 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Surgical Metabolism and Nutrition > Volume 11(2); 2020 > Article
- Original Article Clinical Impact of Preoperative Sarcopenia to Postoperative Prognosis in Patients with Periampullary Malignancy: Retrospective Multicenter Study
-
Jee Hyun Park, M.D.1
 , Youngju Ryu, M.D.1, So Hee Song, M.D.2, Naru Kim, M.D.1, Sang Hyun Shin, M.D., Ph.D.1, Jin Seok Heo, M.D., Ph.D.1, Dong Wook Choi, M.D., Ph.D.1, Woo Kyoung Jeong, M.D., Ph.D.2, Woo Hyun Jung, M.D.3, Yong Chan Shin, M.D.4, Chang-Sup Lim, M.D., Ph.D.5, In Woong Han, M.D., Ph.D.1
, Youngju Ryu, M.D.1, So Hee Song, M.D.2, Naru Kim, M.D.1, Sang Hyun Shin, M.D., Ph.D.1, Jin Seok Heo, M.D., Ph.D.1, Dong Wook Choi, M.D., Ph.D.1, Woo Kyoung Jeong, M.D., Ph.D.2, Woo Hyun Jung, M.D.3, Yong Chan Shin, M.D.4, Chang-Sup Lim, M.D., Ph.D.5, In Woong Han, M.D., Ph.D.1 -
Surgical Metabolism and Nutrition 2020;11(2):40-45.
DOI: https://doi.org/10.18858/smn.2020.11.2.40
Published online: December 30, 2020
1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Radiology Centre for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
3Department of Surgery, Ajou University Medical Center, Ajou University College of Medicine, Suwon, Korea
4Department of Surgery, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
5Department of Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
- Corresponding author: In Woong Han E-mail cardioman76@gmail.com ORCID https://orcid.org/0000-0001-7093-2469
This study was supported by grant from the KSSMN grant no. 2017-04 and presented at 29th Congress of the KSSMN & 2019 International Symposium, Seoul, Korea.
• Received: April 1, 2020 • Revised: May 22, 2020 • Accepted: June 18, 2020
Copyright © 2020 The Korean Society of Surgical Metabolism and Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 995 Views
- 1 Download
Abstract
-
Purpose This study compared the preoperative nutritional status between sarcopenic and non-sarcopenic patients and examined the effects of sarcopenia on the prognosis after a pancreatoduodenectomy (PD).
-
Materials and Methods From 2015 to 2016, 480 patients who underwent PD with periampullary cancer at Samsung Medical Center, Seoul National University Boramae Medical Center, Ilsan Paik Hospital, and Ajou University Hospital were analyzed retrospectively. Sarcopenia was measured from the cross-sectional visceral fat and muscle area on CT imaging using an automatic calculation program. The dysnutritional grade was assessed according to Controlling Nutritional Status (CONUT) score system.
-
Results Preoperative serum albumin (3.9 g/dl) and cholesterol levels (161.7 mg/dl) of sarcopenic patients were significantly lower than those of the non-sarcopenia patients (4.0 g/dl, P=0.024; 176.1 mg/dl, P=0.005). The proportion of moderate-to-severe dysnutritional grade in sarcopenic patients was significantly higher than in the non-sarcopenic patients (20.0 vs. 8.1%, P=0.004). A comparison of the changes in albumin between before and after PD showed a decrease in sarcopenic patients (0.06 vs. 0.05, P=0.024). Sarcopenia itself was not a factor affecting the overall survival (OS) negatively, but moderate-to-severe dysnutritional grade was an independent risk factor for OS (HR 2.418, CI 1.424~4.107, P=0.001).
-
Conclusion Patients with sarcopenia showed poorer preoperative nutritional status than those without sarcopenia, and the sarcopenia affected the postoperative nutritional status negatively. No direct correlation was observed between sarcopenia and OS, but the dysnutritional grade was an independent risk factor that affects OS. As a result, patients with sarcopenia could be affected indirectly for survival because of their poor nutritional status.
INTRODUCTION
Sarcopenia, derived from the Greek words, “sarx,” meaning flesh, and “penia,” meaning loss, was introduced in the late 1980s and is now a broadly used medical term.[1] Sarcopenia is currently understood as a decrease in body muscle mass associated with aging. Several studies describe it as a poor prognostic factor for physical activity, quality of life, and survival time, which is diagnosed by a decrease in body muscle mass, muscle strength, and physical activity.[2-4]
Pancreatoduodenectomy (PD) and pylorus-preserving PD (PPPD) are standard surgical procedures for removing various periampullary tumors.[5,6] Lately, due to improvements in surgical techniques and pre- and postoperative management, the postoperative mortality rates of pancreatic resection at institutions with high surgical volume have decreased significantly to 1% but remain higher in other types of surgeries. Additionally, the preoperative nutritional states of patients tend to be poor, and the areas of surgical resection tend to be much more extensive than other surgeries, leading to complication rates of up to 60%.[7,8] Therefore, efforts in determining prognostic factors to improve surgical outcomes should not be overemphasized.
Several studies show sarcopenia as a prognostic factor in various clinical settings, but this is a poor prognostic factor for key indicators such as postoperative complications, length of stay, and survival rate in patients with abdominal surgical and non-surgical diseases.[9-12] Aside from a few reports, its clinical importance is relatively unknown in patients with periampullary tumors undergoing PD.[13,14] Therefore, this multi-institutional, retrospective study aims to analyze the clinical effects of preoperative sarcopenia on patients after PD and its prognostic value.
