 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 15(1); 2023 > Article
- Original article Comparison of a volume-based feeding protocol with standard feeding for trauma patients in intensive care units in Korea: a retrospective cohort study
-
Juhong Park1
 , Yesung Oh2, Songhee Kwon2, Ji-hyun Lee2, Mihyang Kim2, Kyungjin Hwang1, Donghwan Choi1, Junsik Kwon1
, Yesung Oh2, Songhee Kwon2, Ji-hyun Lee2, Mihyang Kim2, Kyungjin Hwang1, Donghwan Choi1, Junsik Kwon1 -
Annals of Clinical Nutrition and Metabolism 2023;15(1):22-29.
DOI: https://doi.org/10.15747/ACNM.2023.15.1.22
Published online: April 1, 2023
1Division of Trauma Surgery, Department of Surgery, Ajou University School of Medicine, Suwon, Korea
2Department of Food Services and Clinical Nutrition, Ajou University Hospital, Suwon, Korea
- Corresponding author: Junsik Kwon, email: aquaestel@gmail.com
• Received: February 2, 2023 • Revised: March 16, 2023 • Accepted: March 19, 2023
© 2023 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 6,263 Views
- 83 Download
- 1 Crossref
Abstract
-
Purpose Although early enteral nutrition for critically ill patients is essential, it is difficult to provide enteral nutrition to trauma patients in early hospitalization stages due to frequent surgeries and examinations. We aimed to identify the effect of achieving early enteral nutrition goals and improving outcomes through a volume-based feeding (VBF) protocol for trauma patients.
-
Methods Patients who were admitted to the trauma intensive care units (TICUs) of the Ajou University Hospital from January 2020 to September 2021 and received enteral tube feeding for at least 7 days were studied. An institution-specific VBF protocol was developed, and nurses were trained in its execution. We retrospectively compared outcomes, such as in-hospital mortality and initial nutritional goal achievement, between the new and standard protocols.
-
Results Among 2,935 patients, 109 met the inclusion criteria. Of these, 64 patients received nutrition through VBF, with no feeding intolerance symptoms. The VBF group started enteral nutrition approximately 16.9 hours earlier and group achieved 80% of the target calorie and protein intake approximately one day faster than the control group (n=45). The average calorie supply per body weight per day was 4.9 kcal/kg/day more in the VBF group. An increase of 0.2 g/kg/day was also observed in protein uptake. However, mortality and adverse hospital events did not differ between the groups.
-
Conclusion The VBF protocol for patients admitted to the TICU increased the initial nutrient supply without risk of feeding intolerance, but there was no improvement in major clinical outcomes, including mortality and adverse hospital events.
Introduction
Adequate nutritional support is important in severely ill patients. In recent years, the importance of adequate nutritional support has been highlighted because catabolic activity and a negative nitrogen balance resulting from systemic inflammation induced by severe stress such as trauma are associated with a poor prognosis. Therefore, an inadequate supply of calories and major nutrients to trauma patients can result in significant negative outcomes. In trauma patients, like other intensive care unit (ICU) patients, timely enteral feeding plays a positive prognostic role, and the existing enteral nutrition (EN) strategy is related significantly to good outcomes in nutrient delivery [1]. However, situations such as gastrointestinal trauma or surgery/examination requiring fasting while hospitalized in the ICU impede the supply of target calories and proteins [2,3]. Several evidence-based protocols applicable to trauma patients have been shown to increase the reliability of nutritional therapy provided to ICU patients [4,5]. Institutions utilizing EN protocols have shown significant improvements in nutrition practice compared with facilities that do not use such approaches [6]. Volume-based feeding (VBF) protocols have been shown to be effective in achieving the targeted daily feeding goals in trauma patients requiring frequent imaging examinations or surgeries [7]. However, many trauma surgeons and physicians are reluctant to implement VBF protocols due to safety concerns. Adding to the surgeons’ reluctance is the lack of well-designed clinical studies in surgical and traumatic ICU populations. Although studies have reported successful increase in energy transfer using VBF protocols, the clinical outcomes of such protocols have not been established [8].
