 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 14(2); 2022 > Article
- Original Article Body Compositions of Elderly and Non-Elderly Patients Following Gastrectomy for Gastric Cancer
-
Ji Hoon Kang, M.D.1,2
 , Mi Ran Jung, M.D., Ph.D.1,2, Sung Eun Kim, M.D.1,2, Oh Jeong, M.D., Ph.D., F.A.C.S.1,2
, Mi Ran Jung, M.D., Ph.D.1,2, Sung Eun Kim, M.D.1,2, Oh Jeong, M.D., Ph.D., F.A.C.S.1,2 -
DOI: https://doi.org/10.15747/ACNM.2022.14.2.81
Published online: December 1, 2022
1Divsion of Gastroenterologic Surgery, Chonnam National University Hwasun Hospital, Hwasun, Korea
2Department of Surgery, Chonnam National University Medical School, Gwangju, Korea
- Corresponding author: Oh Jeong E-mail surgeonjeong@gmail.com ORCID https://orcid.org/0000-0002-7076-6998
• Received: November 7, 2022 • Revised: November 16, 2022 • Accepted: November 16, 2022
© The Korean Society of Surgical Metabolism and Nutrition and The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,446 Views
- 7 Download
Abstract
-
Purpose Radical gastric resection is the mainstay of treatment in gastric cancer. However, patients can suffer from eating restrictions, weight loss, and malnutrition after gastrectomy, to which elderly patients are more vulnerable. We compared body composition changes in elderly patients and non-elderly patients after gastrectomy.
-
Materials and Methods This prospective study enrolled patients who underwent gastrectomy for gastric carcinoma between 2019 and 2021. Body composition was measured using bioelectrical impedance analysis (InBody S10) before surgery and up to 12 months after surgery. Patients were divided into an elderly group (>70 years) and a non-elderly group (≤70 years), and body composition changes were compared between the two groups using the linear mixed model.
-
Results There were 69 patients in the elderly group and 164 patients in the non-elderly group. The groups showed no significant differences in gastric resection or pathologic stage. Overall, body composition, including total body water, body weight, lean body mass, skeletal muscle mass, and fat mass, decreased immediately after surgery and gradually improved until postoperative 12 months. A linear mixed model showed no significant time×group interactions for any body composition factors between groups.
-
Conclusion Body composition changes did not significantly differ between elderly patients and non-elderly patients after gastrectomy.
INTRODUCTION
Gastric cancer is the fifth most common malignant disease and the fourth leading cause of cancer-related death worldwide [1]. Higher incidences of gastric cancer are observed in Asian countries: in Korea, gastric cancer remains the most prevalent malignant disease in male [2]. Despite progress in multidisciplinary treatment, radical gastric resection remains the mainstay of treatment for gastric cancer. After gastrectomy, patients suffer from poor appetite, eating restriction, gastrointestinal symptoms, and malabsorption, which can result in weight loss and nutritional deficits. With improvements in survival of gastric cancer, there is increasing emphasis on patient-centered outcomes, with appropriate management of postoperative nutrition recognized as essential to maintain better quality of life in patients undergoing gastrectomy [3].
Body composition measurement is useful for assessing nutritional status after surgery. Bioelectrical impedance analysis (BIA) is a non-invasive, safe, rapid, and accurate method for evaluating body composition and is increasingly used for nutritional assessment in patients undergoing gastrectomy. Many studies have investigated the impacts of body composition on postoperative outcomes after gastrectomy [4]. After surgery, patients show immediate changes in body composition, including loss of lean body mass (LBM) and fat mass [5,6]. Body composition remains stable or partly improves 6 to 12 months after surgery [7]. Some studies have investigated risk factors for postoperative body composition change, with sex, gastric resection, operative approach, and postoperative complications found to significantly affect body composition after gastrectomy [8,9].
Due to increases in life expectancy, it is becoming more common to operate on elderly patients. According to a nationwide survey in South Korea in 2019, approximately 30% of gastric cancer patients who underwent surgery were older than 70 years, a near threefold increase from 1995 [10]. Elderly patients often have comorbidities and reduced physiologic reserve, resulting in increased operative risk [11]. Furthermore, nutrition status and body composition undergo significant changes with age, represented by decreased muscle mass, increased adiposity, and decreased total body water [11]. We hypothesized that elderly patients experience different body composition changes after gastrectomy compared to non-elderly patients. Identifying such differences would help clinicians to establish appropriate management plans for postoperative care and nutritional support in this patient group. Therefore, the aim of this study was to investigate body composition changes in elderly gastric cancer patients undergoing gastrectomy.
MATERIALS AND METHODS
We performed a prospective study of patients who underwent gastrectomy for gastric carcinoma in the Division of Gastroenterologic Surgery at Chonnam National University Hwasun Hospital from June 2019 to June 2021. Exclusion criteria were emergency surgery for bleeding or perforation, chemotherapy or chemoradiation therapy within six months, non-resectional surgery (bypass surgery or exploratory laparotomy), and combined resection of other organs. We screened 251 patients who underwent distal or total gastrectomy for primary gastric cancer. The operative approaches included both laparoscopic and open surgery, and 18 were excluded. Finally, 233 patients were included in the analysis. We divided patients into an elderly group (>70 years) and a non-elderly group (≤70 years) and compared body composition changes between the two groups. This study was approved by the Institutional Review Board at Chonnam National University Hwasun Hospital (CNUHH2019-061). A written informed consent was obtained from all participating patients.
