 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 14(1); 2022 > Article
- Review Article Liver Cirrhosis and Sarcopenia
-
Hye Yeon Chon, M.D.
 , Tae Hee Lee, M.D., Ph.D.
, Tae Hee Lee, M.D., Ph.D. -
DOI: https://doi.org/10.15747/ACNM.2022.14.1.2
Published online: June 1, 2022
Department of Internal Medicine, Konyang University College of Medicine, Daejeon, Korea
- Corresponding author: Tae Hee Lee E-mail green740@kyuh.ac.kr ORCID https://orcid.org/0000-0002-8155-7577
• Received: November 18, 2021 • Accepted: December 22, 2021
© The Korean Society of Surgical Metabolism and Nutrition and The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 16,800 Views
- 77 Download
- 1 Crossref
Abstract
- Malnutrition is one of the most common complications in patients with liver cirrhosis. In previous studies, cirrhotic patients with severe malnutrition have been associated with higher morbidity and mortality rates before and after liver transplantation. Frailty and sarcopenia are phenotypes of severe malnutrition that have been associated with complications requiring hospitalization or mortality during the wait for transplantation in patients with cirrhosis. Tools for evaluating frailty include the Activities of Daily Living scale, the Karnofsky Performance Status scale, and the Liver Frailty Index. Diagnosed by using computed tomography, sarcopenia is measured with the skeletal muscle index at L3 and is normalized by height. Nutritional status should be evaluated within the first 24~48 hours of hospitalization in every patient with cirrhosis. Among the various available screening tools, the Royal Free Hospital-Nutritional Prioritizing Tool proposed in the UK is recommended. Nutritional counseling with a multidisciplinary team is recommended to improve long-term survival in patients with cirrhosis. Multidisciplinary nutrition management should include evaluating nutritional status and providing guidance for achieving nutritional goals. Most guidelines suggest a calorie intake of 25~35 kcal/kg/day, and the recommended protein intake is 1.2~1.5 g/kg/day. One beneficial technique for patients is to divide the total recommended intake across four to five daily meals, including a nighttime snack. The principles of nutritional intervention in cirrhotic patients are not different from those in noncirrhotic patients. For improvement of sarcopenia, a strategic approach including physical activity and exercise, hormone replacement therapy, ammonia-lowering agents, and treatment of underlying liver disease is required.
INTRODUCTION
Liver cirrhosis can be accompanied by various complications, with malnutrition being one of the most common. The prevalence of malnutrition in patients with cirrhosis is reported to be 20%, 25%~40%, and 44%~90% in patients with Child-Pugh classifications A, B, and C, respectively. Also, most patients awaiting liver transplantation are malnourished [1]. A number of studies has reported that severe malnutrition is associated with a higher mortality rate in cirrhotic patients, and poor preoperative nutritional status is also known to be associated with higher post-transplant morbidity and mortality following liver transplantation [2]. In addition, malnutrition is related to increased susceptibility and vulnerability to infections and complications, such as hepatic encephalopathy and ascites in patients with cirrhosis [3,4].
Although it is not clear whether malnutrition is reversible in cirrhotic patients, it is indisputable that improvement is needed in dietary intake in cirrhotic patients diagnosed with malnutrition. Above all, frailty and sarcopenia, which are phenotypes of severe malnutrition, have been associated with complications requiring hospitalization in cirrhotic patients or waitlist mortality in patients registered for liver transplant. Frailty and sarcopenia, phenotypes indicating deterioration of muscle function, are associated with various factors, including malnutrition, liver cirrhosis itself, systemic inflammation, decreased physical activity, and environmental factors in cirrhotic patients [5].
As nutritional management in patients with cirrhosis has become more important, the European Society for Clinical Nutrition and Metabolism (ESPEN) and the American Society for Parenteral and Enteral Nutrition (ASPEN), as well as the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD), have presented guidelines and guidance on nutritional management for liver disease patients [5-7]. Based on these guidelines, this study aims to review the methods for evaluating overall nutritional status and sarcopenia in cirrhotic patients, together with nutritional intervention strategies for the patients with liver cirrhosis.
DISCUSSION
Because cirrhotic patients exhibit a high prevalence of malnutrition and frequently show deficiencies in protein and trace elements, evaluation of nutritional status should be conducted within 24~48 hours from patients’ initial visits to physicians. A commonly used method for screening patients for malnutrition is to confirm a low body mass index (BMI) and the presence of progressive decompensated cirrhosis [8,9]. Because cirrhosis causes fluid retention in body tissues, there are some limitations in screening for malnutrition according to BMI. The most highly recommended tool among various screening instruments is the Royal Free Hospital-Nutritional Prioritizing Tool (RFH-NPT), developed in a multicenter trial in the UK (Fig. 1) [10-12]. The RFH-NPT has a scoring system that considers edema and ascites. High RFH-NPT scores are correlated with deterioration of liver function; incidence of complications such as ascites, hepatic encephalopathy, and hepato-renal syndrome; and survival rate [11]. Another proposed screening tool, the six-question Liver Disease Undernutrition Screening Tool, shows a low negative predictive value insofar as it depends on patients’ subjective judgements [13].
1) Assessment of frailty
The prevalence of frailty in patients with liver cirrhosis has been reported to range from 17% to 43% [14]. In cirrhotic patients with hepatic encephalopathy, the prevalence of frailty was reported to be 38% when assessed by the Activities of Daily Living (ADL) scale and 68% when assessed by the Karnofsky Performance Status (KPS) scale [15,16]. In patients with cirrhosis, the presence and worsening of frailty were found to be associated with higher hospitalization rates, re-admission rates, mortality rates and with the lower quality of life [16]. In a study of more than 1,000 patients awaiting liver transplantation at nine medical centers in the United States, high Liver Frailty Index (LFI) scores were associated with a more than two times higher risk of mortality. In addition, an increase in LFI within the preceding three months was independently linked to a more than two-fold increase in the risk of mortality, outside of patients’ evaluation according to the Model for End-Stage Liver Disease score [17].