This study’s aim was to determine if implementation of a VBF protocol for adult trauma patients admitted to a single trauma center could help achieve early EN goals and improve clinical outcomes.
Methods
This study was approved by the Institutional Review Board of the Ajou University Hospital (approval number: AJOUIRB-MDB-2021-580). The committee waived the need for informed consent due to the observational design of the study, which posed little risk to the study population.
It is a retrospective cohort study. It was described according to the STROBE statement available at: https://www.strobe-statement.org/.
This study was conducted at a 40-bed trauma intensive care center from October 2020 to September 2021. This trauma center has the capacity to provide in-patient treatment to about 3,000 trauma patients per year. The center also participates in the Trauma Quality Improvement Program of the American College of Surgeons, in which it is compared with Level I/II trauma centers in the United States, to achieve quality control.
Prior to the introduction of the new EN protocol (VBF protocol), a multidisciplinary trauma team assessed the patient’s condition during morning rounds in the trauma intensive care unit (TICU). A registered dietitian belonging to the multidisciplinary trauma team identified high-risk patients based on The Nutrition Risk in Critically Ill score for nutrition. The target calorie intake for these patients was in the range of 25–30 kcal/kg/day considering the patient’s nutritional characteristics; for some patients, it was determined considering the basal energy expenditure evaluated using an indirect calorimeter. Patients who were unable to eat orally for a long period of time underwent EN with insertion of a feeding tube via nasogastric or percutaneous endoscopic gastrostomy. The target protein was calculated as 1.3–3.0 g/kg/day and was adjusted with reference to patient weight change and prealbumin level. During morning rounds, the attending physician updated the patient’s clinical condition and prescribed the rate of tube feeding for the day. Although there were minor differences among patients, the rate of enteral feeding generally started at 20 mL/h and increased by 20 mL/h every 4 hours until the target rate was reached.
A new EN protocol involving volume-based principles was developed over approximately 6 months, from March to August 2020. According to the new protocol, the charge nurse initiated EN immediately following patient hospitalization upon approval of the attending physician, without waiting for an evaluation by the multidisciplinary team. Once the patient reached the target enteral feeding rate, if feeding was interrupted due to examination or surgery, the charge nurse applied the recalculated speed to achieve the original target volume faster when feeding was restarted (Fig. 1). To apply the new EN (VBF) protocol, ICU nurses were trained for approximately two months. The new EN protocol was applied to patients assigned to nurses trained in the new EN protocol, and the existing EN protocol was applied to patients who were not assigned to these nurses. During admission, patients were randomly assigned to a charge nurse.
The patients included in the study were adults aged 18 years or older who were admitted to the TICU for at least 72 hours.
The primary outcome variable is in-hospital mortality, and the secondary outcomes are the start time of EN, the number of calories and amount of protein supplied, and the time required to reach the target amount.
Data were from the electronic medical records of the institute. Variables were extracted with patient’s information and clinical course. The outcomes of patients admitted to the TICU were compared between the group that utilized the VBF protocol and the group that did not.
There was no potential source of bias in selecting participants.
Since it is a retrospective study, sample size estimation was not done. All participants were selected according to the inclusion and exclusion criteria.
All statistical analysis were performed using the Statistical Product and Service Solution IBM SPSS version 23.0 (IBM Corp.). Student’s t-test and analysis of variance were applied for quantitative data analysis, and the chi-square test was applied for qualitative data analysis. To study categorical variables with expected cell frequencies less than five, Fisher’s exact test was applied. Statistical significance decreased to P<0.05. For descriptive statistics, normally distributed data are presented as the mean±standard deviation, and nonparametric data are presented as the median.