Patients underwent distal or total gastrectomy with regional lymph node dissection following South Korean gastric cancer treatment guidelines [12]. Laparoscopic surgery was indicated in most patients except those with very advanced disease, such as extensive lymph node metastasis or large tumor. After distal gastrectomy, Billroth-II or Roux-en Y gastrojejunostomy was performed at the surgeons' discretion. After total gastrectomy, Roux-en esophagojejunostomy was performed in all patients.
Perioperative management followed our institution's enhanced recovery after surgery (ERAS) protocols [13]. In brief, preoperative fasting was avoided, and a carbohydrate-rich drink was administered 2 hours before surgery. No mechanical bowel preparation was performed. Routine insertion of a nasogastric tube or abdominal drainage was not performed. After the operation, patients commenced an oral diet from postoperative day 1. Limited amounts of intravenous fluid were administered only for three postoperative days. Patients were discharged from the hospital starting on postoperative day 6 when they satisfied the predefined discharge criteria.
Body composition was measured using segmental multifrequency BIA (InBody S10; InBody, Co. Ltd, Seoul, Korea). We measured body composition preoperatively and at postoperative 1 month, 3 months, 6 months, and 12 months. According to the manufacturer’s protocol, patients were examined before breakfast in the morning. The patients were asked to lie comfortably on a bed while the examiner attached clamp electrodes to both arms and legs.
Using the InBody, we obtained the following data regarding body composition: intracellular water, extracellular water, body weight, skeletal muscle mass (SMM), body fat mass (BFM), percent body fat (PBF), LBM, and body mass index (BMI). Other nutritional information estimated using the InBody was body cell mass (BCM), bone mineral content (BMC), visceral fat area (VFA), and basal metabolic rate (BMR).
Data are expressed as mean±standard deviation or n (%). Categorical variables were compared using the chi-square or Fisher’s exact test as appropriate and continuous variables using Student’s t-test. A linear mixed model and paired t-test were used to assess differences in body composition changes between the two groups. P-values <0.05 were considered statistically significant. All statistical analyses were performed using SPSS, version 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Table 1 shows the baseline characteristics of elderly and non-elderly patients. The mean ages of the elderly and non-elderly groups were 75.1±3.9 and 56.5±8.4 years, respectively. The elderly group had higher American Society of Anesthesiologists scores than the non-elderly group. Operative outcomes, such as surgical approach and gastric resection, did not significantly differ between the two groups. However, D2 lymphadenectomy and Billroth II reconstruction were performed more frequently in the elderly group. The two groups showed no significant difference in final pathologic stage. All but 1 patient completed outpatient follow-up for 12 months. There were no deaths during the follow-up period. We obtained Inbody measurements for 216 patients at 1 month, 211 patients at 3 months, 204 patients at 6 months, and 183 patients at 12 months (92.7%, 90.6%, 87.6%, and 78.5% of the entire patient sample, respectively).
Short-term surgical outcomes are presented in Table 2. There was no significant difference in operating time or operative blood loss. The overall morbidities in the elderly and non-elderly groups were 17.4% and 11.6%, respectively, but this difference was not statistically significant. There were also no significant differences between the two groups in length of hospital stay, gas passage day, or diet resumption.
Fig. 1 shows body composition changes up to postoperative 12 months between the two groups. Overall, body weight, protein, muscle mass, and fat mass decreased immediately after surgery and gradually improved until postoperative 12 months. Interestingly, the decrease in BFM was remarkable until postoperative 12 months compared to body weight, SMM, and LBM changes. When body composition changes were compared between the two groups, a linear mixed model showed no significant time×group interactions for any body composition factors, including body water, protein, SMM, BFM, or LBM.
Table 3 shows detailed body composition data for the two groups. BFM showed the greatest decrease in both groups (−23.4% in the non-elderly and −26.5% in the elderly). The LBM loss in both groups was around −2.2% at postoperative six months. There were no significant differences in changes of any body composition factors at postoperative 6 and 12 months between the two groups (Fig. 1).
DISCUSSION
In the present study, we investigated chronologic changes of body composition after gastrectomy and compared such changes between elderly and non-elderly patients. The strength of this study is its prospective design and inclusion of patients receiving standardized perioperative care. We found that changes of body composition, including BMI, LBM, SMM, and fat mass, did not significantly differ between the two groups. This suggests that age does not significantly affect body composition after gastrectomy.
