 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 14(2); 2022 > Article
- Case Report Refeeding Syndrome after Gastrectomy in a Patient with Hypophosphatemia: A Case Report
-
Cheong Ah Oh, M.D.

-
DOI: https://doi.org/10.15747/ACNM.2022.14.2.88
Published online: December 1, 2022
Department of Hospital Medicine, Inha University Hospital, Incheon, Korea
- Corresponding author: Cheong Ah Oh E-mail caoh@inhauh.com ORCID https://orcid.org/0000-0002-1115-5150
• Received: July 15, 2022 • Revised: September 13, 2022 • Accepted: September 13, 2022
© The Korean Society of Surgical Metabolism and Nutrition and The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,898 Views
- 34 Download
Abstract
- This study describes an 81-year-old male who was highly suspicious for refeeding syndrome (RFS) after a retrospective review of his postoperative clinical progression. This highlights the importance of clinicians’ awareness of the possibility of RFS development in surgical patients with any RFS risk factors.
INTRODUCTION
Malnutrition is a well-known risk factor for poor surgical outcomes. It has been reported that the catabolic impact of surgery itself can exacerbate pre-existing malnutrition and metabolic derangement [1]. Inadvertent nutritional treatment can cause a potentially fatal clinical condition, such as refeeding syndrome (RFS), in malnourished or metabolically stressed patients [2]. RFS is an exaggerated metabolic response to resumption of nutrition in malnourished patients and is characterized by electrolyte disturbances, vitamin deficiencies, and fluid overload, which can lead to many organ dysfunctions [2,3]. Despite long-standing recognition as a serious clinical complication with a high mortality rate, RFS has been frequently overlooked, underdiagnosed and often inappropriately treated even if recognized [2,4]. Accurate and early identification of surgical patients who are at risk for RFS may allow optimization of preoperative nutrition and prevention of RFS [3].
In the present study, we report the case of an 81-year-old male gastric cancer patient who rapidly deteriorated and died from cardiopulmonary abnormalities during the postoperative period after gastrectomy. A retrospective chart review revealed that he was classified as high risk for RFS according to the National Institute for Health and Clinical Excellence (NICE) criteria [5]. Because the possibility of RFS occurrence had not been considered in an earlier examination, appropriate preventative measures were not applied. The present case raises the awareness of the possibility of RFS occurrence in malnourished surgical patients.
CASE REPORT
This case study was conducted according to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Inha University Hospital (2022-05-018). In August 2018, an 81-year-old male was admitted for gastrectomy after identification of a 3 cm-sized Borrmann type III advanced gastric cancer on a periodic check-up for lung cancer. He had undergone right upper lung lobectomy and right lower lung wedge resection for a large-cell neuroendocrine lung tumor in May 2006 and then received adjuvant chemotherapy. He underwent laparoscopic left adrenalectomy for isolated metastasis from lung cancer in May 2017. Anamnesis revealed hypertension, history of pulmonary tuberculosis, chronic obstructive pulmonary disease, atrial fibrillation, pulmonary embolism, and peripheral artery occlusive disease in both lower extremities. The patient was on medication for hypertension and had been prescribed a platelet agglutination inhibitor.
On admission, he weighed 50.9 kg and was 164.4 cm tall; his body mass index (BMI) was 18.83 kg/m2. His malnutrition status was evaluated using the Malnutrition Universal Screening Tool on the day of admission, showing a medium risk of undernutrition (score 1 because of BMI between 18.5 and 20.0 kg/m2) [6,7]. According to the Nutritional Risk Screening 2002 system, he was nutritionally at risk, with an age-adjusted total score of 3 after obtaining score 2 for major abdominal surgery on the severity of disease [7,8]. He underwent subtotal gastrectomy with Billroth-I reconstruction. Curative resection with D2 lymph node dissection was performed without intraoperative complications.
The patient was nulla per os until postoperative day (POD) 4. On POD 1, he received 1,450 mL Winuf®peri (JW Pharmaceutical, Seoul, Korea) with Hartmann’s solution. Oliguria (<0.5 mL/kg/hour) occurred on POD 1 and did not improve despite fluid resuscitation. Winuf®peri was replaced by 1,440 mL of 5% dextrose fluid in an attempt to improve oliguria by administration of a high dose of crystalloid on POD 2. He received 1,440 mL of 5% dextrose fluid with Hartmann’s solution until he began taking sips of water on POD 5. On POD 6, he started a semi-fluid diet with oral supplemental drinks. On POD 7, the patient was reluctant to continue oral intake due to general weakness and loss of appetite. At 10 a.m., he developed sudden dyspnea and had a blood pressure of 132/70 mmHg, a pulse rate of 130 beats/minute, a body temperature of 36.9°C, and an percutaneous oxygen saturation of 85%. On physical examination, the patient exhibited crackle lung sounds in both lung fields and no abnormal findings in the abdomen. Posteroanterior chest X-ray revealed bilateral pleural effusions, and electrocardiography showed atrial fibrillation with a rapid ventricular response. Pulmonary embolism computed tomography was carried out to discern the cause of his sudden respiratory distress and revealed pulmonary edema combined with pneumonia. The patient had been treated with empirical antibiotics for hospital-acquired pneumonia (HAP) since POD 2 (Fig.1). Because his respiratory distress increased over time, endotracheal intubation was performed on POD 10. He eventually died of multiple organ failure resulting from aggravated pneumonia on POD 53. Tables 1, 2 summarize the laboratory test results and notable clinical aspects according to net energy intake during the postoperative period.