Several tools to assess frailty have been proposed (Table 1), with these instruments including objective performance-based assessment tools as well as subjective survey-based assessment methods. The ADL and KPS, both of which emphasize practicality, assess patients’ ability to perform various activities of everyday life. The LFI comprises assessment of muscle function (hand grip strength and chair stand tests) and evaluation of balance. The degree of frailty is evaluated based on LFI score (<3.2, robust; 3.2~4.3, prefrail; ≥4.4, frail), and changes in LFI scores during follow-up periods have been reported to be associated with prognosis [17].
Accordingly, while there is some debate among researchers on which frailty assessment tools are optimal, it is widely agreed that patients with liver cirrhosis should be assessed for baseline frailty and changes in frailty during regular follow-up.
2) Assessment of sarcopenia
Of patients with end-stage liver disease, 30%~70% are reported to have sarcopenia [18]. Sarcopenia is more common in men (54%) than in women (21%), and the severity of liver disease has been found to be correlated with the degree of sarcopenia only in men [9]. In previous studies, sarcopenia has been reported to be associated with mortality, liver failure, decreased quality of life, an increase in the occurrence of infections, and increased length of hospital stays [19].
To diagnose sarcopenia, medical imaging techniques such as dual energy X-ray absorptiometry or computed tomography (CT) and/or magnetic resonance imaging (MRI) are used (Table 2) [20]. Sarcopenia is a main clinical feature of malnutrition in cirrhotic patients, and it can be diagnosed when patients have a loss of muscle mass or muscle function. Computed tomography is currently recommended as the gold standard method for evaluating muscle mass in patients with cirrhosis, but it has limitations due to the cost and risks such as radiation exposure [20]. Muscle mass is generally represented with the Skeletal Muscle Index (SMI), which is calculated by normalizing a subject’s total skeletal muscle area measured at L3 by height [21]. The skeletal muscle area at L3 has a linear correlation with whole-body skeletal muscle mass, and when observed on CT, loss of skeletal muscle mass is associated with increased mortality in patients with liver cirrhosis and in those awaiting liver transplantation [22]. In addition, it has been demonstrated that fat-free mass measured by bioelectrical impedance analysis (BIA) is correlated with muscle mass and is also related to mortality in patients with cirrhosis [23]. In cirrhotic patients with ascites, phase angle measurements are helpful because fluid retention affects the reliability of fat-free mass measured by BIA [24].
1) Metabolic status in patients with cirrhosis
Cirrhosis is a state of accelerated starvation, in which the body’s primary metabolic fuel is shifted from glucose to fatty acids, protein synthesis is decreased, gluconeogenesis from protein is increased, and proteolysis is also increased. In these ways, cirrhosis contributes to sarcopenia in patients [25]. The state of accelerated starvation in cirrhotic patients is aggravated by various factors, such as nausea, dyspepsia, decreased appetite due to sodium-restricted diet, decreased intestinal motility due to portal hypertension, and fasting owing to gastrointestinal bleeding [26]. Insulin resistance, which frequently accompanies liver cirrhosis, affects the metabolism of skeletal muscle. Although glucose uptake and non-oxidative glucose processing such as glycogen synthesis in skeletal muscle are decreased, glucose oxidation and lactic acid production are normal in patients with cirrhosis [27]. The use of oxidative fuels induces an increase in the rate of lipid oxidation and insulin resistance during cirrhotic fasting state [28].
2) Energy and protein intake
In general, the energy requirements of patients with compensated cirrhosis are not higher than those of healthy people. In addition, as patients with cirrhosis begin to exhibit a decrease in physical activity, their physical activity-related energy expenditure is reduced. Along these lines, cirrhotic patients tend to spontaneously decrease dietary intake during the natural course of cirrhosis.
Energy supplementation should be carried out in consideration of total energy consumption of subjects in general, and the daily energy expenditure of cirrhotic patients is reported to be 28~37.5 kcal/kg [1]. To accurately measure caloric requirements, the use of an indirect calorimeter can be considered [25]. Most guidelines recommend total energy supplementation of 25~35 kcal/kg/day in cirrhotic patients [5-7]. In the energy expenditures presented herein, weight represents actual body weight adjusted for ascitic fluid and refers to dry weight. However, it is difficult to determine dry weight in actual clinical practice.
Recommended protein intake for patients with cirrhosis is 1.2~1.5 g/kg/day [5-7]. More specifically, 1.2 g/kg/day is recommended for cirrhotic patients without malnutrition, and 1.5 g/kg/day is recommended for those with malnutrition and sarcopenia. When intervening with high-protein supplements, mid-arm muscle circumference, hand grip strength, and serum albumin levels were shown to be improved [28,29]. Even in cirrhotic patients with hepatic encephalopathy, protein intake should not be restricted. A randomized controlled trial reported that protein restriction had no benefits in the clinical course of patients with acute hepatic encephalopathy and can actually increase protein catabolism in patients with hepatic encephalopathy [30].
3) Treatment strategies for sarcopenia
Skeletal muscle is considered an organ that houses protein and maintains protein homeostasis. Skeletal muscle mass varies depending on age, sex, and race, as well as severity of liver disease [31]. Increased ammonia level in skeletal muscle, decreased testosterone and growth hormone, and increased serum and intramuscular myostatin levels, together with endotoxemia and decreased dietary intake also impact sarcopenia (Fig. 2). Although research on molecular mechanisms for treatment of sarcopenia in cirrhosis patients is being conducted, further studies are warranted [32].
Sarcopenia treatment strategies that can be used for cirrhosis patients include increased physical activity and exercise, hormone replacement therapy, lowering of blood ammonia level, and treatment of underlying liver disease [33-36]. Oral nutritional supplements (ONS) and branched-chain amino acids supplements have been reported to be helpful in some patients [37].