Elderly patients are more vulnerable to surgical stress due to physiological changes in diverse functions associated with aging. Impaired cardiovascular systems and respiratory function and disorders of fluid and electrolyte balance are common in the elderly [11]. Body composition also changes with aging. The proportion of body fat increases and is accompanied by decreases in total body water and SMM [14]. Therefore, sarcopenia is a common age-related clinical problem that increases risk in elderly patients undergoing surgery [15]. Furthermore, LBM loss after surgery is aggravated in the elderly due to several factors. Previous research showed that skeletal muscle protein synthesis tended to be lower in old individuals [16,17]. Immunologic and inflammatory responses to surgical stress, which accelerate muscle catabolism, are more profound in the elderly after surgery [18]. Postoperative oral intake tends to be inadequate in the elderly because of disability, frailty, poor appetite, frequent gastrointestinal symptoms, and socioeconomic conditions. Therefore, elderly patients may require more aggressive and tailored postoperative nutrition support, such as provision of oral nutrition supplementation or a high-protein diet.
Aoyama et al. [8] investigated risk factors for loss of LBM measured using bioelectrical impedance in patients undergoing gastrectomy and showed that infectious surgical complications, total gastrectomy, and male sex were significantly associated with severe LBM loss, but age was not. However, their study examined short-term outcomes and used an arbitrary cut-off value to define severe LBM loss. Therefore, LBM loss could not be compared adequately between the elderly and non-elderly in the study. Meanwhile, in another study comparing weight loss and body composition change in elderly (>70 years) and non-elderly patients, LBM loss was significantly more severe at 1 and 3 months after gastrectomy in elderly patients, while total body weight loss was similar between the two groups [19]. Our study showed that elderly patients had body composition changes similar to those of non-elderly patients. However, the number of elderly patients in our sample was relatively small, and elderly patients were defined as those >70 years of age. Therefore, the impact of age on body composition changes requires further investigation. Identifying differences in body composition changes in the elderly will help clinicians to develop more practical nutritional support plans.
Recently, there has been growing interest in body composition assessment in patients with gastric cancer for nutritional evaluation and prognostication. Body composition can be measured using CT, dual-energy X-ray absorptiometry, and BIA. Among these, BIA is increasingly used because it is a simple, quick, non-invasive method that can assess body composition at the bedside. Previous studies showed that body composition could be used to predict postoperative complications in patients undergoing gastrectomy. In a systematic review including 39 studies of body composition assessment in patients with gastric cancer, preoperative sarcopenia was associated with significantly higher rates of overall postoperative complications and mortality [4]. In a recent prospective study, preoperative lower skeletal mass and high visceral and subcutaneous adipose tissue radiation attenuation were associated with higher risk of major complications after gastrectomy [20]. The type and extent of surgery may impact long-term body mass and composition. Park et al. [7] showed that total gastrectomy resulted in significantly decreased protein mass, BFM, SMM, and VFA compared to distal gastrectomy at postoperative three years. The impact of operative approach (open or laparoscopy) on body composition change is controversial. In a previous study comparing open and laparoscopic distal gastrectomy, patients undergoing laparoscopic surgery showed significantly lower visceral fat loss [9]. However, another study showed no significant difference in loss of body weight and LBM between open and laparoscopic distal gastrectomy [21].
There are some limitations in this study. First, we examined patients treated at a single institution, and most of our patients had early gastric cancer. Due to nationwide screening for gastric cancer in South Korea, more than half of gastric cancer patients are diagnosed at an early stage. Therefore, the results of our study should be validated in another cohort. Second, body composition assessment using the BIA method has limited accuracy in patients with abnormal hydration states due to conditions such as malnutrition, edema, or old age [22]. Last, although we applied a prospective design, some patients failed to return for all visits to undergo body composition measurement. These missing data could influence the results.
CONCLUSION
In summary, the present study investigated body composition changes in elderly patients undergoing gastrectomy. We found that body composition in the elderly did not significantly differ from that in non-elderly patients. However, our results should be validated in future research. Information about body composition changes will help clinicians to develop practical nutritional support plans for elderly patients.
AUTHOR CONTRIBUTIONS
Conceptualization: OJ. Data curation: JHK, SEK. Formal analysis: OJ, JHK. Funding acquisition: OJ. Investigation: OJ, JHK, MRJ, SEK. Methodology: OJ. Project administration: OJ. Resources: OJ. Supervision: MRJ. Validation: OJ, MRJ. Writing – original draft: JHK. Writing – review & editing: OJ, MRJ.
CONFLICTS OF INTEREST
The authors of this manuscript have no conflicts of interest to disclose.
FUNDING
This study was supported by the research fund of the Korean Society of Surgical Metabolism and Nutrition (KSSMN) and a grant (HCRI 19016) from Chonnam National University Hospital Biomedical Research Institute.