Results
A total of 2,935 patients visited the trauma center from October 2020 to September 2021; of these, 1,872 patients were admitted to the TICU and 388 underwent EN. Among the 388 patients, 163 stayed in the TICU for less than 72 hours, and 114 patients died within seven days of starting EN or were successfully transitioned to a complete oral diet and stopped tube feeding during the study period. Additionally, two pediatric patients younger than 18 years were excluded from the study, resulting in a total of 109 patients analyzed in this study. Of these 109 patients, 64 received EN according to the VBF protocol, while the rest received standard EN care (Fig. 2). There were no statistically significant differences in age, sex, body mass index, trauma severity indicators (Injury Severity Score, Trauma and Injury Severity Score, Glasgow Coma Scale), 24-hour red blood cell transfusion volume, and number of operations or laparotomies between the two groups. Further, there was no statistical difference between the VBF and control groups in terms of number of symptoms related to feeding intolerance, such as ileus, vomiting, constipation, diarrhea, and abdominal distension (Table 1). Three patients in the VBF group discontinued tube feeding due to feeding intolerance, a smaller number than in the control group (Table 2). According to the protocol, maintenance, reduction, or discontinuation of feeding was determined according to the severity of symptoms (Fig. 1).
Clinical outcomes
Clinical outcomes between the two groups, such as mortality, number of days in the ICU, or complication rate showed no differences during the study period. The average time to start EN in the VBF group was 16.9 hours earlier than that in the control group (P<0.01).
Target calories and proteins
There was no difference in target calories and proteins between the two groups (P=0.49), and there was no difference in the frequency of patients who succeeded in achieving 80% of the target calorie (P=0.11) and protein supply (P=0.31). The VBF group established this 80% of the target calorie (P<0.001) and protein intake (P=0.04) an average of one day faster than the control group (Fig. 3). During the study period, the VBF group had larger average daily supply of calories (P<0.001) and protein (P<0.001) per body weight than did the control group (Table 3).
Discussion
In trauma patients, EN is often interrupted due to frequent imaging examinations and surgeries. Therefore, trauma patients are more likely to fail in early EN targets compared to medical patients or elective surgical patients [9]. For trauma patients, it is extremely important to establish a well-designed protocol to successfully set and achieve target calorie and protein amounts for nutrition supply. Our data are expected to help in developing protocols for proper nutrition in patients with severe trauma. It was identified that the daily energy and protein goals could be achieved more quickly using our protocol compared to the traditional method, and that there was a high possibility of supplying more energy and protein through the early stage of hospitalization. In addition, the new protocol did not cause adverse symptoms related to feeding intolerance, such as vomiting or diarrhea.
Although many studies are published on the efficacy and safety of VBF in the medical ICU [10,11], well designed studies in patients with severe trauma are lacking. Although unique surgical requirements or pathophysiological characteristics of severe trauma patients, such as damage control surgery or temporary abdominal closure, can create a potentially unsuitable environment, enteral feeding is an important tool for treatment of traumatized patients. Roberts et al. [12] recently published a retrospective review in Journal of Parenteral and Enteral Nutrition (JPEN) and examined the outcomes of patients with severe trauma admitted to surgical and medical ICUs within 48 hours of requiring mechanical ventilation. There were 171 patients who met the inclusion criteria, 25 of whom were trauma patients, and 16 of whom were treated with a VBF protocol. During the first 12 days of hospitalization, either ratio-based or volume-based EN plans were used (n=85 and n=86, respectively). Within the VBF group, energy supply increased 8.9% and protein supply increased 7.7%. In addition, the VBF group received more calories and protein, although its inclusion of only trauma patients resulted in a more homogeneous patient population than in other ICU types. Another study on provision of appropriate EN for trauma patients admitted to the ICU was recently published in JPEN and compared control (n=121) and study patients in a trauma ICU (n=118). They suggested three principles to enhance nutrient delivery.