MATERIALS AND METHODS
From January 2015 to December 2016, a multi-institutional retrospective study was performed on patients who underwent PD for periampullary tumors at the Samsung Seoul Hospital, SNU Boramae Medical Center, AJOU University School of Medicine, and INJE University Ilsan Paik Hospital. Excluding patients with metastatic or multiple primary cancers and those without analyzable computed tomography (CT) before surgery, a total of 480 patients were included in the final analysis. Clinical and laboratory data such as age, gender, diagnosis, postoperative survival time, preoperative and six-month postoperative weights, body mass index (BMI), serum albumin, and cholesterol were collected. A separate web-based data storage program (MDB©, Seoul, South Korea) was used for data collection. Every step of the study was carried out after the approval of the Institutional Review Board (SMC 2017-10-028).
All CT images were analyzed in the portal phase. Analysis of CT images for diagnosing sarcopenia was performed at the Samsung Seoul Hospital Radiology Department using Matlab version R2010a (Mathworks Inc., Natick, MA, USA) to calculate subcutaneous fat, muscle mass, and visceral fat levels. The preprocessed CT image was divided into internal and external CT images using the detected muscle boundary. This step was followed by the division of the CT image pixel into four clusters using a fuzzy c-means clustering algorithm based on the pixel’s Hounsfield unit (HU). In the cluster, background pixels, subcutaneous fat, muscles, and bones were included. Using a ?300 HU~?50 HU threshold in the CT image, the visceral fat was differentiated, and the area was measured by multiplying the number of pixels and the pixel surface area of each type (subcutaneous fat, muscle, and visceral fat) at the lumbar (L3) level. Using the CT analysis method, sarcopenia was defined using the skeletal muscle index (SMI) at L3 level below 50.18 cm2/m2 for men, and 38.63 cm2/m2 for women.[15,16]
The controlling nutritional status (CONUT) score, introduced in 2005, is a widely used tool for detecting and evaluating patients’ dysnutrition state.[17] This score is composed of serum albumin (g/dl), cholesterol (mg/dl), and absolute lymphocyte count, which is divided into normal, mild, moderate, and severe states based on the total score.
Continuous variables were expressed with median and range and analyzed with a t-test or a Mann-Whitney U-test. Categorical variables were compared using the χ2 test or Fisher’s exact test, and survival models were analyzed using Kaplan-Meier and Cox proportional hazard model. The risk factor analysis was performed using logistic regression analysis, and statistical significance was set at P<0.05. All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS 23-Statistical Package for Social Science, version 23.0, IBM Corporation, Chicago, IL, USA).
RESULTS
A total of 480 patients from four institutions were divided into 221 sarcopenia patients and 259 non-sarcopenia patients using SMI. There was no significant difference in age, diagnoses, and surgical methods between the two groups. However, in the sarcopenia group, the proportion of men was significantly higher (62.1% vs. 37.9%, P<0.001), while weight (59.8 vs. 62.6 kg, P=0.007) and BMI (21.9 vs. 24.6 kg/m2, P<0.001) were significantly lower than the non-sarcopenia group. Meanwhile, the preoperative serum albumin and cholesterol levels were significantly lower in the sarcopenia group compared to the non-sarcopenia group (albumin 3.9 vs. 4.0 g/dl P=0.024; cholesterol 161.7 vs. 176.1 mg/dl, P=0.005). As for the CONUT score, the ratio of the moderate-to-severe state over the normal-to-mild state was significantly higher in the sarcopenia group (14.0 vs. 8.1%, P=0.004) (Table 1).
The evaluation of nutritional indicators such as preoperative and six-month postoperative weight, BMI, serum albumin, and serum cholesterol showed that serum albumin levels were significantly lower in the sarcopenia group (0.06 vs. 0.05, P=0.024) (Table 2).
The five-year survival rate was 80.5% in the sarcopenia group compared to 78.8% in the non-sarcopenia group, showing no significant difference after surgery (Fig. 1). However, when performing survival analysis based on preoperative dysnutrition grade with a worsening CONUT score, the survival rate decreased significantly (Fig. 2). Based on the result, risk factor analysis for postoperative survival time was performed. In the univariate analysis, low preoperative serum albumin (Hazard Ratio 1.647, 95% CI 1.105~1.463, P=0.014), low cholesterol levels (HR 1.004, 95% CI 1.001~1.009, P=0.046), and a moderate state or worse CONUT score (HR 2.546, 95% CI 1.538~4.214, P<0.001) were shown to be risk factors for the postoperative survival time. In the multivariate analysis, a CONUT score with moderate state or worse (HR 2.418, 95% CI 1.424~4.107, P=0.001) alone was shown to be the independent risk factor (Table 3).
DISCUSSION
Several nutritional indicators, including weight, BMI, preoperative serum albumin, and serum cholesterol, were poor in the sarcopenia group compared to the non-sarcopenia group, and the ratio of the moderate-to-severe state over the normal-to-mild state was higher in the sarcopenia group (Table 1). This study found that the correlation between sarcopenia and poor nutritional state was similar to the results in previous studies, and poor nutritional state, regardless of the cancer’s progression, caused severe muscle loss, even in obese patients.[18,19] Therefore, a thorough evaluation of the nutritional state of patients with sarcopenia is necessary.