Fig. 1
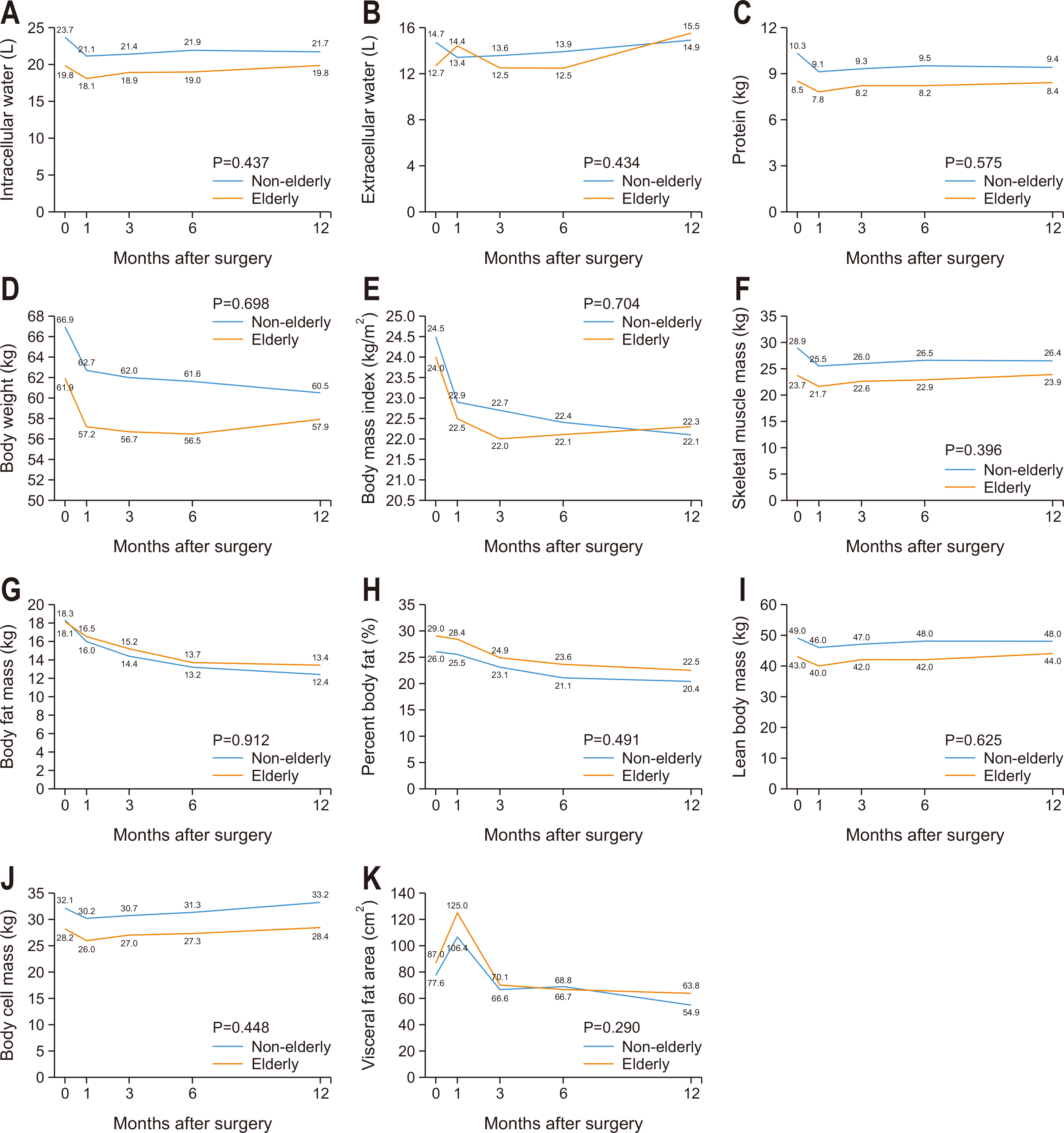
Body composition changes in non-elderly and elderly groups. (A) Intracellular water, (B) extracellular water, (C) protein, (D) body weight, (E) body mass index, (F) skeletal muscle mass, (G) body fat mass, (H) percent body fat, (I) lean body mass, (J) body cell mass, and (K) visceral fat area.
Table 1
Patient characteristics
| Variable | Non-elderly (n=164) | Elderly (n=69) | P-value | |
|---|---|---|---|---|
| Age (yr) | 56.5±8.4 | 75.1±3.9 | <0.001 | |
| Sex | Female | 52 (31.7) | 25 (36.2) | 0.503 |
| Male | 112 (68.3) | 44 (63.8) | ||
| BMI (kg/m2) | 24.4±3.2 | 24.1±3.3 | 0.489 | |
| ASA status | 1 | 62 (37.8) | 5 (7.2) | <0.001 |
| 2 | 101 (61.6) | 52 (75.4) | ||
| 3 | 1 (0.6) | 12 (17.4) | ||
| Abdominal operation history | 18 (11.0) | 8 (11.6) | 0.891 | |
| Smoking | None | 83 (50.6) | 45 (65.2) | 0.009 |
| Current | 43 (26.2) | 6 (8.7) | ||
| Former | 35 (21.3) | 18 (26.1) | ||
| Operative approach | Open | 6 (3.7) | 6 (8.7) | 0.112 |
| Laparoscopy | 158 (96.3) | 63 (91.3) | ||
| Gastric resection | Distal | 139 (84.8) | 58 (84.1) | 0.893 |
| Total | 25 (15.2) | 11 (15.9) | ||
| Lymphadenectomy | D1+ | 134 (81.7) | 48 (69.6) | 0.041 |
| D2 | 30 (18.3) | 21 (30.4) | ||
| Reconstruction | Billroth II | 69 (42.1) | 44 (63.8) | 0.002 |
| Roux-en-Y | 95 (57.9) | 25 (36.2) | ||
| Omentectomy | Partial | 149 (90.9) | 57 (82.6) | 0.073 |
| Complete | 15 (9.1) | 12 (17.4) | ||
| Tumor size (cm) | 2.8±1.6 | 3.4±1.9 | 0.599 | |
| pTa | T1 | 127 (77.4) | 44 (63.8) | 0.098 |
| T2 | 18 (11.0) | 9 (13.0) | ||
| T3 | 11 (6.7) | 11 (15.9) | ||
| T4 | 8 (4.9) | 5 (7.2) | ||
| pNa | N0 | 138 (84.1) | 51 (73.9) | 0.250 |
| N1 | 12 (7.3) | 10 (14.5) | ||
| N2 | 7 (4.3) | 5 (7.2) | ||
| N3 | 7 (4.3) | 3 (4.3) | ||
| TNM stagea | Stage I | 135 (82.3) | 50 (72.5) | 0.236 |
| Stage II | 20 (12.2) | 13 (18.8) | ||
| Stage III | 9 (5.5) | 6 (8.7) | ||
Table 2
Short-term surgical outcomes
Table 3
Rates of change in body composition in elderly and non-elderly patients
Values are presented as mean±standard deviation.