First, EN should be initiated as quickly as possible. Second, fasting was limited, and proper nutrition was provided to the patient before surgery. Third, if the patient had been fasting for a certain period, additional nutrition was supplied through a separate protocol. This strategy can serve as a reference for other organizations that seek to incorporate similar guidelines. Those authors concluded that their approach started EN sooner, reduced the time to reach calorie goals, and improved overall EN delivery. The authors also reported an additive effect of reduced pneumonia in the intervention group. However, in our study, improvements were not demonstrated in adverse hospital events, such as pneumonia, acute kidney injury, and urinary tract infection, as well as in-hospital mortality. Many of the benefits of proper nutrition cannot be ascertained until the patient has fully recovered. This study was also incapable of identifying long-term prognoses by reviewing patient records to determine outcomes, such as 1-year mortality or readmission rates. In addition, this study did not reflect the variability in patients’ nutritional supply after discharge. To provide evidence for the significance of adequate nutrition after discharge to long-term prognosis [13-16], an additional follow-up is required for the patient group included in this study.
When developing novel feeding protocols, safety is an important factor. This is particularly true for patients with severe traumatic brain injury or spinal cord trauma, as secondary intestinal obstruction and gastric motility disorders are frequent. Vomiting is the most common safety issue experienced by such patients. Feeding intolerance symptoms, including vomiting, are tallied in nursing records and showed that the number of vomiting and feeding intolerance events did not increase after introduction of the VBF protocol. Although the difference was not statistically significant, there was a small tendency to discontinue EN with the VBF protocol due to these symptoms. However, a recent multi-center, pilot, randomized, controlled trial with a small number of patients reported increased vomiting and pointed out that these issues complicated the protocol [17].
This study had some limitations. First, data collection and analysis were conducted retrospectively and were not randomized or blinded. A blinded study design was not possible because bedside nurses recorded the respective changes in feeding rates of patients according to circumstances. Second, the EN products used in the study were not uniform. The total amounts of calories and proteins provided through EN products were used as data, but compositional ingredients can vary from product to product, which might have affected the results. Finally, this study excluded patients during the first 72 hours of their ICU stay. This exclusion most likely did not affect the overall pattern and significance of the data points [18]; however, this could not be proven. To confirm the full effect of tube feeding, patients who were briefly admitted to the ICU were excluded.
Above results can be generalized in the trauma center in other area in Korea with same protocol of the EN.
This study aimed to confirm the validity of a VBF strategy for injured patients admitted to an ICU. The novel protocol increased the initial nutrient supply without increasing the risk of enteral intolerance-related symptoms; however, no improvement in mortality was observed.
Acknowledgments
None.
Authors’ contribution
Conceptualization: JL, MK, JK. Data curation: YO, SK, JL, MK, JK. Formal analysis: MK, JK. Funding acquisition: JK. Investigation: YO, SK, MK, JK. Methodology: MK, JL, DC, JK. Project administration: JK. Resources: JP, YO, SK, JL, MK, DC, JK. Software: KH, JK. Supervision: JK. Validation: JP, JL, DC, JK. Visualization: KH, JP, JK. Writing – original draft: JP, JK. Writing – review & editing: JP, JK.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
This work was supported by the Korean Society for Parenteral and Enteral Nutrition.
Data availability
Contact the corresponding author for data availability.
Supplementary materials
None.