When evaluating nutritional indicators such as preoperative and six-month postoperative weight, BMI, serum albumin, and serum cholesterol, serum albumin was significantly lower in the sarcopenia group (0.06 vs. 0.05, P=0.024; Table 2) and there was no statistical difference between weight and BMI. According to a report from South Korea in 2013, the post-PD recovery period was 6 months in benign diseases and longer than 6 months in malignant diseases.[20] Patients regain their normal weights 2~3 months after surgery and their preoperative weights after 6 months. Aside from sarcopenia, factors influencing weight change may be related to chemoradiation therapy, and further studies assessing the effects of sarcopenia on postoperative weight change are necessary.
Most patients requiring PD experienced dysnutrition during diagnosis or after surgery due to exocrine dysfunction, which caused them to undergo pancreatic exocrine replacement treatment (PERT).[21,22] This treatment not only supports recovering exocrine function but also increases survival rate in patients who underwent PD, as evidenced by a retrospective study of 469 patients from 2007 to 2015 that reported a hazard ratio of 0.75 (95% confidence interval 0.57~0.99, P=0.046).[23] In this study, preoperative dysnutrition was a risk factor affecting the survival rate, which can be increased by improving the patient’s pre- and postoperative nutritional state (Fig. 2, Table 3).
There was no direct causal relationship between sarcopenia and postoperative survival time among patients with periampullary tumors who underwent PD (Fig. 1, Table 3). However, the sarcopenia group had a poorer nutrition state (Table 1), and a low CONUT score was associated with lower postoperative survival rate (Fig. 2, Table 3). Thus, sarcopenia indirectly affects postoperative prognosis. In recent years, some studies on sarcopenia, PD, and periampullary tumors reported on the characteristics of PD and periampullary tumors with higher postoperative mortality rates and identified sarcopenia as an important prognostic factor. In a 2012 pancreatic adenocarcinoma study, sarcopenia was defined using total psoas muscles; based on the three-year survival rate, preoperative sarcopenia was identified as an independent prognostic factor.[13] This pattern is found not in patients with PD from pancreatic carcinomas but from other periampullary tumors.[24] In other diseases, sarcopenia is a poor prognostic factor for survival time. For example, in a 2013 study of 1,473 patients with digestive or pulmonary malignancy, sarcopenia, regardless of the patient’s weight, was a poor prognostic factor.[25] The meta-analysis of patients with cirrhosis also found sarcopenia as a poor prognostic factor in the development of cirrhotic complications, and such a pattern was more commonly found in Asian patients, including Koreans.[9] Based on these findings, a meta-analysis recently found that sarcopenia was a predictor of all types of mortalities in elderly patients, and advanced diagnosis and treatment would lead to an improved overall prognosis.[10,26] Sarcopenia is one of the prognostic factors of survival rate for patients with periampullary tumors or who underwent PD.[24,27,28]
This study is limited as it was a retrospective study with a short follow up period, and it excluded numerous variables, including complications. However, to complement the short follow up period, numerous patient cohorts from several institutions were utilized. Additionally, when analyzing risk factors for patient survival rate, a multivariate analysis should be performed using pathologic risk factors, including the TNM stage. However, this study included patients who underwent PD for various periampullary tumors, including cancers in the head of the pancreas, the duodenum, or the ampullary or biliary tracts. The pathologic risk factor analysis was excluded from the survival rate analysis because the staging system and diagnostic criteria are different depending on the type of cancer. In future studies, cancers should be separated into different types, before proceeding with pathologic risk factor analysis. Lastly, dysnutrition and sarcopenia were used to evaluate a patient’s nutritional state. According to the European Working Group on Sarcopenia in Older People (EWGSOP), three categories (muscle mass, muscle strength, and physical activity), must be evaluated when measuring sarcopenia.[2,29,30] Follow-up studies should include prospective evaluations of muscle strength and physical strength.
CONCLUSION
Dysnutrition with a moderate or severe state was shown to be the one of risk factors determining the survival rate of patients who underwent PD for periampullary tumors. Specifically, there was an assoication between patients in the dysnutrition with a moderate or severe state among the sarcopenia group and the survival rate of patients. Therefore, patients with preoperative sarcopenia would need to be monitored and managed more thoroughly.
ACKNOWLEDGMENTS
This study was supported by grant from the KSSMN grant no. 2017-04. We thank the study research nurse, Hyemin Kim at Samsung Medical Center, for her tremendous work in the acquisition of data.