ICW = intracellular water; ECW = extracellular water; BW = body weight; BMI = body mass index; SMM = skeletal muscle mass; BFM = body fat mass; PBF = percent body fat; LBM = lean body mass; BCM = body cell mass; BMC = bone mineral content; VFA = visceral fat area; BMR = basal metabolic rate.
- 1. Ilic M, Ilic I. Epidemiology of stomach cancer. World J Gastroenterol 2022;28:1187-203. ArticlePubMedPMC
- 2. Hong S, Won YJ, Park YR, Jung KW, Kong HJ, Lee ES. Community of Population-Based Regional Cancer Registries. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2017. Cancer Res Treat 2020;52:335-50. ArticlePubMedPMCPDF
- 3. Kubota T, Shoda K, Konishi H, Okamoto K, Otsuji E. Nutrition update in gastric cancer surgery. Ann Gastroenterol Surg 2020;4:360-8. ArticlePubMedPMCPDF
- 4. Kamarajah SK, Bundred J, Tan BHL. Body composition assessment and sarcopenia in patients with gastric cancer: a systematic review and meta-analysis. Gastric Cancer 2019;22:10-22; Erratum in: Gastric Cancer 2019;22:645-50. ArticlePubMedPDF
- 5. Kiyama T, Mizutani T, Okuda T, Fujita I, Tokunaga A, Tajiri T, et al. Postoperative changes in body composition after gastrectomy. J Gastrointest Surg 2005;9:313-9. ArticlePubMed
- 6. Aoyama T, Kawabe T, Hirohito F, Hayashi T, Yamada T, Tsuchida K, et al. Body composition analysis within 1 month after gastrectomy for gastric cancer. Gastric Cancer 2016;19:645-50. ArticlePubMedPDF
- 7. Park KB, Park JY, Lee SS, Chung HY, Kwon OK. Chronological changes in quality of life and body composition after gastrectomy for locally advanced gastric cancer. Ann Surg Treat Res 2020;98:262-9. ArticlePubMedPMCPDF
- 8. Aoyama T, Sato T, Segami K, Maezawa Y, Kano K, Kawabe T, et al. Risk factors for the loss of lean body mass after gastrectomy for gastric cancer. Ann Surg Oncol 2016;23:1963-70. ArticlePubMedPDF
- 9. Park KB, Kwon OK, Yu W, Jang BC. Body composition changes after totally laparoscopic distal gastrectomy with delta-shaped anastomosis: a comparison with conventional Billroth I anastomosis. Surg Endosc 2016;30:4286-93. ArticlePubMedPDF
- 10. Information Committee of the Korean Gastric Cancer Association. Korean Gastric Cancer Association-led nationwide survey on surgically treated gastric cancers in 2019. J Gastric Cancer 2021;21:221-35. ArticlePubMedPMCPDF
- 11. Ramesh HS, Pope D, Gennari R, Audisio RA. Optimising surgical management of elderly cancer patients. World J Surg Oncol 2005;3:17.ArticlePubMedPMCPDF