According to the European Society for Clinical Nutrition and Metabolism [9], the postoperative energy and protein requirements of this patient were 1,272.5~1,527.0 kcal/day (25~30 kcal/kg/day) and 76.3 g/day (1.5 g/kg/day), respectively, based on a body weight of 50.9 kg. Energy intake from 1,450 mL Winuf®peri (103 g glucose, 45.7 g amino acids, 40.8 g fat) on POD 1 was 1,004 kcal (78% of the recommended 25 kcal/kg/day). From POD 2 to POD 5, the source of the patient’s main energy intake was 1,440 mL of 5% dextrose fluid (72 g glucose), providing 244.8 kcal, which covered only 19% of the recommended postoperative energy intake. With resumption of an oral dietary intake on POD 6, the patient was supplied with a total of 575 kcal of a semi-fluid diet with supplemental oral drinks, which provided only 45% of the recommended energy intake. However, most of the total calories were supplied only for breakfast and lunch. On the next day (POD 7), his pneumonia deteriorated accompanying with symptoms of sudden respiratory distress.
Postmortem assessment showed hypophosphatemia from the time of hospitalization through the postoperative period (Fig 2). Intravenous phosphate supplementation (phosphate 20 mmol as KH2PO4 20 mL) was administered at a level of phosphate 1.5 mg/dL on POD 4, but the concentration (2.0 mg/dL) measured at the time of reinstitution of oral intake on POD 5 was below the normal range. Through a retrospective chart review, he was later classified as high risk for RFS due to hypophosphatemia before refeeding according to the NICE criteria [5].
CONCLUSION
RFS is manifested by an imbalance of electrolytes (particularly phosphate, potassium, and magnesium), vitamin depletion (e.g., vitamin B1 thiamine deficiency), fluid imbalances, and organ dysfunctions, which are associated with mortality and other adverse clinical outcomes [2,3,10]. Hypophosphatemia is the most common symptom of RFS and can lead to several clinical manifestations, such as rhabdomyolysis, hemolysis, respiratory failure, and musculoskeletal disorders [2,10]. Therefore, phosphate supplementation should be administered preventively to patients at very high risk for RFS even in the case of low-normal serum level to prevent RFS [3]. The expert consensus of Friedli et al. recommends that clinicians assess all patients’ individual risk for RFS before beginning nutritional therapy and adapt the nutritional care plan accordingly [2,11,12]. The rates of fluid and nutrition administration, correction of electrolyte imbalances, and supplementation of vitamins and micronutrients should be determined based on RFS risk [3,13]. Owing to the risk of fluid overload, sodium, and hydration should be provided cautiously until the patient is metabolically stable [2,3].
Our patient might have suffered from excessive hyper-catabolism due to the stress of major surgery and postoperative pneumonia in addition to his pre-existing malnourished status, and therefore he might have depleted intracellular micronutrient stores [2]. After reviewing his postoperative nutritional assessment, it was obvious that he had not been nourished properly to overcome the excessive catabolic state caused by major surgical stress and infectious diseases (like HAP). We failed to recognize his high risk of RFS as an oncological and geriatric patient, and we failed to properly plan his nutritional treatment preoperatively and postoperatively. Priorly, we should have tried to correct electrolyte imbalances more timely and adequately with supplementation of thiamine before initiation of feeding [2,3,10]. During his stay, no other laboratory tests that would have helped to diagnose RFS were performed; his magnesium and thiamine levels were not measured. The proper phosphate concentration correction was neglected, and there was no consideration for supplementation of thiamine. After the reintroduction of feeding without proper prophylactic treatment in a patient at risk for RFS who had experienced a period of undernutrition, exacerbated hypophosphatemia (20% reduction) and clinical manifestations (such as aggravated respiratory distress and edema) led to suspicion of RFS only after a chart review. The limitation of this case is as follows. Although he might have had RFS, the main cause of mortality might not have been RFS. Before the diet was administered, the patient had already demonstrated several problems caused by existing co-morbidities that could have led to his adverse clinical outcomes. However, it is regrettable that the patient’s prognosis might have been changed if the medical staff had quickly recognized and addressed RFS.
Awareness of the risk of RFS in malnourished surgical patients must be increased since RFS is a highly challenging metabolic situation [2] that may lead to potentially serious outcomes and post-surgical complications. Clinical suspicion, close monitoring, and early treatment of patients at risk will help prevent RFS.
CONFLICTS OF INTEREST
The author of this manuscript has no conflicts of interest to disclose.
FUNDING
None.