Fig. 1
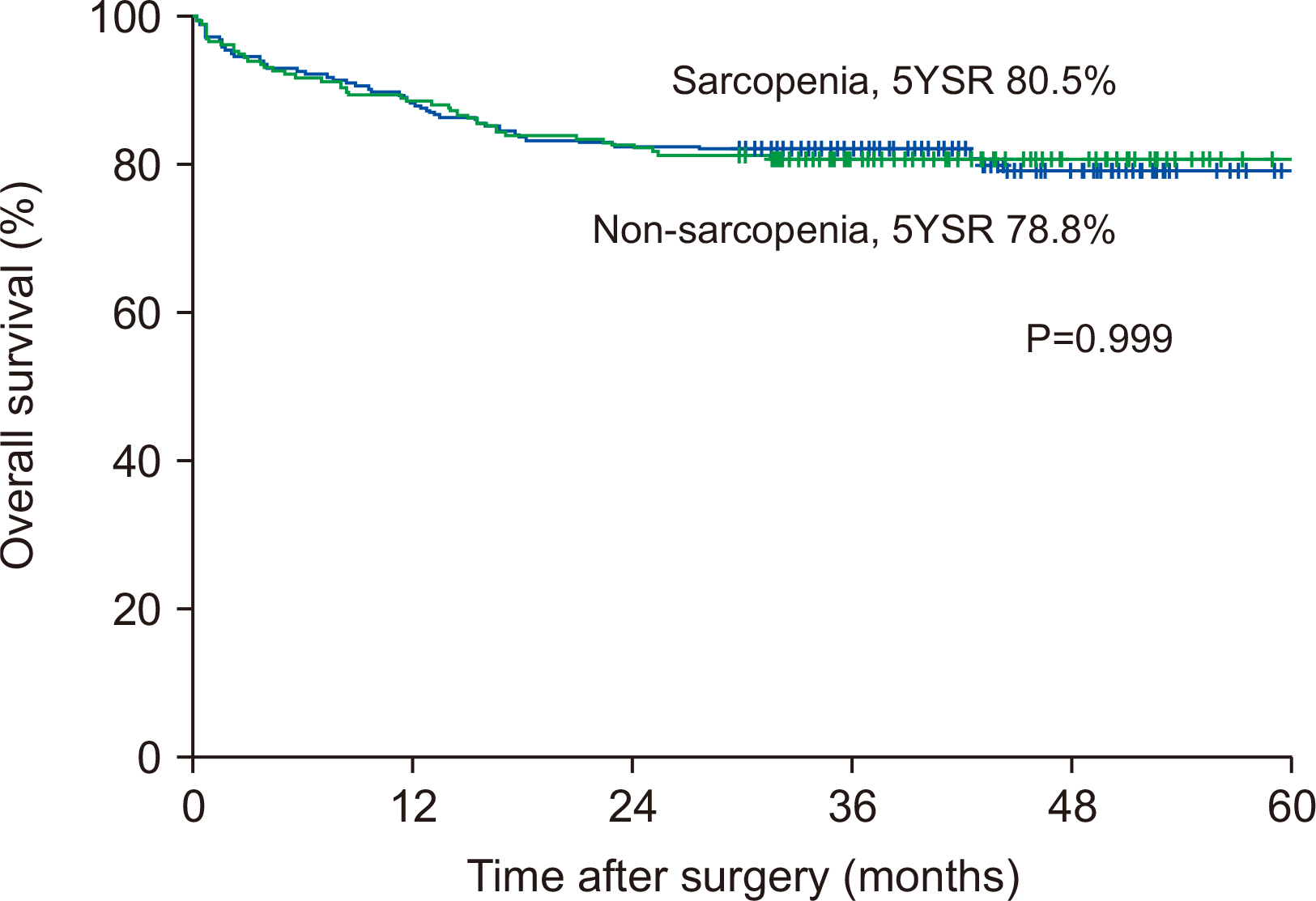
Survival curves of overall survival according to sarcopenia or not 5YSR, 5-years survival rate.
Fig. 2
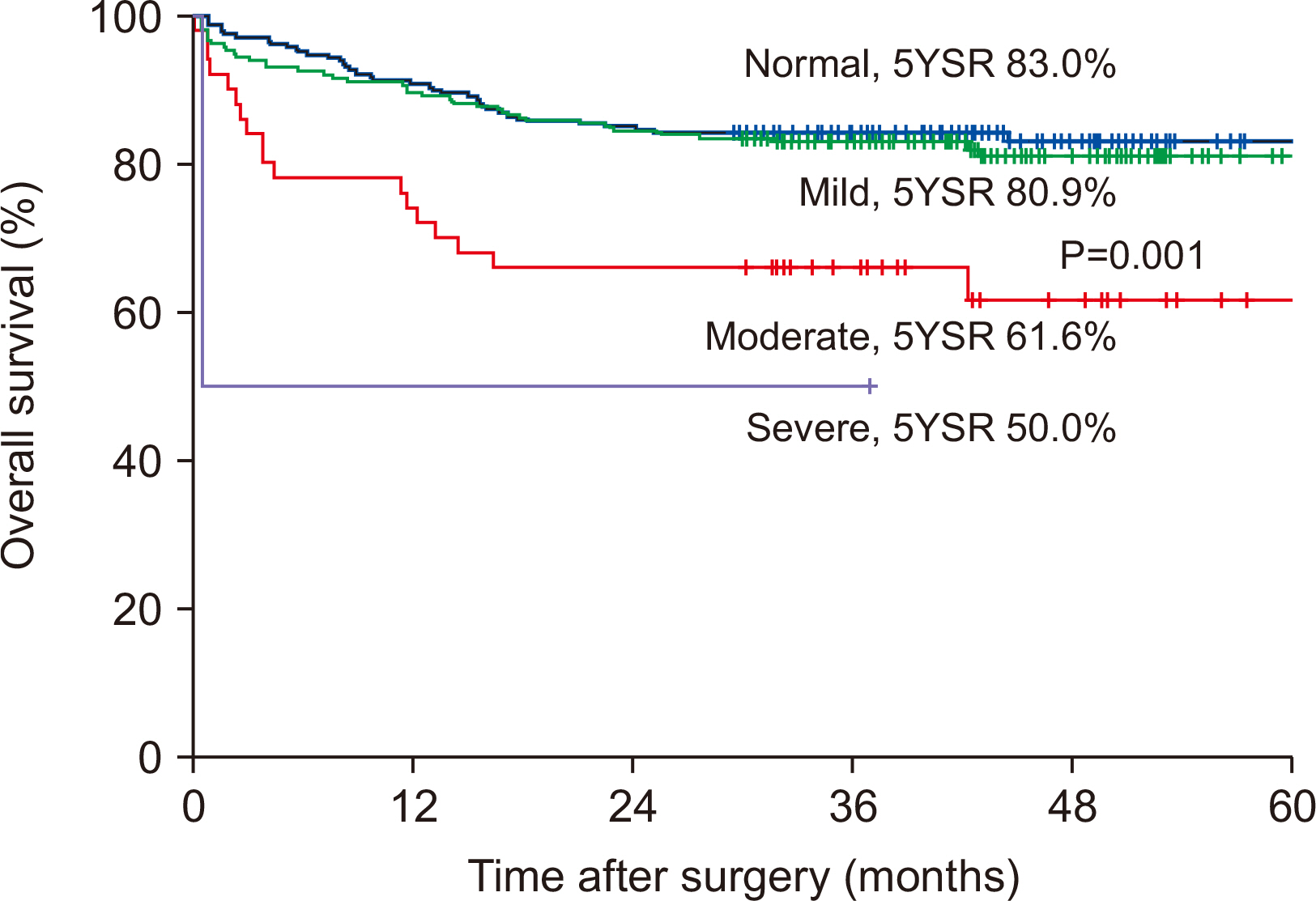
Survival curves of overall survival according to dysnutritional grade 5YSR, 5-years survival rate.