- 12. Guideline Committee of the Korean Gastric Cancer Association (KGCA), Development Working Group & Review Panel. Korean practice guideline for gastric cancer 2018: an evidence-based, multi-disciplinary approach. J Gastric Cancer 2019;19:1-48; Erratum in: J Gastric Cancer 2019;19:372-3. ArticlePubMedPMCPDF
- 13. Jung MR, Ryu SY, Park YK, Jeong O. Compliance with an enhanced recovery after a surgery program for patients undergoing gastrectomy for gastric carcinoma: a phase 2 study. Ann Surg Oncol 2018;25:2366-73. ArticlePubMedPDF
- 14. Tonner PH, Kampen J, Scholz J. Pathophysiological changes in the elderly. Best Pract Res Clin Anaesthesiol 2003;17:163-77. ArticlePubMed
- 15. Fukuda Y, Yamamoto K, Hirao M, Nishikawa K, Nagatsuma Y, Nakayama T, et al. Sarcopenia is associated with severe postoperative complications in elderly gastric cancer patients undergoing gastrectomy. Gastric Cancer 2016;19:986-93. ArticlePubMedPDF
- 16. Tanner RE, Brunker LB, Agergaard J, Barrows KM, Briggs RA, Kwon OS, et al. Age-related differences in lean mass, protein synthesis and skeletal muscle markers of proteolysis after bed rest and exercise rehabilitation. J Physiol 2015;593:4259-73. ArticlePubMedPMC
- 17. Toth MJ, Matthews DE, Tracy RP, Previs MJ. Age-related differences in skeletal muscle protein synthesis: relation to markers of immune activation. Am J Physiol Endocrinol Metab 2005;288:E883-91. ArticlePubMed
- 18. Grimble RF. Inflammatory response in the elderly. Curr Opin Clin Nutr Metab Care 2003;6:21-9. PubMed
- 19. Aoyama T, Maezawa Y, Yoshikawa T, Segami K, Kano K, Hayashi T, et al. Comparison of weight and body composition after gastrectomy between elderly and non-elderly patients with gastric cancer. In Vivo 2019;33:221-7. ArticlePubMedPMC
- 20. Tweed TTT, van der Veen A, Tummers S, van Dijk DPJ, Luyer MDP, Ruurda JP, et al. Body composition is a predictor for postoperative complications after gastrectomy for gastric cancer: a prospective side study of the LOGICA trial. J Gastrointest Surg 2022;26:1373-87. ArticlePubMedPMCPDF
- 21. Aoyama T, Sato T, Hayashi T, Yamada T, Cho H, Ogata T, et al. Does a laparoscopic approach attenuate the body weight loss and lean body mass loss observed in open distal gastrectomy for gastric cancer? A single-institution exploratory analysis of the JCOG 0912 phase III trial. Gastric Cancer 2018;21:345-52. ArticlePubMedPDF