4) Trace elements and sodium
Patients with cirrhosis can exhibit deficiencies of water-soluble vitamins (especially thiamine) and fat-soluble vitamins such as vitamin D. There is no validated guideline for systematic evaluation of micronutrient requirements in cirrhotic patients. In addition, administration of micronutrients has been found to have no proven therapeutic effects except for prevention or correction of their specific deficiencies. Zinc and vitamin A supplements can improve taste disorders to indirectly improve food intake and nutritional status by increasing the experience of eating. On the other hand, zinc and selenium deficiencies in patients with alcoholic and nonalcoholic liver disease have been reported [38]. Diagnosis of deficiencies in specific trace elements or vitamins is expensive and can delay initiation of supplementation. Thus, it is recommended to provide supplementation of sufficient amounts of trace elements during the first two weeks of nutritional support in cirrhotic patients in actual clinical practice [39]. However, refeeding syndrome should be considered with caution in cirrhotic patients with malnutrition.
In prescribing a low-sodium diet, the increased risk of any further reduction of food intake should be balanced against the moderate advantages of sodium restriction for treatment of ascites. Indeed, care should be taken not to compromise the palatability of a patient’s diet following sodium reduction [6]. Although low-sodium diets need to be considered in cirrhotic patients with ascites, the benefits of lowering sodium intake can be offset by reductions in energy and protein intake in these patients due to unpalatable dietary restrictions. Accordingly, when prescribing a low-sodium diet, meticulous care must be taken to ensure adequate nutrition intake.
5) Reduction of the fasting state
Eating frequent, small meals is known to help prevent the state of accelerated starvation and proteolysis in cirrhotic patients [40]. Because the interval between meals is longest between evening and morning meals, it is recommended to eat three to five meals a day, including a late evening snack, to improve total body protein status [41]. A retrospective clinical study reports that nocturnal provision of ONS was more effective in improving total body protein status than was daytime supplementation, while a systematic literature review reveals that late evening snacks improve nitrogen balance [41].
6) Multidisciplinary approach
To improve long-term survival in cirrhotic patients, nutritional counseling using a multidisciplinary team is recommended. Multidisciplinary nutritional management should include monitoring of nutritional status and provide guidelines for achieving nutritional goals [42].
Nutritional counseling has the benefit of inducing behavioral changes in patients. Programs should include patient education on the benefits of healthy diets tailored to the medical conditions of the patient. In a single-center retrospective study with a small sample size, specialized nutritional counseling was associated with improved survival in patients with cirrhosis in comparison to patients who did not receive nutritional counseling. It was also found that nutritional counseling using a multidisciplinary team including a physician, nurse, pharmacist, and dietitian is linked to better survival than is counseling by experts in a single profession [42].
The principles of nutritional interventions for cirrhosis patients are not different from those in noncirrhotic patients. If the patient has trouble taking sufficient nutrients orally or it is difficult to supply the target amount even with the provision of ONS, it is necessary to consider enteral nutrition support. In addition, if the patient cannot receive an adequate intake of nutrients orally or via enteral tube feeding or if the patient has fasted for 72 hours or longer, then it is necessary to start intravenous (parenteral) nutrition. Because patients with cirrhosis are susceptible and vulnerable to infections and sepsis, extra care should be taken regarding the management of central venous catheters, and concentrated solutions should be used to prevent fluid overload. In addition, care should be taken against hyperglycemia, and the provision of vitamins and trace elements should be implemented from day one of clinical management. If necessary, nutrition support therapy should be adjusted to prevent refeeding syndrome.
CONCLUSION
In patients with liver cirrhosis, malnutrition is one of the most common complications, and severe malnutrition can be manifested as frailty and sarcopenia. Appropriate assessment of nutritional status should be conducted for all patients with cirrhosis, and when a nutritional intervention is implemented, a multidisciplinary approach has been proven to help to improve survival rates. While sarcopenia is commonly diagnosed with CT, there are limitations in performing CT only for diagnosis of sarcopenia. Accordingly, confirmation of the presence or absence of sarcopenia in all patients with liver disease who undergo CT is required. For patients with liver cirrhosis, adequate intake of calories and protein is essential, and patients benefit more from a program that divides total food intake across several small daily meals, including a late evening snack. To improve sarcopenia, a strategic approach must be involve not only nutrition interventions, but also increased physical activity and exercise, hormone replacement therapy, ammonia-lowering agents, and treatment of underlying liver disease.
AUTHOR CONTRIBUTIONS
Conceptualization: THL. Data curation: HYC. Formal analysis: HYC. Funding acquisition: THL. Investigation: HYC, THL. Methodology: HYC, THL. Project administration: THL. Resources: HYC, THL. Software: HYC. Supervision: THL. Validation: THL. Visualization: HYC, THL. Writing – original draft: HYC. Writing — review and editing: HYC, THL.
CONFLICTS OF INTEREST
The authors of this manuscript have no conflicts of interest to disclose.
FUNDING
None.