Fig. 1
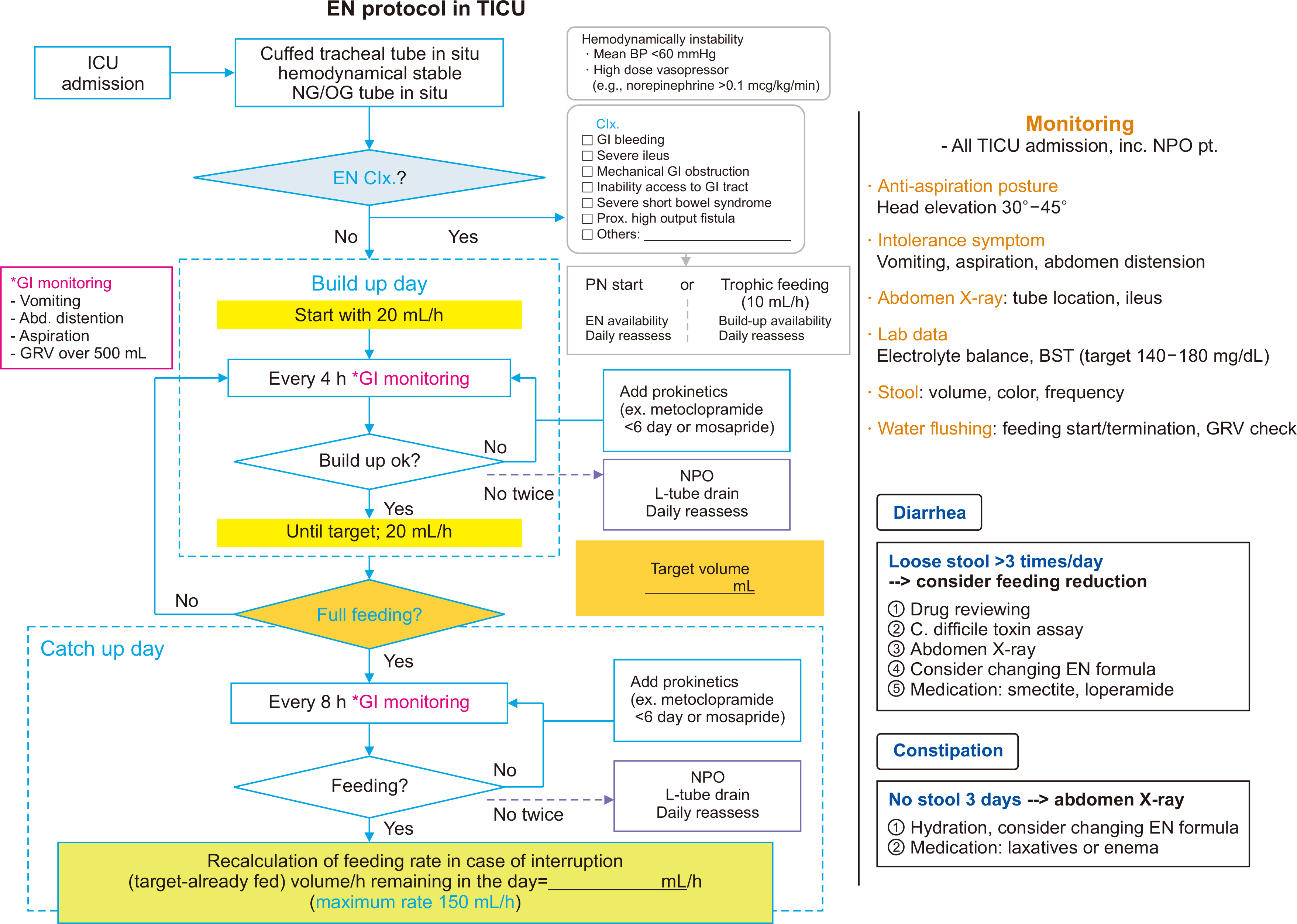
Volume-based feeding algorithm.
EN = enteral nutrition; TICU = trauma intensive care unit; ICU = intensive care unit; NG = nasogastric; OG = orogastric; CIx. = contraindication; GI = gastrointestinal; Abd. = abdominal; GRV = gastric residual volume; BP = blood pressure; Prox. = proximal; PN = parenteral nutrition; NPO = nil per os; BST = blood sugar test; C. difficile = clostridium difficile.