- 22. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gómez JM, et al. Composition of the ESPEN Working Group. Bioelectrical impedance analysis--part I: review of principles and methods. Clin Nutr 2004;23:1226-43. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteBody Compositions of Elderly and Non-Elderly Patients Following Gastrectomy for Gastric Cancer
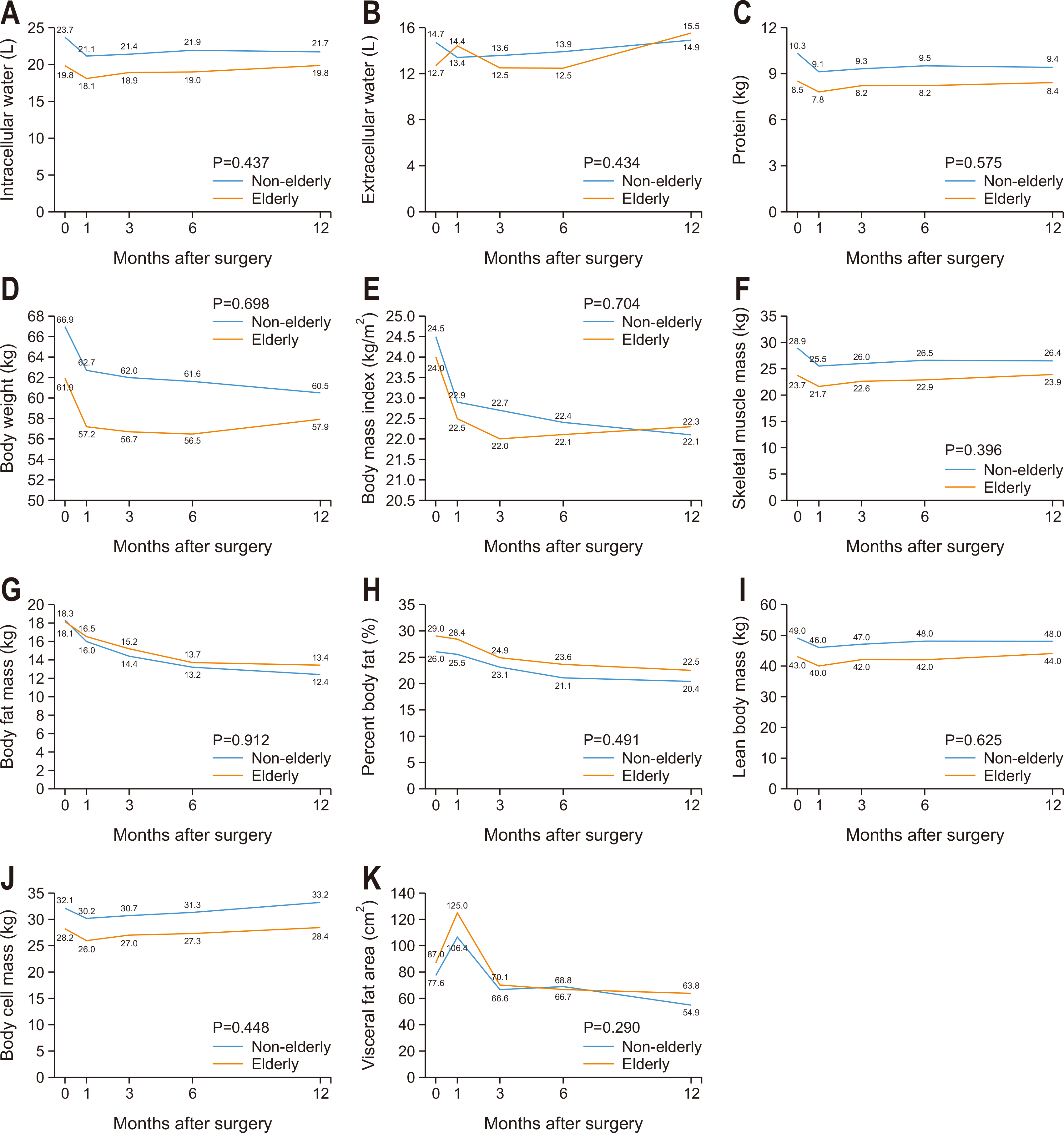
Fig. 1
Body composition changes in non-elderly and elderly groups. (A) Intracellular water, (B) extracellular water, (C) protein, (D) body weight, (E) body mass index, (F) skeletal muscle mass, (G) body fat mass, (H) percent body fat, (I) lean body mass, (J) body cell mass, and (K) visceral fat area.
Fig. 1
Body Compositions of Elderly and Non-Elderly Patients Following Gastrectomy for Gastric Cancer
Patient characteristics
| Variable | Non-elderly (n=164) | Elderly (n=69) | P-value | |
|---|---|---|---|---|
| Age (yr) | 56.5±8.4 | 75.1±3.9 | <0.001 | |
| Sex | Female | 52 (31.7) | 25 (36.2) | 0.503 |
| Male | 112 (68.3) | 44 (63.8) | ||
| BMI (kg/m2) | 24.4±3.2 | 24.1±3.3 | 0.489 | |
| ASA status | 1 | 62 (37.8) | 5 (7.2) | <0.001 |
| 2 | 101 (61.6) | 52 (75.4) | ||
| 3 | 1 (0.6) | 12 (17.4) | ||
| Abdominal operation history | 18 (11.0) | 8 (11.6) | 0.891 | |
| Smoking | None | 83 (50.6) | 45 (65.2) | 0.009 |
| Current | 43 (26.2) | 6 (8.7) | ||
| Former | 35 (21.3) | 18 (26.1) | ||
| Operative approach | Open | 6 (3.7) | 6 (8.7) | 0.112 |
| Laparoscopy | 158 (96.3) | 63 (91.3) | ||
| Gastric resection | Distal | 139 (84.8) | 58 (84.1) | 0.893 |
| Total | 25 (15.2) | 11 (15.9) | ||
| Lymphadenectomy | D1+ | 134 (81.7) | 48 (69.6) | 0.041 |
| D2 | 30 (18.3) | 21 (30.4) | ||
| Reconstruction | Billroth II | 69 (42.1) | 44 (63.8) | 0.002 |
| Roux-en-Y | 95 (57.9) | 25 (36.2) | ||
| Omentectomy | Partial | 149 (90.9) | 57 (82.6) | 0.073 |
| Complete | 15 (9.1) | 12 (17.4) | ||
| Tumor size (cm) | 2.8±1.6 | 3.4±1.9 | 0.599 | |
| pT |
T1 | 127 (77.4) | 44 (63.8) | 0.098 |
| T2 | 18 (11.0) | 9 (13.0) | ||
| T3 | 11 (6.7) | 11 (15.9) | ||
| T4 | 8 (4.9) | 5 (7.2) | ||
| pN |
N0 | 138 (84.1) | 51 (73.9) | 0.250 |
| N1 | 12 (7.3) | 10 (14.5) | ||
| N2 | 7 (4.3) | 5 (7.2) | ||
| N3 | 7 (4.3) | 3 (4.3) | ||
| TNM stage |
Stage I | 135 (82.3) | 50 (72.5) | 0.236 |
| Stage II | 20 (12.2) | 13 (18.8) | ||
| Stage III | 9 (5.5) | 6 (8.7) | ||
Values are presented as mean±standard deviation or number (%).
BMI = body mass index; ASA classification = American Society of Anesthesiologists physical status classification.
apTNM stages are based on the American Joint Committee on Cancer TNM classification, seventh edition.