Fig. 1
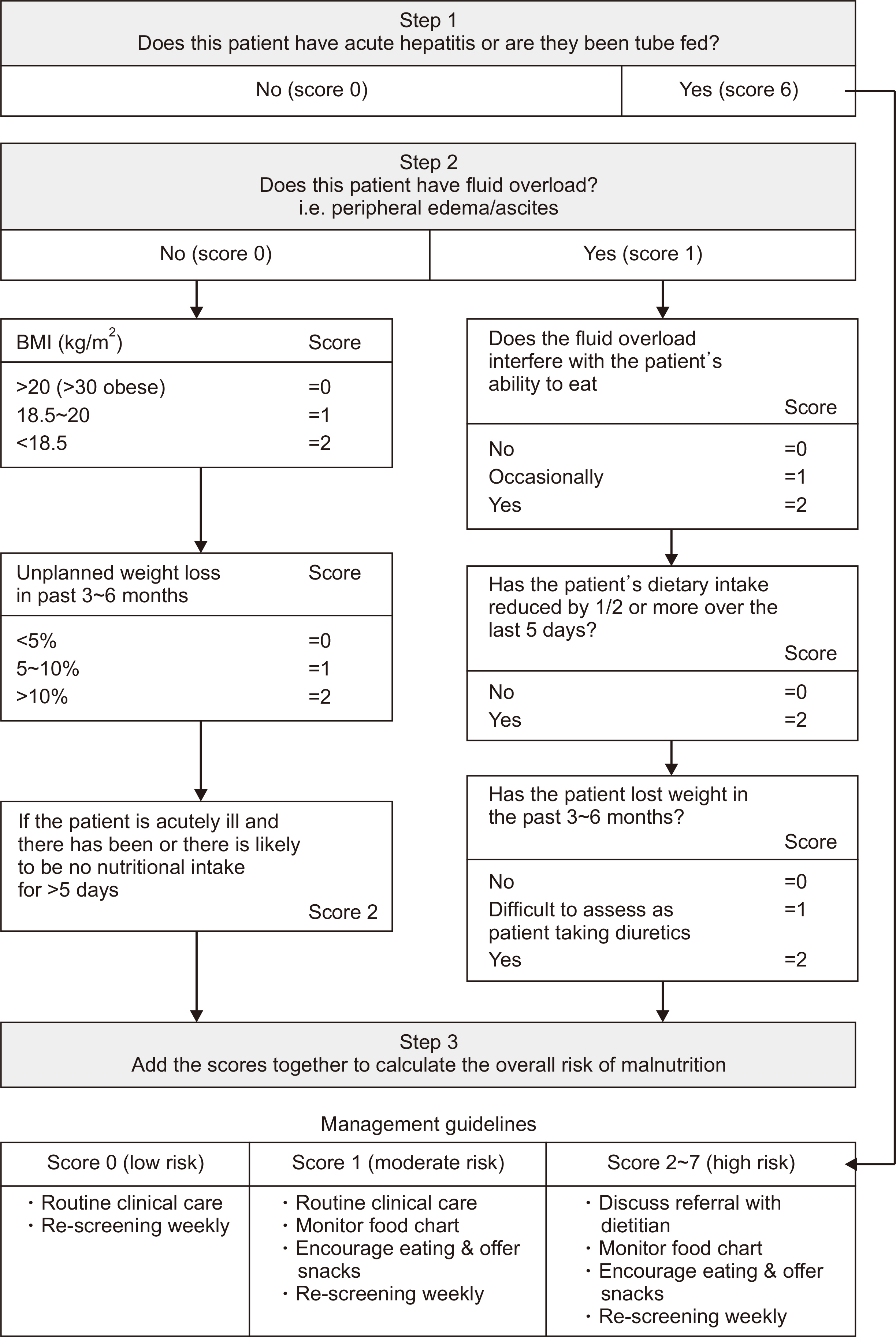
Royal Free Hospital-Nutritional Prioritizing Tool. Revised from an article by Arora et al. (J Hepatol 2012;56(Suppl 2):S241) [12].
BMI = body mass index.
Fig. 2
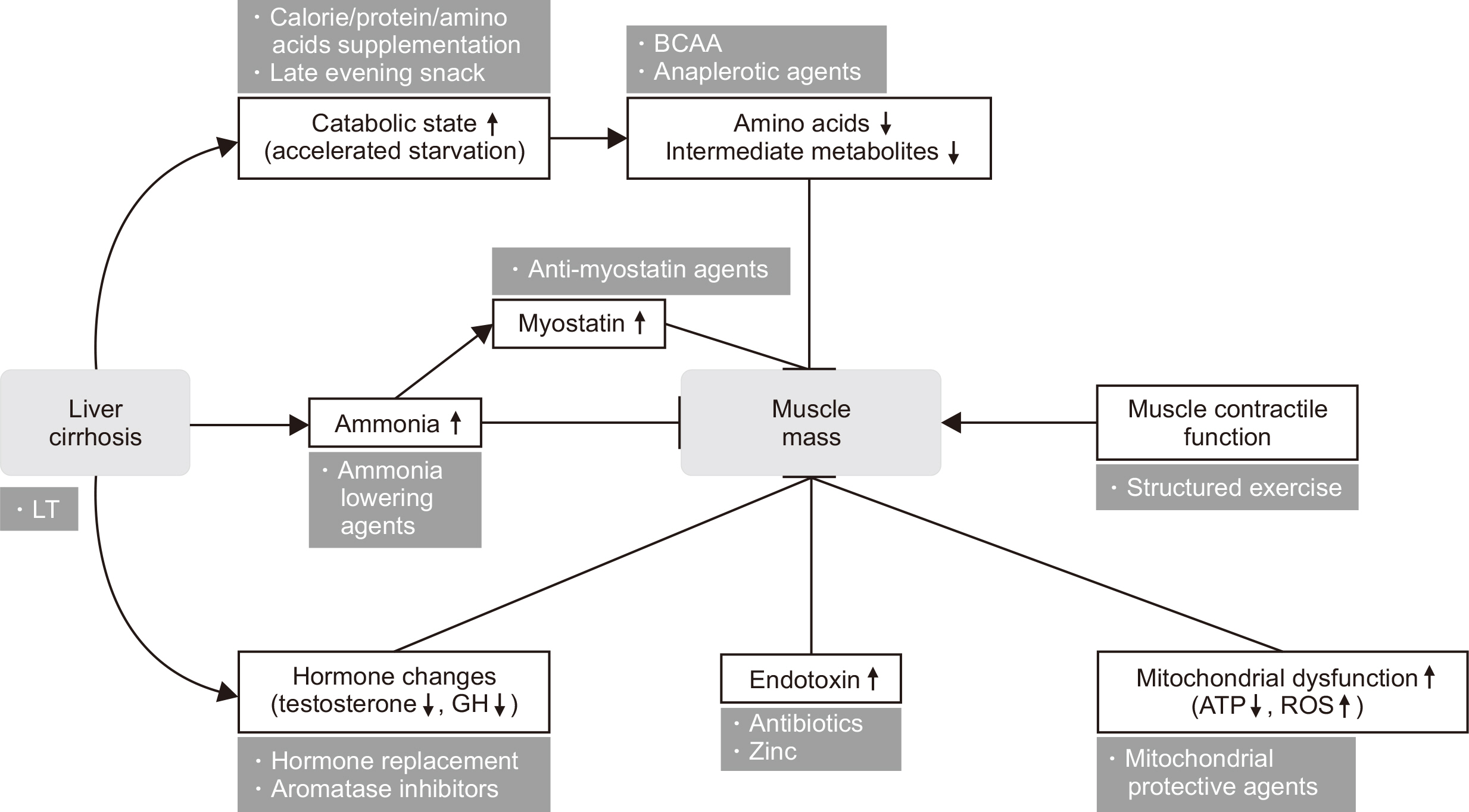
Mechanisms and potential targets for sarcopenia.