Table 1
Characteristics of enrolled patients
Table 2
Perioperative change of nutritional parameters in patients with or without sarcopenia
Table 3
Uni- and multivariate risk factors analysis for overall survival
- 1. Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr 1997;127(5 Suppl):990S-1S. ArticlePubMed
- 2. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. 2010;European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in older people. Age Ageing 39:412-23. PubMedPMC
- 3. Fielding RA, Vellas B, Evans WJ, Bhasin S, Morley JE, Newman AB, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc 2011;12:249-56. ArticlePubMedPMC
- 4. Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2014;15:95-101. ArticlePubMed
- 5. Turaga K, Kaushik M, Forse RA, Sasson AR. In hospital outcomes after pancreatectomies: an analysis of a national database from 1996 to 2004. J Surg Oncol 2008;98:156-60. ArticlePubMed
- 6. Krautz C, Nimptsch U, Weber GF, Mansky T, Grützmann R. Effect of hospital volume on in-hospital morbidity and mortality following pancreatic surgery in Germany. Ann Surg 2018;267:411-7. ArticlePubMed
- 7. La Torre M, Ziparo V, Nigri G, Cavallini M, Balducci G, Ramacciato G. Malnutrition and pancreatic surgery: prevalence and outcomes. J Surg Oncol 2013;107:702-8. ArticlePubMedPDF
- 8. Bozzetti F, Mariani L. Perioperative nutritional support of patients undergoing pancreatic surgery in the age of ERAS. Nutrition 2014;30:1267-71. ArticlePubMed
- 9. Kim G, Kang SH, Kim MY, Baik SK. Prognostic value of sarcopenia in patients with liver cirrhosis: a systematic review and meta-analysis. PLoS One 201712::e0186990. Article
- 10. Tian S, Xu Y. Association of sarcopenicobesity with the risk of all-cause mortality: a meta-analysis of prospective cohort studies. Geriatr Gerontol Int 2016;16:155-66. ArticlePubMed
- 11. Shen Y, Hao Q, Zhou J, Dong B. The impact of frailty and sarcopenia on postoperative outcomes in older patients undergoing gastrectomy surgery: a systematic review and meta-analysis. BMC Geriatr 2017;17:188.ArticlePubMedPMCPDF
- 12. Jones K, Gordon-Weeks A, Coleman C, Silva M. Radiologically determined sarcopenia predicts morbidity and mortality following abdominal surgery: a systematic review and meta-analysis. World J Surg 2017;41:2266-79. ArticlePubMedPMCPDF
- 13. Peng P, Hyder O, Firoozmand A, Kneuertz P, Schulick RD, Huang D, et al. Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma. J Gastrointest Surg 2012;16:1478-86. ArticlePubMedPMCPDF
- 14. Joglekar S, Asghar A, Mott SL, Johnson BE, Button AM, Clark E, et al. Sarcopenia is an independent predictor of complications following pancreatectomy for adenocarcinoma. J Surg Oncol 2015;111:771-5. ArticlePubMedPDF
- 15. Moon JH, Kim KM, Kim JH, Moon JH, Choi SH, Lim S, et al. Predictive Values of the new sarcopenia index by the Foundation for the National Institutes of Health Sarcopenia Project for mortality among older Korean adults. PLoS One 2016;11:e0166344. ArticlePubMedPMC
- 16. Mourtzakis M, Prado CM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE. 2008;A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab 33:997-1006. ArticlePubMed
- 17. Ignacio de Ulíbarri J, González-Madroño A, de Villar NG, González P, González B, Mancha A, et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp 2005;20:38-45.