Fig. 1
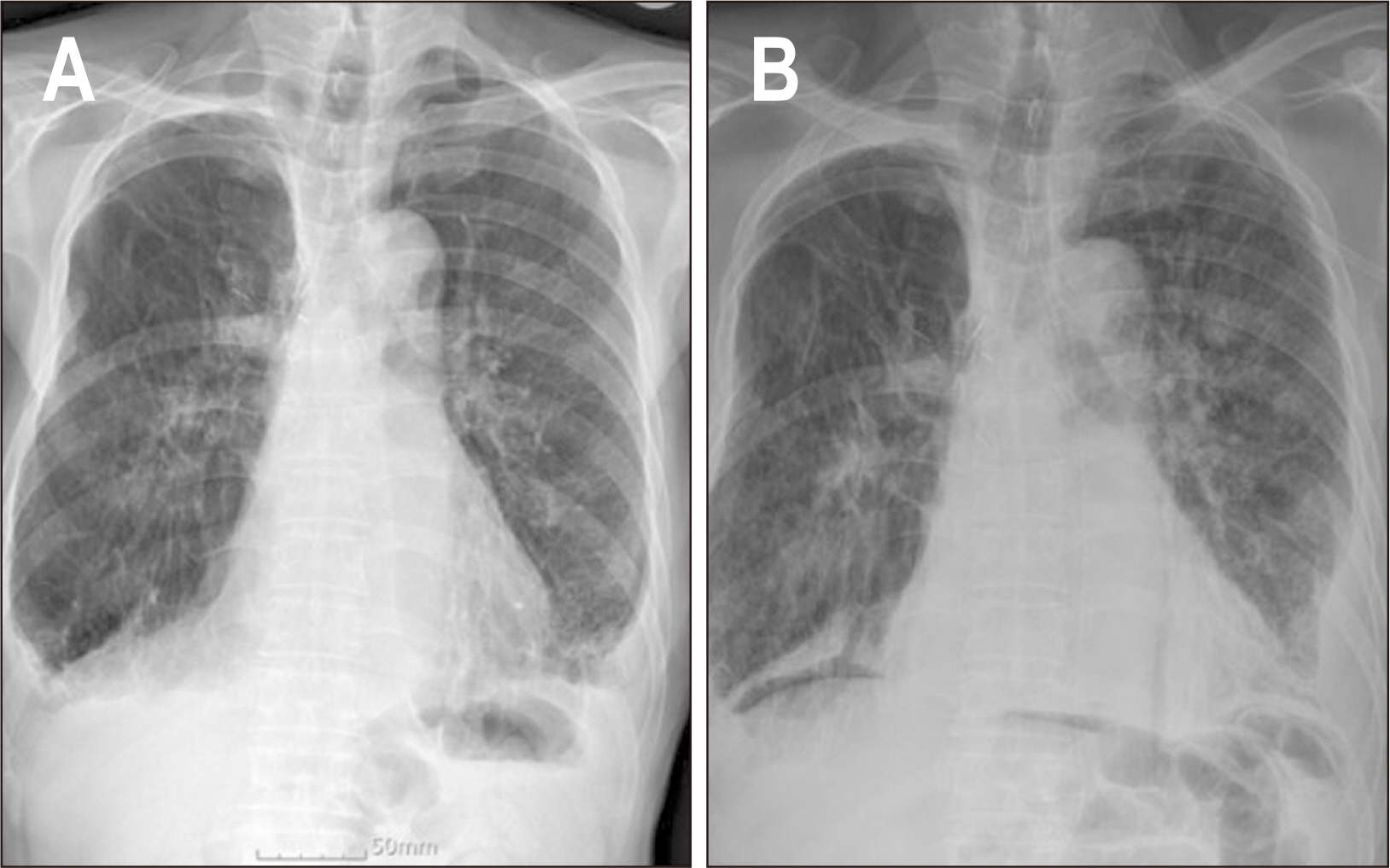
Chest X-ray radiographs (posteroanterior view) on admission (A) and on postoperative day 2 (B).
Fig. 2
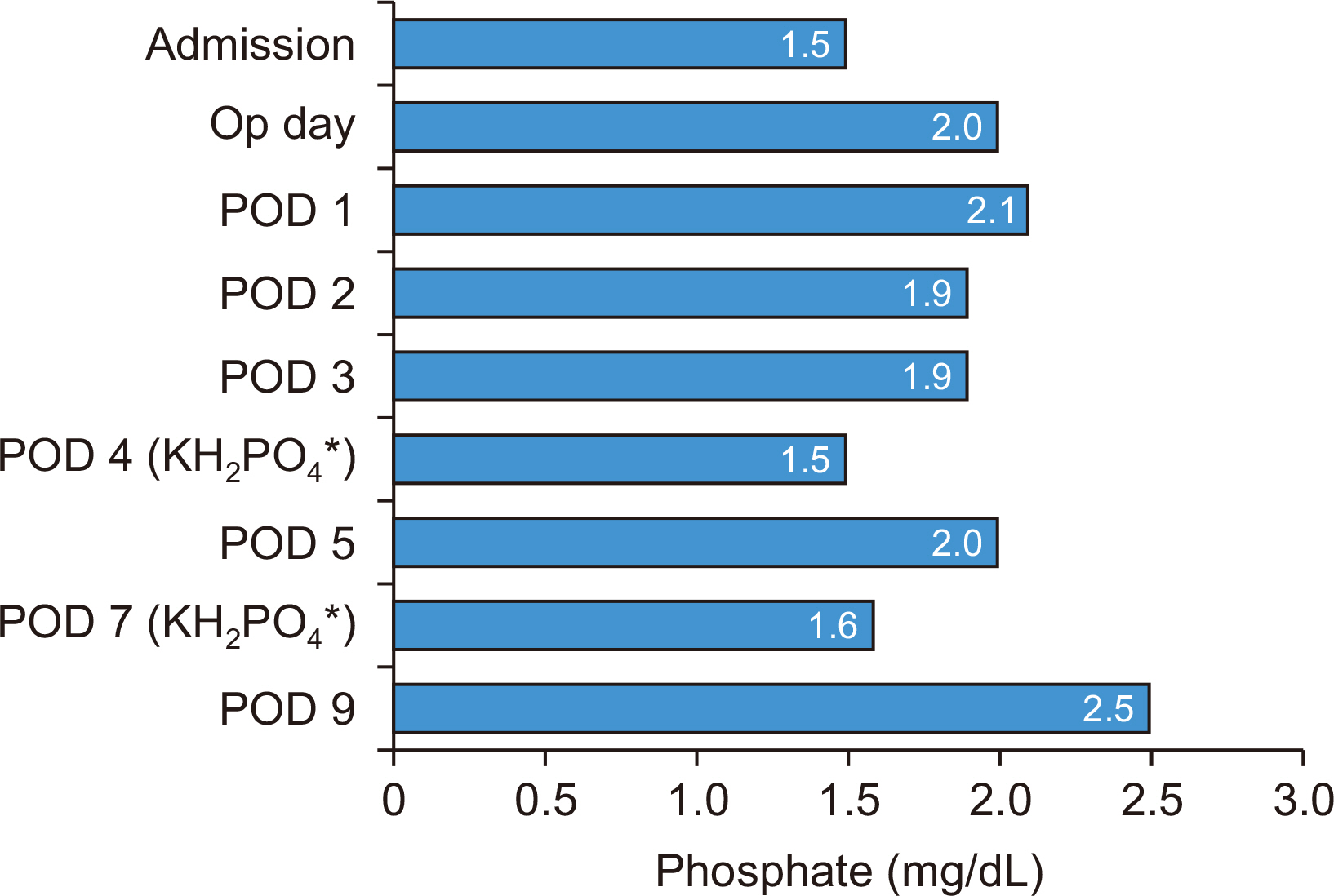
Preoperative and postoperative phosphate level.
*Phosphate supplementation as KH2PO4 was given on POD 4 and POD 7.
Op = operation; POD = postoperative day.
Table 1
Laboratory test results and remarkable clinical characteristics according to net energy intake before resumption of oral intake
| Admission | Op day | POD 1 | POD 2 | POD 3 | POD 4 | |
|---|---|---|---|---|---|---|
| Infused caloric fluid | 5% DNK1 1,440 mL | 5% DNK1 1,440 mL | Winuf®peria 1,450 mL | 5% DNK1 1,440 mL | 5% DNK1 1,440 mL | 5% DNK1 1,440 mL |
| Total calorie (kcal) | 244.8 | 244.8 | 1,004 | 244.8 | 244.8 | 244.8 |
|
|
||||||
| Biochemical parameters (reference range) | ||||||
| White blood cell count (/μL) (4,000~10,000) | 3,960 | 9,110 | 14,830 | 16,470 | 14,250 | 8,960 |
| Hemoglobin (g/dL) (13.1~17.5) | 10.6 | 10.0 | 10.9 | 9.9 | 9.2 | 8.4 |
| Hematocrit (%) (39.0~52.0) | 35.2 | 31.8 | 35.9 | 31.3 | 28.9 | 26.2 |
| Platelet count (×1,000/μL) (140~400) | 166 | 146 | 127 | 90 | 62 | 56 |
| Na (mEq/l) (133~145) | NP | 138 | 135 | 136 | 134 | 133 |
| K (mEq/l) (3.5~5.5) | NP | 4.26 | 4.80 | 4.9 | 4.3 | 3.7 |
| Cl (mEq/l) (95~110) | NP | 105 | 103 | 107 | 104 | 102 |
| Calcium (mg/dL) (8.6~10.7) | 8.5 | 7.8 | 8.7 | 10.1 | 9.1 | 8.4 |
| Phosphate (mg/dL) (2.5~4.5) | 1.5 | 2.0 | 2.1 | 1.9 | 1.9 | 1.5 |
| Glucose (mg/dL) (70~100) | 89 | 114 | 157 | 98 | 124 | 114 |
| Albumin (mg/dL) (3.5~5.2) | 3.6 | 2.7 | 2.8 | 3.2 | 2.6 | 2.6 |
| BUN (mg/dL) (6~20) | 11.5 | 9.4 | 11.7 | 25.9 | 27.0 | 20.8 |
| Creatinine (mg/dL) (0.5~1.2) | 0.97 | 1.02 | 1.09 | 1.07 | 1.29 | 1.08 |
|
|
||||||
| Intake/output (mL/mL) | NP | 1,950/820 | 5,100/1,060 | 4,400/2,615 | 3,150/2,900 | 3,000/2,685 |
| Intraperitoneal drainage amount (mL) | 310 | 320 | 530 | 900 | 585 | |
|
|