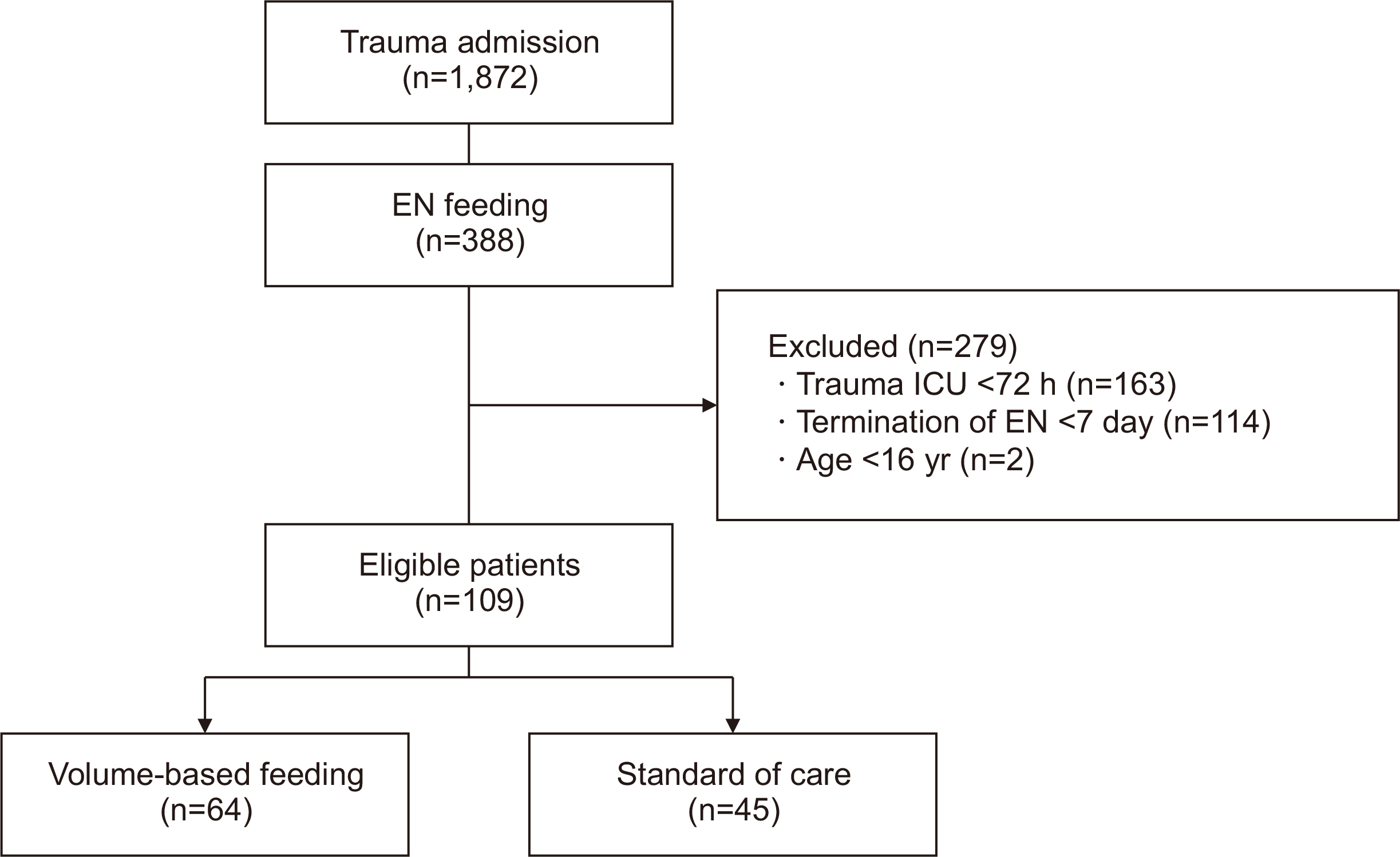
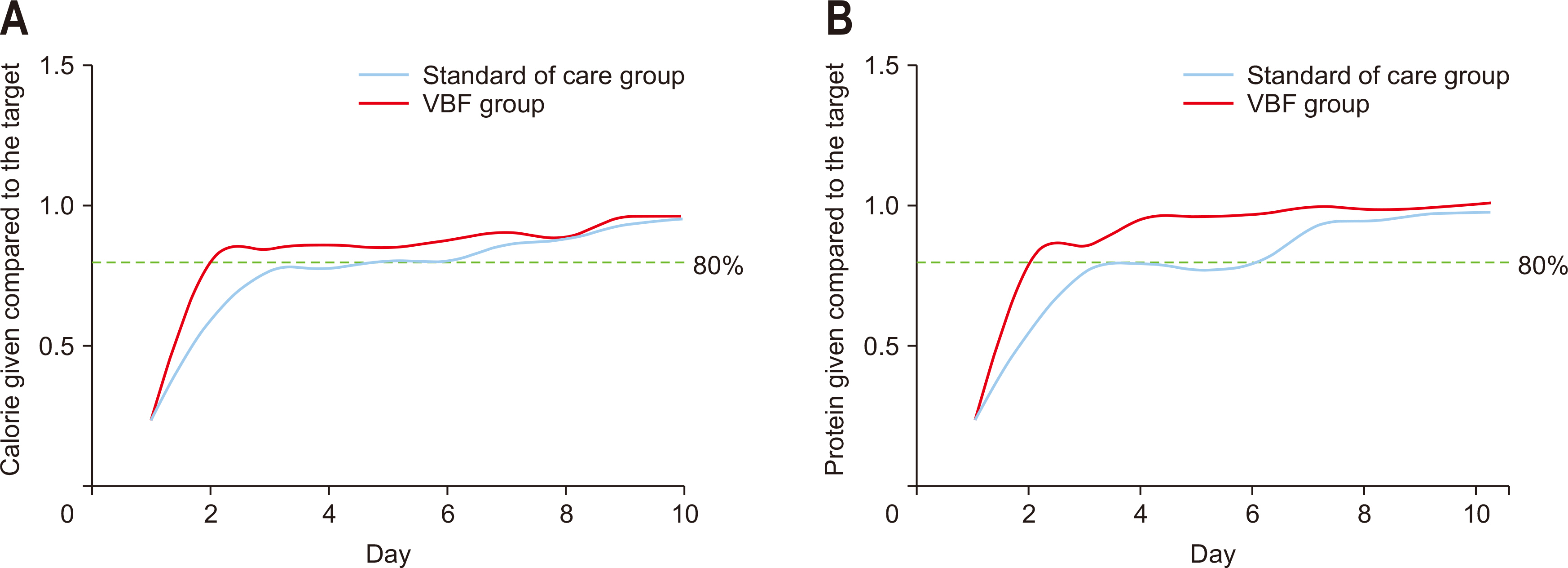
Table 1
Patient demographics and enteral nutrition tolerances
Table 2
Enteral nutrition status at the end of follow-up
Table 3
Primary and secondary outcomes of patients
| Outcome |
VBF (n=64) |
Standard of care (n=45) |
P-value |
|---|---|---|---|
| Primary outcomes | |||
| Mortality | 6 (9.4) | 2 (4.4) | 0.47 |
| ICU LOS (day) | 16.5 (12.0–25.5) | 19 (11–30) | 0.71 |
| Hospital LOS (day) | 31.5 (22.8–46.0) | 39 (20–51) | 0.40 |
| Total ventilator days (day) | 10.5 (6.0–15.5) | 12 (8–22) | 0.28 |
| Sepsis | 6 (9.4) | 2 (4.4) | 0.47 |
| Pneumonia | 25 (39.1) | 16 (35.6) | 0.71 |
| ARDS | 7 (10.9) | 6 (13.3) | 0.70 |
| AKI | 4 (6.3) | 4 (8.9) | 0.72 |
| UTI | 3 (4.7) | 2 (4.4) | >0.99 |
| Delirium | 23 (35.9) | 18 (40.0) | 0.67 |
| Secondary outcomes | |||
| Time to EN initiation (h) | 24.6 (18.7–41.1) | 41.5 (22.0–58.1) | <0.01* |
| Target calorie (kcal/day) | 1,730.5 (1,581–1,860) | 1,725 (1,473–1,905) | 0.49 |
| Target 80% of calories achieved | 59 (92.2) | 37 (82.2) | 0.11 |
| Day on which 80% was achieved (day) | 2 (2–3) | 3 (2–5) | <0.01* |
| Calorie per body weight (kcal/kg/day) | 20.5 (16.0–24.7) | 15.6 (12.8–18.6) | <0.01* |
| Target protein (g/day) | 82 (74.5–88.6) | 77.7 (68.0–87.4) | 0.15 |
| Target 80% of calories achieved | 57 (89.1) | 37 (82.2) | 0.31 |
| Day when 80% protein was achieved (day) | 2 (2–3) | 3 (2–4) | 0.04* |
| Protein per body weight (g/kg/day) | 1.0 (0.8–1.2) | 0.8 (0.6–0.9) | <0.01* |