ATP = adenosine triphosphate; GH = growth hormone; BCAA = branched chain amino acid; ROS = reactive oxygen species; LT = liver transplantation.
Table 1
Tools to assess frailty
Adapted from an article by Lai et al. (Hepatology 2021;74:1611-44) [5] with original copyright holder’s permission.
ADL = Activities of Daily Living; KPS = Karnofsky Performance Status.
Table 2
Tools to assess sarcopenia
Adapted from an article by Lai et al. (Hepatology 2021;74:1611-44) [5] with original copyright holder’s permission.
BIA = bioelectrical impedance analysis; MRI = magnetic resonance imaging; DEXA = dual energy x-ray absorptiometry; CT = computed tomography.
- 1. Guglielmi FW, Panella C, Buda A, Budillon G, Caregaro L, Clerici C, et al. Nutritional state and energy balance in cirrhotic patients with or without hypermetabolism. Multicentre prospective study by the ‘Nutritional problems in gastroenterology’ Section of the Italian Society of Gastroenterology (SIGE). Dig Liver Dis 2005;37:681-8. ArticlePubMed
- 2. Figueiredo F, Dickson ER, Pasha T, Kasparova P, Therneau T, Malinchoc M, et al. Impact of nutritional status on outcomes after liver transplantation. Transplantation 2000;70:1347-52. ArticlePubMed
- 3. Merli M, Lucidi C, Giannelli V, Giusto M, Riggio O, Falcone M, et al. Cirrhotic patients are at risk for health care-associated bacterial infections. Clin Gastroenterol Hepatol 2010;8:979-85. ArticlePubMed
- 4. Gunsar F, Raimondo ML, Jones S, Terreni N, Wong C, Patch D, et al. Nutritional status and prognosis in cirrhotic patients. Aliment Pharmacol Ther 2006;24:563-72. ArticlePubMed
- 5. Lai JC, Tandon P, Bernal W, Tapper EB, Ekong U, Dasarathy S, et al. Malnutrition, frailty, and sarcopenia in patients with cirrhosis: 2021 practice guidance by the American Association for the study of liver diseases. Hepatology 2021;74:1611-44. ArticlePubMedPMCPDF
- 6. Bischoff SC, Bernal W, Dasarathy S, Merli M, Plank LD, Schütz T, et al. ESPEN practical guideline: clinical nutrition in liver disease. Clin Nutr 2020;39:3533-62. ArticlePubMed
- 7. European Association for the Study of the Liver. EASL clinical practice guidelines on nutrition in chronic liver disease. J Hepatol 2019;70:172-93. ArticlePubMedPMC
- 8. Cederholm T, Bosaeus I, Barazzoni R, Bauer J, Van Gossum A, Klek S, et al. Diagnostic criteria for malnutrition - an ESPEN consensus statement. Clin Nutr 2015;34:335-40. ArticlePubMed
- 9. Tandon P, Ney M, Irwin I, Ma MM, Gramlich L, Bain VG, et al. Severe muscle depletion in patients on the liver transplant wait list: its prevalence and independent prognostic value. Liver Transpl 2012;18:1209-16. ArticlePubMedPDF
- 10. Tandon P, Raman M, Mourtzakis M, Merli M. A practical approach to nutritional screening and assessment in cirrhosis. Hepatology 2017;65:1044-57. ArticlePubMedPDF
- 11. Borhofen SM, Gerner C, Lehmann J, Fimmers R, Görtzen J, Hey B, et al. The royal free hospital-nutritional prioritizing tool is an independent predictor of deterioration of liver function and survival in cirrhosis. Dig Dis Sci 2016;61:1735-43. ArticlePubMedPDF
- 12. Arora S, Mattina C, McAnenny C, O'Sullivan N, McGeeney L, Calder N, et al. The development and validation of a nutritional prioritising tool for use in patients with chronic liver disease. J Hepatol 2012;56(Suppl 2):S241.