||||||
| Injections | Hartmann’s solution Calcium gluconate 10% 40 mL 20% albumin 100 mL Volulyte®b 6% 500 mL | Hartmann’s solution Tamipool®c 1 ampoule Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g | Hartmann’s solution 20% albumin 100 mL Levofloxacin 750 mg Piperacillin/tazobactam 4.5 g | Hartmann’s solution KH2PO4 20 mL 20% albumin 100 mL Levofloxacin 750 mg Piperacillin/tazobactam 4.5 g | ||
|
|
||||||
| Body weight (kg) | 50.9 | 51.2 | 53.8 | 56.1 | 58.8 | 59.0 |
| Notable clinical features | HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | |||
Table 2
Laboratory test results and notable clinical features according to net energy intake after initiating oral intake
| POD 5 | POD 6 | POD 7 | POD 9 | |
|---|---|---|---|---|
| Infused caloric fluid | 5% DNK1 1,440 mL | Nutriflex®peri 40a | ||
| Oral intake | SOW |
SFD Breakfast: whole meal (300 kcal) Lunch: 2/3 meal (200 kcal) Dinner: 1/4 meal (75 kcal) |
SBD (minimal) | None (intubation status) |
| Total calories (kcal) | 244.8 | 575 | <200 | 480 |
|
|
||||
| Biochemical parameters (reference range) | ||||
| White blood cell count (/μL) (4,000~1,000) | 7,480 | NP | 6,630 | 17,670 |
| Hemoglobin (g/dL) (13.1~17.5) | 9.4 | NP | 9.2 | 11.6 |
| Hematocrit (%) (39.0~52.0) | 29.2 | NP | 28.6 | 36.6 |
| Platelet count (×1,000/μL) (140~400) | 67 | NP | 94 | 142 |
| Na (mEq/l) (133~145) | 134 | NP | 132 | 135 |
| K (mEq/l) (3.5~5.5) | 3.6 | NP | 3.5 | 2.68 |
| Cl (mEq/l) (95~110) | 99 | NP | 95 | 95 |
| Calcium (mg/dL) (8.6~10.7) | 8.6 | NP | 8.0 | 8.3 |
| Phosphate (mg/dL) (2.5~4.5) | 2.0 | NP | 1.6 | 2.5 |
| Glucose (mg/dL) (70~100) | 92 | NP | 83 | 91 |
| Albumin (mg/dL) (3.5~5.2) | 3.1 | NP | 2.7 | 2.8 |
| BUN (mg/dL) (6~20) | 18.7 | NP | 13.7 | 23.5 |
| Creatinine (mg/dL) (0.5~1.2) | 1.06 | NP | 1.00 | 1.17 |
|
|
||||
| Intake/output (mL/mL) | 3,000/2,920 | 2,935/3,450 | 2,935/3,450 | 1,440/1,340 |
| Intraperitoneal drainage amount (mL) | 920 | 390 | 1,220 | 160 |
