Sex | Age (y) | Days from SBS to referral | Bowel anatomy | PN dependence (%) | Prealbumin (20∼40 mg/dL) | Vitamin supplementation | |
|---|---|---|---|---|---|---|---|
| 1 | M | 45 | 701 | Jejunoileal anastomosis | 80 | 10.3 | None |
| 2 | F | 58 | 390 | Jejunocolic anastomosis | 80 | 18.8 | None |
| 3 | F | 43 | 108 | Jejunoileal anastomosis | 50 | 8.6 | None |
| 4 | M | 58 | 2,234 | Jejunoileal anastomosis | 50 | 23.9 | None |
| 5 | M | 67 | 39 | Jejunoileal anastomosis | 100 | 27.7 | Intravenous |
| 6 | M | 51 | 90 | Jejunostomy | 100 | 9.9 | Intravenous |
| 7 | M | 55 | 8 | Jejunostomy | 100 | 27.1 | None |
| 8 | F | 57 | 45 | Jejunostomy | 100 | 27.6 | Intravenous |
| 9 | M | 21 | 314 | Jejunostomy | 100 | 23.3 | Intravenous |
M = male; F = female; SBS = short bowel syndrome; PN = parenteral nutrition.
Initial vitamin analysis results
| Days from SBS to vitamin analysis | Vitamin B12 (160∼970 pg/mL) | Vitamin D (10∼150 ng/mL) | Vitamin E (11.6∼46.4 umol/L) | Folate (1.5∼16.9 ng/mL) | INR (0.9∼1.1) | |
|---|---|---|---|---|---|---|
| 1 | 721 | 852.0 | 1.8 | 15.1 | 5.3 | NA |
| 2 | 391 | 2,925.0 | 16.0 | 15.2 | 5.5 | 1.01 |
| 3 | 306 | 1,529.0 | 1.8 | 24.7 | 7.5 | 1.24 |
| 4 | 2,545 | 174.0 | 7.0 | 28.9 | 15.0 | 1.02 |
| 5 | 89 | 853.0 | 6.0 | 52.8 | 9.5 | 1.11 |
| 6 | 91 | 764.0 | 3.4 | 36.5 | 1.5 | 1.20 |
| 7 | 11 | 529.0 | 16.7 | 36.7 | 6.6 | 1.20 |
| 8 | 54 | 338.0 | 33.5 | 32.0 | NA | 0.99 |
| 9 | 319 | 4,460.0 | 2.7 | 62.4 | 14.8 | 1.41 |
SBS = short bowel syndrome; INR = international normalized ratio; NA = not available.
Composition of intravenous multi-vitamin concentrate (Tamipool®) and daily requirement of vitamins
| Unit | TamipoolⓇ | Daily requirement | |
|---|---|---|---|
| Vitamin A | IU | 3,300 | 3,300 |
| Vitamin D | IU | 200 | 200 |
| Vitamin E | IU | 10 | 10 |
| Vitamin K | mcg | 0 | 150 |
| Vitamin C | mg | 100 | 200 |
| Thiamine | mg | 3.4 | 6 |
| Riboflavin | mg | 2.8 | 3.6 |
| Niacin | mg | 40 | 40 |
| Pantothenic acid | mg | 15 | 15 |
| Pyridoxine | mg | 4.0 | 6 |
| Cyanocobalamin | mcg | 5 | 5 |
| Biotin | mcg | 60 | 60 |
| Folic acid | mcg | 400 | 600 |
Table 1
Patient demographics
M = male; F = female; SBS = short bowel syndrome; PN = parenteral nutrition.
Table 2
Initial vitamin analysis results
SBS = short bowel syndrome; INR = international normalized ratio; NA = not available.
Table 3
Composition of intravenous multi-vitamin concentrate (Tamipool®) and daily requirement of vitamins