- 13. Booi AN, Menendez J, Norton HJ, Anderson WE, Ellis AC. 2015;Validation of a screening tool to identify undernutrition in ambulatory patients with liver cirrhosis. Nutr Clin Pract 30:683-9. ArticlePubMedPDF
- 14. Tandon P, Tangri N, Thomas L, Zenith L, Shaikh T, Carbonneau M, et al. A rapid bedside screen to predict unplanned hospitalization and death in outpatients with cirrhosis: a prospective evaluation of the clinical frailty scale. Am J Gastroenterol 2016;111:1759-67. ArticlePubMedPDF
- 15. Tapper EB, Finkelstein D, Mittleman MA, Piatkowski G, Lai M. Standard assessments of frailty are validated predictors of mortality in hospitalized patients with cirrhosis. Hepatology 2015;62:584-90. ArticlePubMedPMC
- 16. Tandon P, Reddy KR, O'Leary JG, Garcia-Tsao G, Abraldes JG, Wong F, et al. North American Consortium for the Study of End-Stage Liver Disease. A Karnofsky performance status-based score predicts death after hospital discharge in patients with cirrhosis. Hepatology 2017;65:217-24. ArticlePubMedPDF
- 17. Lai JC, Dodge JL, Kappus MR, Dunn MA, Volk ML, Duarte-Rojo A, et al. Multi-Center Functional Assessment in Liver Transplantation (FrAILT) Study. Changes in frailty are associated with waitlist mortality in patients with cirrhosis. J Hepatol 2020;73:575-81. ArticlePubMedPMC
- 18. Mazurak VC, Tandon P, Montano-Loza AJ. Nutrition and the transplant candidate. Liver Transpl 2017;23:1451-64. ArticlePubMedPDF
- 19. Montano-Loza AJ, Meza-Junco J, Prado CM, Lieffers JR, Baracos VE, Bain VG, et al. Muscle wasting is associated with mortality in patients with cirrhosis. Clin Gastroenterol Hepatol 2012;10:166-73. 173.e1. ArticlePubMed
- 20. Carey EJ, Lai JC, Sonnenday C, Tapper EB, Tandon P, Duarte-Rojo A, et al. A North American expert opinion statement on sarcopenia in liver transplantation. Hepatology 2019;70:1816-29. ArticlePubMedPMCPDF
- 21. Carey EJ, Lai JC, Wang CW, Dasarathy S, Lobach I, Montano-Loza AJ, et al. Fitness, Life Enhancement, and Exercise in Liver Transplantation Consortium. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transpl 2017;23:625-33. ArticlePubMedPMCPDF
- 22. Kaido T, Ogawa K, Fujimoto Y, Ogura Y, Hata K, Ito T, et al. Impact of sarcopenia on survival in patients undergoing living donor liver transplantation. Am J Transplant 2013;13:1549-56. ArticlePubMed
- 23. Pirlich M, Schütz T, Spachos T, Ertl S, Weiss ML, Lochs H, et al. Bioelectrical impedance analysis is a useful bedside technique to assess malnutrition in cirrhotic patients with and without ascites. Hepatology 2000;32:1208-15. ArticlePubMed
- 24. Bellafronte NT, Diani LM, Vega-Piris L, Cuadrado GB, Chiarello PG. Comparison between dual-energy x-ray absorptiometry and bioelectrical impedance for body composition measurements in adults with chronic kidney disease: a cross-sectional, longitudinal, multi-treatment analysis. Nutrition 2021;82:111059.ArticlePubMed
- 25. Glass C, Hipskind P, Cole D, Lopez R, Dasarathy S. Handheld calorimeter is a valid instrument to quantify resting energy expenditure in hospitalized cirrhotic patients: a prospective study. Nutr Clin Pract 2012;27:677-88. PubMedPMC
- 26. Juakiem W, Torres DM, Harrison SA. Nutrition in cirrhosis and chronic liver disease. Clin Liver Dis 2014;18:179-90. ArticlePubMed
- 27. Owen OE, Trapp VE, Reichard GA Jr, Mozzoli MA, Moctezuma J, Paul P, et al. Nature and quantity of fuels consumed in patients with alcoholic cirrhosis. J Clin Invest 1983;72:1821-32. ArticlePubMedPMC