|
|
||||
| Injections | Hartmann’s solution Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g | Hartmann’s solution Tamipool®b 1 ampoule 20% albumin 100 mL Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g Furosemide 30 mg | Hartmann’s solution KH2PO4 20 mL Tamipool®b 1 ampoule 20% albumin 100 mL Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g Furosemide 20 mg | Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g |
|
|
||||
| Body weight (kg) | 50.9 | 51.2 | 53.8 | 56.1 |
| Notable clinical features | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion |
- 1. Lakananurak N, Gramlich L. The role of preoperative parenteral nutrition. Nutrients 2020;12:1320.ArticlePubMedPMC
- 2. Reber E, Friedli N, Vasiloglou MF, Schuetz P, Stanga Z. Management of refeeding syndrome in medical inpatients. J Clin Med 2019;8:2202.ArticlePubMedPMC
- 3. Ponzo V, Pellegrini M, Cioffi I, Scaglione L, Bo S. The refeeding syndrome: a neglected but potentially serious condition for inpatients. A narrative review. Intern Emerg Med 2021;16:49-60. ArticlePubMedPMCPDF
- 4. Buitendag J, Variawa S, Davids R, Ahmed N. Refeeding syndrome in surgical patients post initiation of artificial feeding, a prospective cohort study in a low-income country. Clin Nutr ESPEN 2021;46:210-5. ArticlePubMed
- 5. National Institute for Health and Care Excellence. 2006. London: United Kingdom: Available from: https://www.nice.org.uk/guidance/cg32/chapter/Recommendations#screening-for-malnutrition-and-the-risk-of-malnutrition-in-hospital-and-the-community. [cited 2022 May 24
- 6. Stratton RJ, Hackston A, Longmore D, Dixon R, Price S, Stroud M, et al. Malnutrition in hospital outpatients and inpatients: prevalence, concurrent validity and ease of use of the 'malnutrition universal screening tool' ('MUST') for adults. Br J Nutr 2004;92:799-808. ArticlePubMed