- 18. Cruz-Jentoft AJ, Kiesswetter E, Drey M, Sieber CC. Nutrition, frailty, and sarcopenia. Aging Clin Exp Res 2017;29:43-8. ArticlePubMedPDF
- 19. Prado CM, Purcell SA, Laviano A. Nutrition interventions to treat low muscle mass in cancer. J Cachexia Sarcopenia Muscle 202011:366-80. ArticlePDF
- 20. Park JW, Jang JY, Kim EJ, Kang MJ, Kwon W, Chang YR, et al. Effects of pancreatectomy on nutritional state, pancreatic function and quality of life. Br J Surg 2013;100:1064-70. ArticlePubMedPDF
- 21. Sikkens EC, Cahen DL, de Wit J, Looman CW, van Eijck C, Bruno MJ. Prospective assessment of the influence of pancreatic cancer resection on exocrine pancreatic function. Br J Surg 2014;101:109-13. ArticlePubMedPDF
- 22. Nikfarjam M, Wilson JS, Smith RC. Australasian Pancreatic Club Pancreatic Enzyme Replacement Therapy Guidelines Working Group. Diagnosis and management of pancreatic exocrine insufficiency. Med J Aust 2017;207:161-5. ArticlePubMedPDF
- 23. Roberts KJ, Schrem H, Hodson J, Angelico R, Dasari BVM, Coldham CA, et al. Pancreas exocrine replacement therapy is associated with increased survival following pancreatoduodenectomy for periampullary malignancy. HPB (Oxford) 2017;19:859-67. ArticlePubMed
- 24. Onesti JK, Wright GP, Kenning SE, Tierney MT, Davis AT, Doherty MG, et al. Sarcopenia and survival in patients undergoing pancreatic resection. Pancreatology 2016;16:284-9. ArticlePubMed
- 25. Martin L, Birdsell L, Macdonald N, Reiman T, Clandinin MT, McCargar LJ, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol 2013;31:1539-47. ArticlePubMed