- 28. Manguso F, D'Ambra G, Menchise A, Sollazzo R, D'Agostino L. Effects of an appropriate oral diet on the nutritional status of patients with HCV-related liver cirrhosis: a prospective study. Clin Nutr 2005;24:751-9. ArticlePubMed
- 29. Norman K, Kirchner H, Freudenreich M, Ockenga J, Lochs H, Pirlich M. Three month intervention with protein and energy rich supplements improve muscle function and quality of life in malnourished patients with non-neoplastic gastrointestinal disease--a randomized controlled trial. Clin Nutr 2008;27:48-56. ArticlePubMed
- 30. Córdoba J, López-Hellín J, Planas M, Sabín P, Sanpedro F, Castro F, et al. Normal protein diet for episodic hepatic encephalopathy: results of a randomized study. J Hepatol 2004;41:38-43. ArticlePubMed
- 31. Dasarathy J, McCullough AJ, Dasarathy S. Sarcopenia in alcoholic liver disease: clinical and molecular advances. Alcohol Clin Exp Res 2017;41:1419-31. ArticlePubMedPMCPDF
- 32. Dasarathy S. Cause and management of muscle wasting in chronic liver disease. Curr Opin Gastroenterol 2016;32:159-65. ArticlePubMedPMC
- 33. Sinclair M, Grossmann M, Hoermann R, Angus PW, Gow PJ. Testosterone therapy increases muscle mass in men with cirrhosis and low testosterone: a randomised controlled trial. J Hepatol 2016;65:906-13. ArticlePubMed
- 34. Berzigotti A, Albillos A, Villanueva C, Genescá J, Ardevol A, Augustín S, et al. Ciberehd SportDiet Collaborative Group. Effects of an intensive lifestyle intervention program on portal hypertension in patients with cirrhosis and obesity: the SportDiet study. Hepatology 2017;65:1293-305. ArticlePubMedPDF
- 35. Kumar A, Davuluri G, Silva RNE, Engelen MPKJ, Ten Have GAM, Prayson R, et al. Ammonia lowering reverses sarcopenia of cirrhosis by restoring skeletal muscle proteostasis. Hepatology 2017;65:2045-58. ArticlePubMedPMCPDF
- 36. Sinclair M, Gow PJ, Grossmann M, Angus PW. Review article: sarcopenia in cirrhosis--aetiology, implications and potential therapeutic interventions. Aliment Pharmacol Ther 2016;43:765-77. ArticlePubMed
- 37. Nakaya Y, Harada N, Kakui S, Okada K, Takahashi A, Inoi J, et al. Severe catabolic state after prolonged fasting in cirrhotic patients: effect of oral branched-chain amino-acid-enriched nutrient mixture. J Gastroenterol 2002;37:531-6. ArticlePubMedPDF
- 38. Garrett-Laster M, Russell RM, Jacques PF. Impairment of taste and olfaction in patients with cirrhosis: the role of vitamin A. Hum Nutr Clin Nutr 1984;38:203-14. PubMed
- 39. Sriram K, Lonchyna VA. Micronutrient supplementation in adult nutrition therapy: practical considerations. JPEN J Parenter Enteral Nutr 2009;33:548-62. ArticlePubMedPDF
- 40. Tsien CD, McCullough AJ, Dasarathy S. Late evening snack: exploiting a period of anabolic opportunity in cirrhosis. J Gastroenterol Hepatol 2012;27:430-41. ArticlePubMed
- 41. Plank LD, Gane EJ, Peng S, Muthu C, Mathur S, Gillanders L, et al. Nocturnal nutritional supplementation improves total body protein status of patients with liver cirrhosis: a randomized 12-month trial. Hepatology 2008;48:557-66. PubMed
- 42. Iwasa M, Iwata K, Hara N, Hattori A, Ishidome M, Sekoguchi-Fujikawa N, et al. Nutrition therapy using a multidisciplinary team improves survival rates in patients with liver cirrhosis. Nutrition 2013;29:1418-21. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Liver fibrosis index and mortality in metabolic dysfunction–associated steatotic liver disease: a Korean cohort study
Yesung Lee, Woncheol Lee
Scientific Reports.2025;[Epub] CrossRef
 Cite
CiteLiver Cirrhosis and Sarcopenia
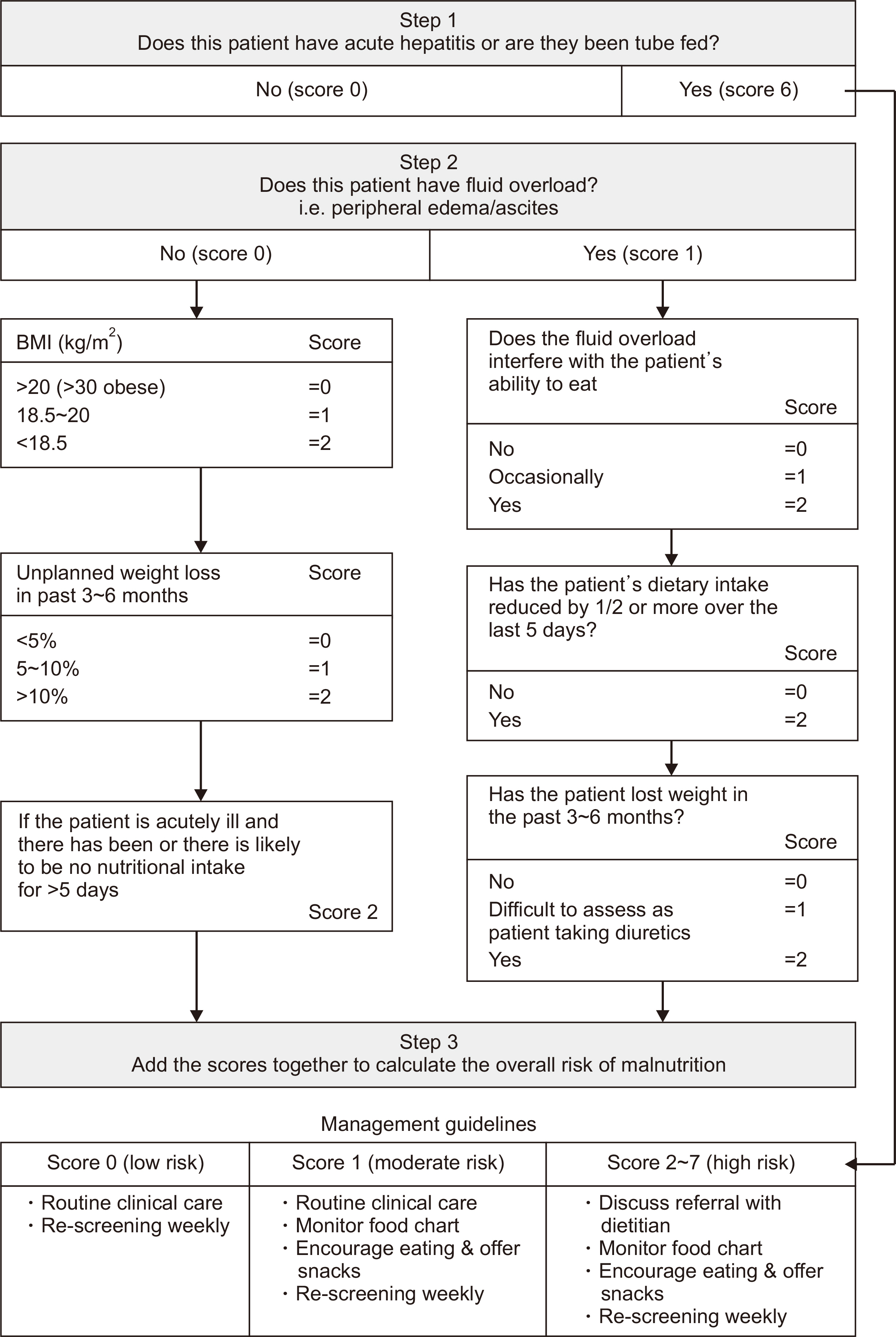
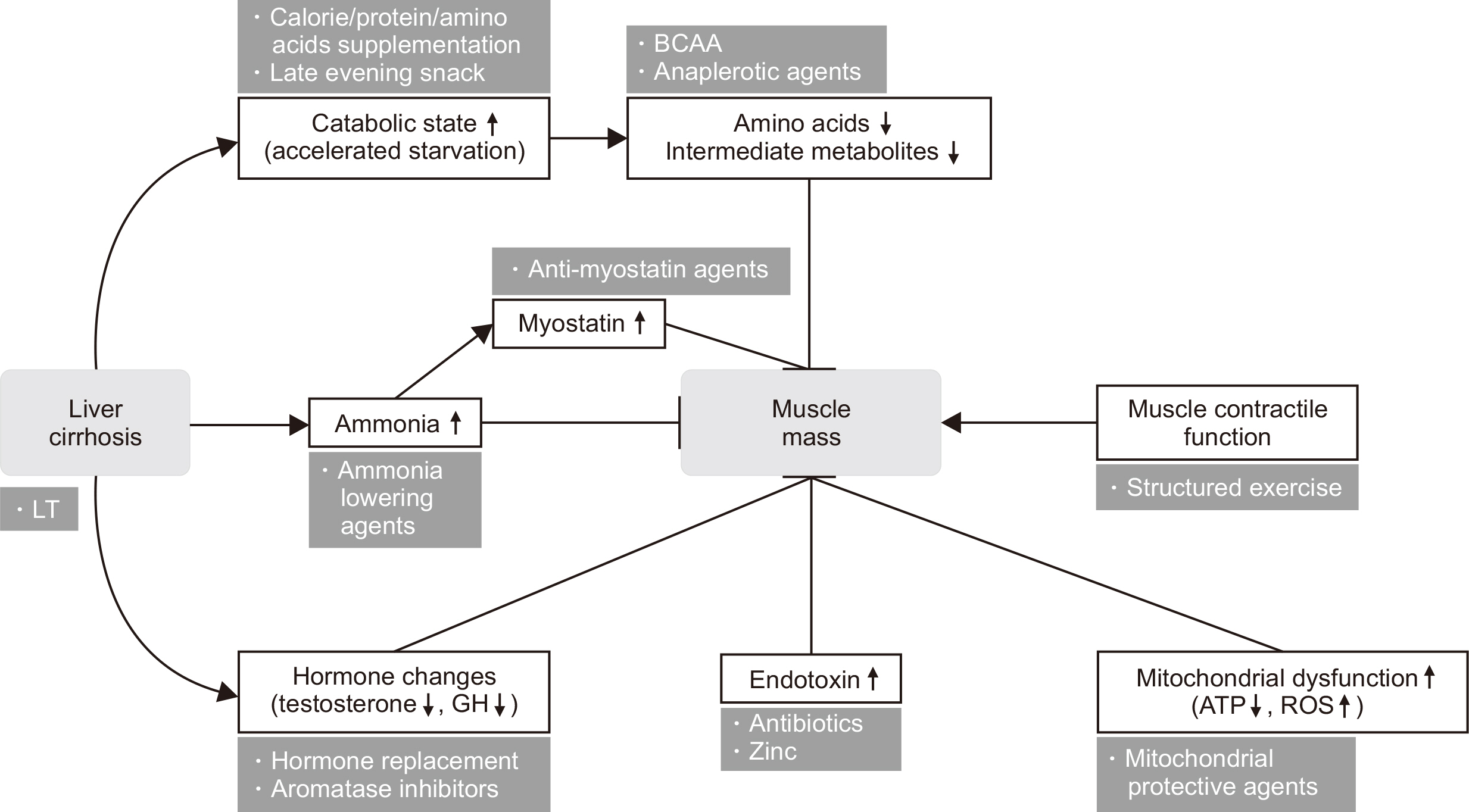