- 1. Alberda C, Gramlich L, Jones N, Jeejeebhoy K, Day AG, Dhaliwal R, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med 2009;35:1728-37; Erratum in: Intensive Care Med 2009;35:1821. ArticlePubMedPDF
- 2. Villet S, Chiolero RL, Bollmann MD, Revelly JP, Cayeux RNMC, Delarue J, et al. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin Nutr 2005;24:502-9. ArticlePubMed
- 3. Yeh DD, Fuentes E, Quraishi SA, Cropano C, Kaafarani H, Lee J, et al. Adequate nutrition may get you home: effect of caloric/protein deficits on the discharge destination of critically ill surgical patients. JPEN J Parenter Enteral Nutr 2016;40:37-44. PubMed
- 4. Barr J, Hecht M, Flavin KE, Khorana A, Gould MK. Outcomes in critically ill patients before and after the implementation of an evidence-based nutritional management protocol. Chest 2004;125:1446-57. ArticlePubMed
- 5. Doig GS, Simpson F, Finfer S, Delaney A, Davies AR, Mitchell I, et al. Nutrition Guidelines Investigators of the ANZICS Clinical Trials Group. Effect of evidence-based feeding guidelines on mortality of critically ill adults: a cluster randomized controlled trial. JAMA 2008;300:2731-41. ArticlePubMed
- 6. Heyland DK, Cahill NE, Dhaliwal R, Sun X, Day AG, McClave SA. Impact of enteral feeding protocols on enteral nutrition delivery: results of a multicenter observational study. JPEN J Parenter Enteral Nutr 2010;34:675-84. PubMed
- 7. Taylor SJ, Fettes SB, Jewkes C, Nelson RJ. Prospective, randomized, controlled trial to determine the effect of early enhanced enteral nutrition on clinical outcome in mechanically ventilated patients suffering head injury. Crit Care Med 1999;27:2525-31. ArticlePubMed