- 7. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M. Educational and Clinical Practice Committee, European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002. Clin Nutr 2003;22:415-21. ArticlePubMed
- 8. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z. Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr 2003;22:321-36. ArticlePubMed
- 9. Weimann A, Braga M, Carli F, Higashiguchi T, Hübner M, Klek S, et al. ESPEN guideline: clinical nutrition in surgery. Clin Nutr 2017;36:623-50. ArticlePubMed
- 10. Kim JW. Refeeding syndrome. J Clin Nutr 2015;7:15-22. Article
- 11. Friedli N, Stanga Z, Culkin A, Crook M, Laviano A, Sobotka L, et al. Management and prevention of refeeding syndrome in medical inpatients: an evidence-based and consensus-supported algorithm. Nutrition 2018;47:13-20. ArticlePubMed
- 12. Friedli N, Stanga Z, Sobotka L, Culkin A, Kondrup J, Laviano A, et al. Revisiting the refeeding syndrome: results of a systematic review. Nutrition 2017;35:151-60. ArticlePubMed
- 13. McKnight CL, Newberry C, Sarav M, Martindale R, Hurt R, Daley B. Refeeding syndrome in the critically ill: a literature review and clinician's guide. Curr Gastroenterol Rep 2019;21:58.ArticlePubMedPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteRefeeding Syndrome after Gastrectomy in a Patient with Hypophosphatemia: A Case Report
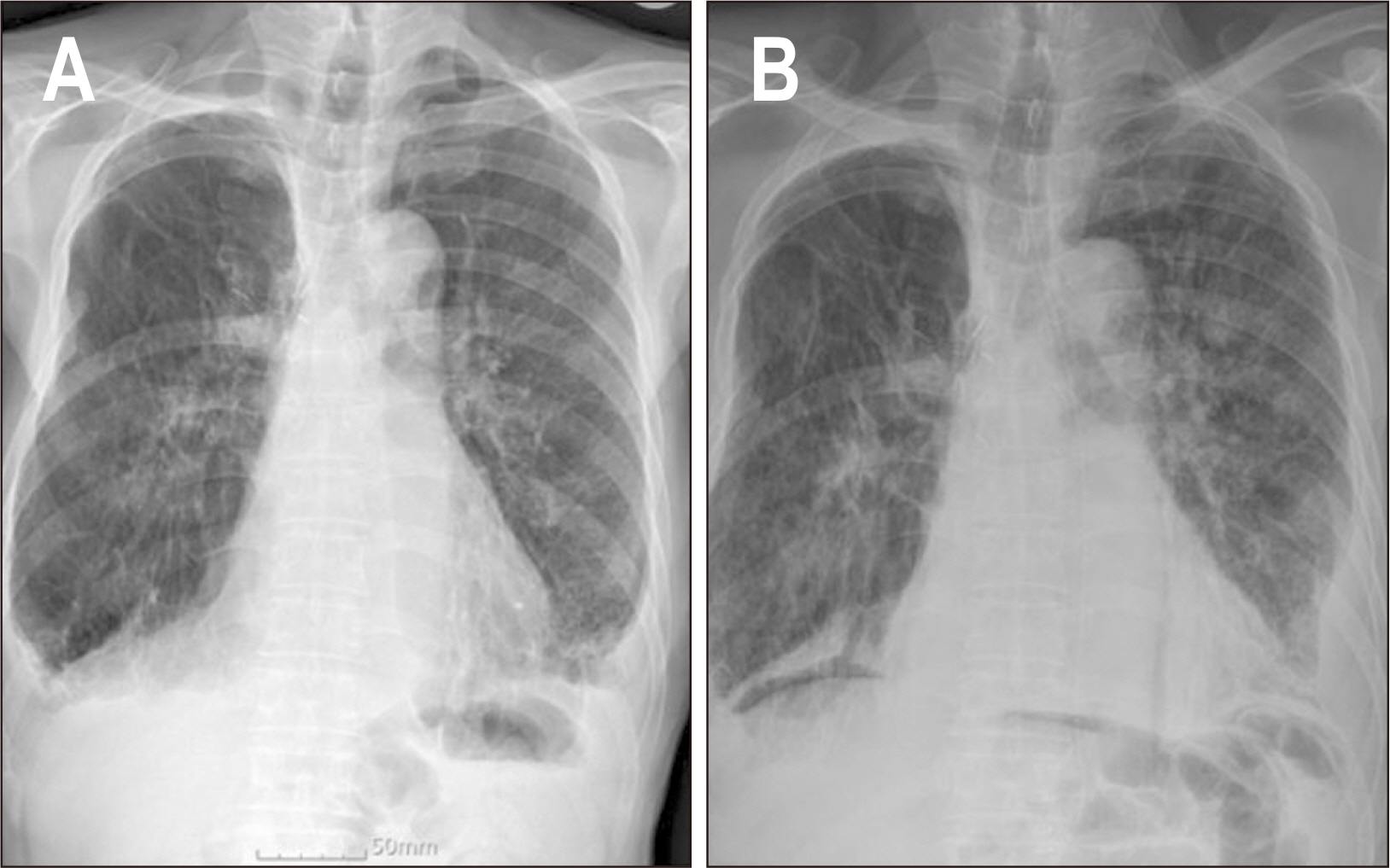
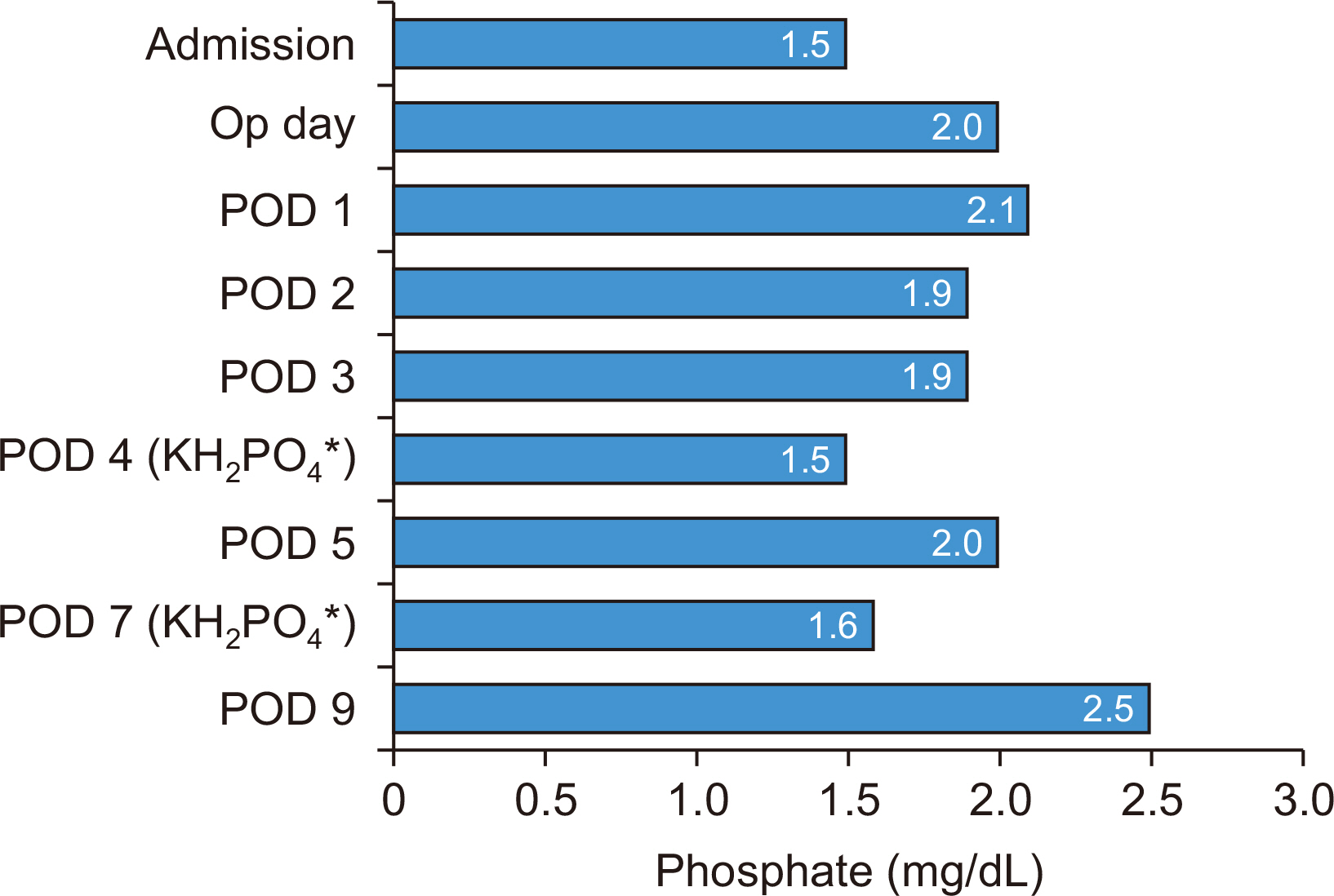
Fig. 1
Chest X-ray radiographs (posteroanterior view) on admission (A) and on postoperative day 2 (B).
Fig. 2
Preoperative and postoperative phosphate level.
*Phosphate supplementation as KH2PO4 was given on POD 4 and POD 7.
Op = operation; POD = postoperative day.
Fig. 1
Fig. 2
Refeeding Syndrome after Gastrectomy in a Patient with Hypophosphatemia: A Case Report
Laboratory test results and remarkable clinical characteristics according to net energy intake before resumption of oral intake
| Admission | Op day | POD 1 | POD 2 | POD 3 | POD 4 | |
|---|---|---|---|---|---|---|