- 26. Liu P, Hao Q, Hai S, Wang H, Cao L, Dong B. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: a systematic review and meta-analysis. Maturitas 2017;103:16-22. ArticlePubMed
- 27. Amini N, Spolverato G, Gupta R, Margonis GA, Kim Y, Wagner D, et al. Impact total psoas volume on short- and long-term outcomes in patients undergoing curative resection for pancreatic adenocarcinoma: a new tool to assess sarcopenia. J Gastrointest Surg 2015;19:1593-602. ArticlePubMedPMCPDF
- 28. Pecorelli N, Capretti G, Sandini M, Damascelli A, Cristel G, De Cobelli F, et al. Impact of sarcopenic obesity on failure to rescue from major complications following pancreaticoduodenectomyfor cancer: results from a multicenter study. Ann Surg Oncol 2018;25:308-17. ArticlePubMedPDF
- 29. Chien MY, Huang TY, Wu YT. Prevalence of sarcopenia estimated using a bioelectrical impedance analysis prediction equation in community-dwelling elderly people in Taiwan. J Am Geriatr Soc 2008;56:1710-5. ArticlePubMed
- 30. Kyle UG, Genton L, Hans D, Karsegard VL, Michel JP, Slosman DO, et al. Total body mass, fat mass, fat-free mass, and skeletal muscle in older people: cross-sectional differences in 60-year-old persons. J Am Geriatr Soc 2001;49:1633-40. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteClinical Impact of Preoperative Sarcopenia to Postoperative Prognosis in Patients with Periampullary Malignancy: Retrospective Multicenter Study
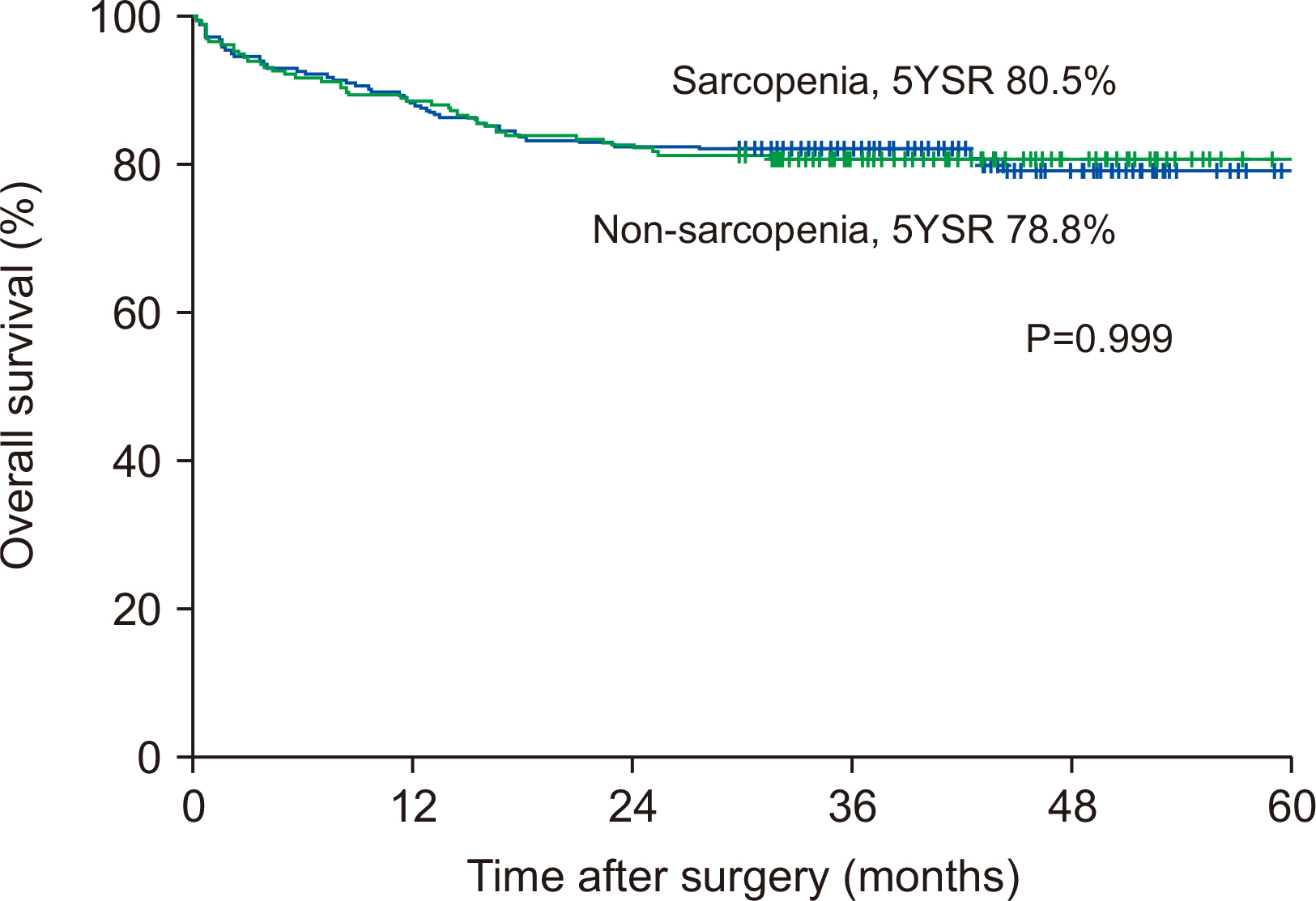
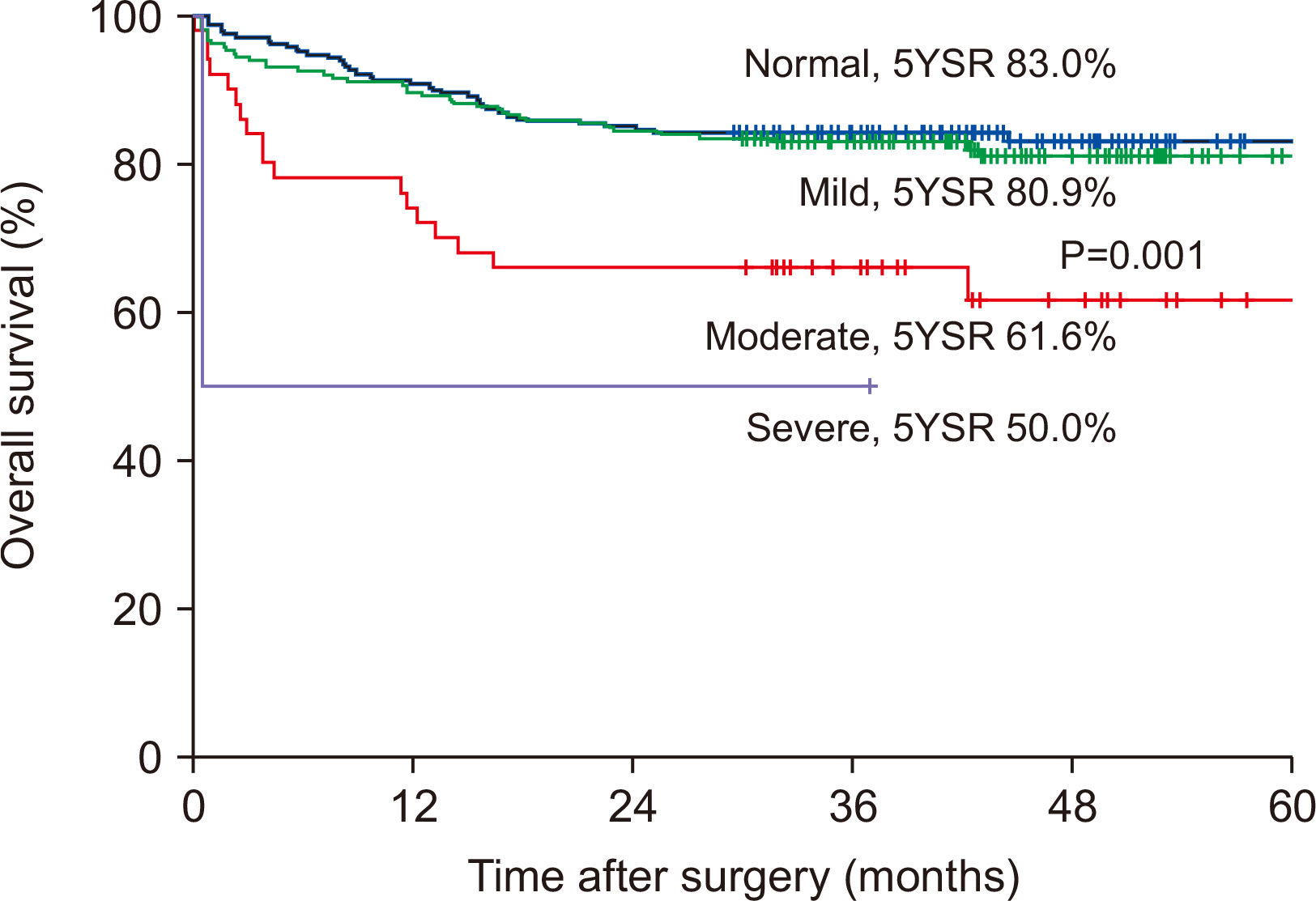
Fig. 1
Survival curves of overall survival according to sarcopenia or not 5YSR, 5-years survival rate.