Fig. 1
Royal Free Hospital-Nutritional Prioritizing Tool. Revised from an article by Arora et al. (J Hepatol 2012;56(Suppl 2):S241) [12].
BMI = body mass index.
Fig. 2
Mechanisms and potential targets for sarcopenia.
ATP = adenosine triphosphate; GH = growth hormone; BCAA = branched chain amino acid; ROS = reactive oxygen species; LT = liver transplantation.
Fig. 1
Fig. 2
Liver Cirrhosis and Sarcopenia
Tools to assess frailty
| Tool | Equipment needed | Components | Details |
|---|---|---|---|
| ADL | None | Ability to conduct basic tasks | Patient or caregiver assesses difficulty or dependence with six activities that are essential to daily function (e.g., basic hygiene, eating, ambulation). |
| KPS | None | Ability to carry out normal ADL | Patient, caregiver, or clinician assesses functional limitations ranging from 100 (normal, no complaints, no evidence of disease) to 50 (requires considerable assistance and frequent medical care) to 10 (moribund, fatal processes progressing rapidly). |
| Hand grip strength | Hand dynamometer | Physical frailty | The patient is asked to grip a dynamometer using the dominant hand with their best effort. The test is repeated three times and the values are averaged. |
| 6-minute walk test | Stopwatch, tape measure | Submaximal aerobic capacity and endurance | Test evaluates distance walked on a flat surface at usual walking speed within 6 minutes. |
| Liver Frailty Index | Stopwatch, hand dynamometer, chair | Physical frailty | Cirrhosis-specific tool consisting of grip strength, chair stands, and balance testing. Changes in Liver Frailty Index are associated with outcomes. |
Adapted from an article by Lai et al. (Hepatology 2021;74:1611-44) [
ADL = Activities of Daily Living; KPS = Karnofsky Performance Status.
Tools to assess sarcopenia
| Method | Advantages | Disadvantages | Summary |
|---|---|---|---|
| BIA | Safe, rapid, accessible, minimal-moderate training, repeatable | Strict parameters around nutritional intake and exercise before the test, positioning is challenging in patients with obesity | Fluid retention can impact the reliability of lean body mass estimates. Data using phase angle show good reliability even in patients with fluid retention. |
| MRI | Accurate, no radiation, measures muscle quantity and quality | Costly, limited availablity | Muscle mass is defined by fat-free muscle areas. |
| DEXA | Safe, rapid | Radiation exposure (low), edema can limit accuracy | Low concordance between DEXA and CT in patients with cirrhosis; DEXA appendicular mass improves accuracy in comparison to CT. |
| CT | Accurate, rapid, measures muscle quantity and quality, requires a high level of training to interpret findings | Radiation exposure, not available at bedside, varying cut-points/sites of measurement, not easily repeatable | The majority of evidence supports diagnostic use but includes challenges with radiation exposure and repeatability. |
Adapted from an article by Lai et al. (Hepatology 2021;74:1611-44) [
BIA = bioelectrical impedance analysis; MRI = magnetic resonance imaging; DEXA = dual energy x-ray absorptiometry; CT = computed tomography.
Table 1
Tools to assess frailty
Adapted from an article by Lai et al. (Hepatology 2021;74:1611-44) [ ADL = Activities of Daily Living; KPS = Karnofsky Performance Status.
Table 2
Tools to assess sarcopenia
Adapted from an article by Lai et al. (Hepatology 2021;74:1611-44) [ BIA = bioelectrical impedance analysis; MRI = magnetic resonance imaging; DEXA = dual energy x-ray absorptiometry; CT = computed tomography.