| Infused caloric fluid | 5% DNK1 1,440 mL | 5% DNK1 1,440 mL | Winuf®peri |
5% DNK1 1,440 mL | 5% DNK1 1,440 mL | 5% DNK1 1,440 mL |
| Total calorie (kcal) | 244.8 | 244.8 | 1,004 | 244.8 | 244.8 | 244.8 |
| Biochemical parameters (reference range) | ||||||
| White blood cell count (/μL) (4,000~10,000) | 3,960 | 9,110 | 14,830 | 16,470 | 14,250 | 8,960 |
| Hemoglobin (g/dL) (13.1~17.5) | 10.6 | 10.0 | 10.9 | 9.9 | 9.2 | 8.4 |
| Hematocrit (%) (39.0~52.0) | 35.2 | 31.8 | 35.9 | 31.3 | 28.9 | 26.2 |
| Platelet count (×1,000/μL) (140~400) | 166 | 146 | 127 | 90 | 62 | 56 |
| Na (mEq/l) (133~145) | NP | 138 | 135 | 136 | 134 | 133 |
| K (mEq/l) (3.5~5.5) | NP | 4.26 | 4.80 | 4.9 | 4.3 | 3.7 |
| Cl (mEq/l) (95~110) | NP | 105 | 103 | 107 | 104 | 102 |
| Calcium (mg/dL) (8.6~10.7) | 8.5 | 7.8 | 8.7 | 10.1 | 9.1 | 8.4 |
| Phosphate (mg/dL) (2.5~4.5) | 1.5 | 2.0 | 2.1 | 1.9 | 1.9 | 1.5 |
| Glucose (mg/dL) (70~100) | 89 | 114 | 157 | 98 | 124 | 114 |
| Albumin (mg/dL) (3.5~5.2) | 3.6 | 2.7 | 2.8 | 3.2 | 2.6 | 2.6 |
| BUN (mg/dL) (6~20) | 11.5 | 9.4 | 11.7 | 25.9 | 27.0 | 20.8 |
| Creatinine (mg/dL) (0.5~1.2) | 0.97 | 1.02 | 1.09 | 1.07 | 1.29 | 1.08 |
| Intake/output (mL/mL) | NP | 1,950/820 | 5,100/1,060 | 4,400/2,615 | 3,150/2,900 | 3,000/2,685 |
| Intraperitoneal drainage amount (mL) | 310 | 320 | 530 | 900 | 585 | |
| Injections | Hartmann’s solution Calcium gluconate 10% 40 mL 20% albumin 100 mL Volulyte® |
Hartmann’s solution Tamipool® |
Hartmann’s solution 20% albumin 100 mL Levofloxacin 750 mg Piperacillin/tazobactam 4.5 g | Hartmann’s solution KH2PO4 20 mL 20% albumin 100 mL Levofloxacin 750 mg Piperacillin/tazobactam 4.5 g | ||
| Body weight (kg) | 50.9 | 51.2 | 53.8 | 56.1 | 58.8 | 59.0 |
| Notable clinical features | HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | |||
Op = operation; POD = postoperative day; 5% DNK1 = dextrose 5% (187 kcal/bag); NP = not performed; HAP = hospital-acquired pneumonia.