Fig. 2
Survival curves of overall survival according to dysnutritional grade 5YSR, 5-years survival rate.
Fig. 1
Fig. 2
Clinical Impact of Preoperative Sarcopenia to Postoperative Prognosis in Patients with Periampullary Malignancy: Retrospective Multicenter Study
Characteristics of enrolled patients
| Total (n=480) | Non-sarcopenia (n=259) | Sarcopenia (n=221) | P | |
|---|---|---|---|---|
| Age (years) | 64.5 (14~92) | 64.0 (31~92) | 65.2 (14~89) | 0.189 |
| Sex | <0.001 | |||
| Male, n (%) | 272 (56.7) | 103 (37.9) | 169 (62.1) | |
| Female, n (%) | 208 (43.3) | 156 (75.0) | 52 (25.0) | |
| Body weight (kg) | 61.3 (31.4~95.5) | 62.6 (38.4~95.5) | 59.8 (31.4~88.0) | 0.007 |
| BMI (kg/m2) | 23.3 (14.2~38.5) | 24.6 (17.3~38.5) | 21.9 (14.2~30.0) | <0.001 |
| Serum albumin, preoperative (g/dl) | 3.92 (2.1~5.4) | 4.0 (2.4~5.4) | 3.9 (2.1~5.0) | 0.024 |
| Serum cholesterol, preoperative (mg/dl) | 170.3 (1~508) | 176.1 (39~508) | 161.7 (1~295) | 0.005 |
| Dysnutritional grade | 0.004 | |||
| Normal | 222 (46.3) | 133 (51.4) | 89 (40.3) | |
| Mild | 206 (42.9) | 105 (40.5) | 101 (45.7) | |
| Moderate | 50 (10.4) | 21 (8.1) | 29 (13.1) | |
| Severe | 2 (0.4) | 0 (0) | 2 (0.9) | |
| Diseases | 0.372 | |||
| Pancreas head cancer | 203 (42.3) | 112 (43.2) | 91 (41.2) | |
| Distal CBD cancer | 130 (27.1) | 66 (25.5) | 64 (29.0) | |
| Mid CBD cancer | 22 (4.6) | 15 (5.8) | 7 (3.2) | |
| AoV cancer | 99 (20.6) | 56 (21.6) | 43 (19.5) | |
| Duodenal cancer | 20 (4.2) | 8 (3.1) | 12 (5.4) | |
| Surgery | ||||
| PPPD | 351 (73.1) | 189 (73.0) | 162 (73.3) | |
| PRPD | 80 (16.7) | 49 (18.9) | 31 (14.0) | |
| Whipple’s operation | 47 (9.8) | 21 (8.1) | 26 (11.8) |
BMI = body mass index; CBD = common bile duct; AoV = ampulla of Vater; PPPD = pylorus-preserving pancreatoduodenectomy; PRPD = pylorus-resecting pancreatoduodenectomy.
Perioperative change of nutritional parameters in patients with or without sarcopenia
| Variables difference | Total (n=480) | Non-sarcopenia (n=259) | Sarcopenia (n=221) | P |
|---|---|---|---|---|
| Δ Body weight | 3.67 (–47.10~39.80) | 3.29 (–47.10~26.75) | 4.01 (–15.54~39.8) | 0.493 |
| Δ BMI | 1.34 (–21.80~11.63) | 1.38 (–21.80~10.62) | 1.26 (–8.34~11.63) | 0.075 |
| Δ Albumin | 0.05 (–1.9~3.6) | 0.05 (–1.6~3.6) | 0.06 (–1.9~1.8) | 0.024 |
| Δ Cholesterol | 30.71 (–208~275) | 34.04 (–208~275) | 25.84 (–146~156) | 0.948 |
Δ Value at preoperative time minus value at postoperative 6 months.
BMI = Body mass index.
Uni- and multivariate risk factors analysis for overall survival
| Variables | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | P | HR | 95% CI | P | |
| Age | 1.014 | 0.994~1.035 | 0.167 | |||
| Male | 1.250 | 0.824~1.894 | 0.294 | |||
| BMI | 0.979 | 0.917~1.046 | 0.529 | |||
| Preoperative low albumin level (<3.5 g/dl) | 1.647 | 1.105~1.463 | 0.014 | 1.048 | 0.570~1.598 | 0.859 |
| Preoperative low cholesterol level (<170 mg/dl) | 1.004 | 1.001~1.009 | 0.046 | 1.002 | 0.993~1.002 | 0.295 |
| Sarcopenia | 1.000 | 0.666~1.501 | 0.999 | |||
| Dysnutritional grade (≥moderate, severe) | 2.546 | 1.538~4.214 | <0.001 | 2.418 | 1.424~4.107 | 0.001 |
BMI = Body mass index.
Table 1
Characteristics of enrolled patients
BMI = body mass index; CBD = common bile duct; AoV = ampulla of Vater; PPPD = pylorus-preserving pancreatoduodenectomy; PRPD = pylorus-resecting pancreatoduodenectomy.
Table 2
Perioperative change of nutritional parameters in patients with or without sarcopenia
Δ Value at preoperative time minus value at postoperative 6 months. BMI = Body mass index.
Table 3
Uni- and multivariate risk factors analysis for overall survival
BMI = Body mass index.