Short-term surgical outcomes
| Variable | Non-elderly (n=164) | Elderly (n=69) | P-value |
|---|---|---|---|
| Operating time (min) | 180.6±63.6 | 163.5±56.8 | 0.055 |
| Operative blood loss (mL) | 35.5±62.0 | 30.7±25.8 | 0.531 |
| Morbidity | 19 (11.6) | 12 (17.4) | 0.234 |
| Local | 19 (11.6) | 11 (15.9) | 0.365 |
| Systemic | 2 (1.2) | 1 (1.4) | 0.887 |
| Mortality | 0 | 0 | |
| Harvested lymph nodes | 50.6±18.5 | 55.1±21.1 | 0.105 |
| Blood transfusion | 3 (1.8) | 1 (1.5) | 0.844 |
| Fever | 5 (3.0) | 5 (7.2) | 0.149 |
| Gas passage (day) | 2.7±1.0 | 2.6±0.8 | 0.148 |
| Diet resumption (day) | 1.8±2.1 | 1.7±1.6 | 0.701 |
| Hospital stay (day) | 7.5±2.0 | 7.5±1.5 | 0.914 |
Values are presented as mean±standard deviation or number (%).
Rates of change in body composition in elderly and non-elderly patients
| Variable | Baseline | 6 months | 12 months | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-elderly (n=164) | Elderly (n=69) | Non-elderly (n=143) | Elderly (n=61) | P-value | Non-elderly (n=135) | Elderly (n=48) | P-value | |||
| ICW (L) | 23.7±17.1 | 19.8±3.7 | –3.3±9.2 | –3.5±9.9 | 0.879 | –2.5±10.1 | –1.9±7.6 | 0.712 | ||
| ECW (L) | 14.7±10.1 | 12.7±2.4 | –1.7±8.4 | –0.9±8.0 | 0.543 | –0.6±10.5 | 0.1±7.0 | 0.654 | ||
| Protein (kg) | 10.3±7.4 | 8.5±1.6 | –3.4±8.8 | –2.7±8.7 | 0.593 | –2.8±9.5 | –3.4±14.2 | 0.756 | ||
| Mineral (kg) | 3.3±0.7 | 2.9±0.5 | –0.9±8.6 | –0.2 ±10.5 | 0.629 | 0.7±9.4 | 1.1±10.5 | 0.846 | ||
| BW (kg) | 66.9±11.2 | 61.9±12.4 | –9.27±11.3 | –8.3±11.7 | 0.579 | –9.0±6.5 | –8.0±10.5 | 0.449 | ||
| BMI (kg/m2) | 24.5±3.2 | 24.0±3.6 | –8.4±7.1 | –7.0±12.1 | 0.285 | –9.0±6.6 | –6.8±11.4 | 0.106 | ||
| SMM (kg) | 28.9±22.3 | 23.7±4.9 | –3.7±9.4 | –3.1±9.3 | 0.697 | –2.8±9.8 | –2.0±8.3 | 0.614 | ||
| BFM (kg) | 18.3±13.4 | 18.1±7.6 | –23.4±21.8 | –26.5±20.6 | 0.362 | –28.1±27.5 | –26.8±28.2 | 0.776 | ||
| PBF (%) | 26.0±8.7 | 29.0±8.0 | –16.8±21.6 | –17.1±23.5 | 0.928 | –20.9±25.5 | –21.6±27.1 | 0.874 | ||
| LBM (kg) | 49.5±10.0 | 43.8±8.2 | –2.3±5.4 | –2.1±8.4 | 0.826 | –1.5±6.1 | –1.1±7.4 | 0.718 | ||
| BCM (kg) | 32.1±6.6 | 28.2±5.4 | –2.9 ±5.6 | –2.9 ±8.6 | 0.962 | –2.0±6.2 | –1.8±7.7 | 0.854 | ||
| BMC (kg) | 2.7±0.6 | 2.4±0.4 | –0.7±9.3 | 0.4 ±10.9 | 0.489 | 1.2±9.9 | 1.8±10.7 | 0.744 | ||
| VFA (cm2) | 77.6±37.3 | 87.0±42.3 | –19.7±30.7 | –20.0±32.2 | 0.943 | –29.7±30.3 | –24.3±36.5 | 0.323 | ||
| BMR (kcal) | 1,448.6±177.9 | 1,316.0±177.9 | –1.7±7.5 | –1.5±6.1 | 0.823 | –1.8±11.5 | –0.8±5.3 | 0.534 | ||
Values are presented as mean±standard deviation.
ICW = intracellular water; ECW = extracellular water; BW = body weight; BMI = body mass index; SMM = skeletal muscle mass; BFM = body fat mass; PBF = percent body fat; LBM = lean body mass; BCM = body cell mass; BMC = bone mineral content; VFA = visceral fat area; BMR = basal metabolic rate.
Table 1
Patient characteristics
Values are presented as mean±standard deviation or number (%). BMI = body mass index; ASA classification = American Society of Anesthesiologists physical status classification. apTNM stages are based on the American Joint Committee on Cancer TNM classification, seventh edition.
Table 2
Short-term surgical outcomes
Values are presented as mean±standard deviation or number (%).
Table 3
Rates of change in body composition in elderly and non-elderly patients
Values are presented as mean±standard deviation. ICW = intracellular water; ECW = extracellular water; BW = body weight; BMI = body mass index; SMM = skeletal muscle mass; BFM = body fat mass; PBF = percent body fat; LBM = lean body mass; BCM = body cell mass; BMC = bone mineral content; VFA = visceral fat area; BMR = basal metabolic rate.