aWinuf®peri (JW Pharmaceutical, Seoul, Korea); bVolulyte® (Fresenius Kabi Deutschland GmbH, Friedberg, Germany); cTamipool® (BCWP, Yeoju, Korea).
Laboratory test results and notable clinical features according to net energy intake after initiating oral intake
| POD 5 | POD 6 | POD 7 | POD 9 | |
|---|---|---|---|---|
| Infused caloric fluid | 5% DNK1 1,440 mL | Nutriflex®peri 40 |
||
| Oral intake | SOW | SFD Breakfast: whole meal (300 kcal) Lunch: 2/3 meal (200 kcal) Dinner: 1/4 meal (75 kcal) |
SBD (minimal) | None (intubation status) |
| Total calories (kcal) | 244.8 | 575 | <200 | 480 |
| Biochemical parameters (reference range) | ||||
| White blood cell count (/μL) (4,000~1,000) | 7,480 | NP | 6,630 | 17,670 |
| Hemoglobin (g/dL) (13.1~17.5) | 9.4 | NP | 9.2 | 11.6 |
| Hematocrit (%) (39.0~52.0) | 29.2 | NP | 28.6 | 36.6 |
| Platelet count (×1,000/μL) (140~400) | 67 | NP | 94 | 142 |
| Na (mEq/l) (133~145) | 134 | NP | 132 | 135 |
| K (mEq/l) (3.5~5.5) | 3.6 | NP | 3.5 | 2.68 |
| Cl (mEq/l) (95~110) | 99 | NP | 95 | 95 |
| Calcium (mg/dL) (8.6~10.7) | 8.6 | NP | 8.0 | 8.3 |
| Phosphate (mg/dL) (2.5~4.5) | 2.0 | NP | 1.6 | 2.5 |
| Glucose (mg/dL) (70~100) | 92 | NP | 83 | 91 |
| Albumin (mg/dL) (3.5~5.2) | 3.1 | NP | 2.7 | 2.8 |
| BUN (mg/dL) (6~20) | 18.7 | NP | 13.7 | 23.5 |
| Creatinine (mg/dL) (0.5~1.2) | 1.06 | NP | 1.00 | 1.17 |
| Intake/output (mL/mL) | 3,000/2,920 | 2,935/3,450 | 2,935/3,450 | 1,440/1,340 |
| Intraperitoneal drainage amount (mL) | 920 | 390 | 1,220 | 160 |
| Injections | Hartmann’s solution Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g | Hartmann’s solution Tamipool® |
Hartmann’s solution KH2PO4 20 mL Tamipool® |
Levofloxacin 750 mg Piperacillin/ tazobactam 4.5 g |
| Body weight (kg) | 50.9 | 51.2 | 53.8 | 56.1 |
| Notable clinical features | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion | Pitting edema HAP with bilateral pleural effusion |
POD = postoperative day; 5% DNK1 = dextrose 5% (187 kcal/bag); SOW = sips of water; SFD: semi-fluid diet; SBD = soft blended diet; NP = not performed; HAP = hospital-acquired pneumonia.
aNutriflex®peri 40 (B. Braun Medical AG, Crissier, Switzerland); bTamipool® (BCWP, Yeoju, Korea).
Table 1
Laboratory test results and remarkable clinical characteristics according to net energy intake before resumption of oral intake
Op = operation; POD = postoperative day; 5% DNK1 = dextrose 5% (187 kcal/bag); NP = not performed; HAP = hospital-acquired pneumonia. aWinuf®peri (JW Pharmaceutical, Seoul, Korea); bVolulyte® (Fresenius Kabi Deutschland GmbH, Friedberg, Germany); cTamipool® (BCWP, Yeoju, Korea).
Table 2
Laboratory test results and notable clinical features according to net energy intake after initiating oral intake
POD = postoperative day; 5% DNK1 = dextrose 5% (187 kcal/bag); SOW = sips of water; SFD: semi-fluid diet; SBD = soft blended diet; NP = not performed; HAP = hospital-acquired pneumonia. aNutriflex®peri 40 (B. Braun Medical AG, Crissier, Switzerland); bTamipool® (BCWP, Yeoju, Korea).