- 8. Haskins IN, Baginsky M, Gamsky N, Sedghi K, Yi S, Amdur RL, et al. Volume-based enteral nutrition support regimen improves caloric delivery but may not affect clinical outcomes in critically ill patients. JPEN J Parenter Enteral Nutr 2017;41:607-11. ArticlePubMedPDF
- 9. McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. American Society for Parenteral and Enteral Nutrition. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2016;40:159-211; Erratum in: JPEN J Parenter Enteral Nutr 2016;40:1200. PubMed
- 10. Heyland DK, Murch L, Cahill N, McCall M, Muscedere J, Stelfox HT, et al. Enhanced protein-energy provision via the enteral route feeding protocol in critically ill patients: results of a cluster randomized trial. Crit Care Med 2013;41:2743-53. PubMed
- 11. Krebs ED, O'Donnell K, Berry A, Guidry CA, Hassinger TE, Sawyer RG. Volume-based feeding improves nutritional adequacy in surgical patients. Am J Surg 2018;216:1155-9. ArticlePubMed
- 12. Roberts S, Brody R, Rawal S, Byham-Gray L. Volume-based vs rate-based enteral nutrition in the intensive care unit: impact on nutrition delivery and glycemic control. JPEN J Parenter Enteral Nutr 2019;43:365-75. ArticlePubMedPDF
- 13. Lee JC, Williams GW, Kozar RA, Kao LS, Mueck KM, Emerald AD, et al. Multitargeted feeding strategies improve nutrition outcome and are associated with reduced pneumonia in a level 1 trauma intensive care unit. JPEN J Parenter Enteral Nutr 2018;42:529-37. ArticlePubMedPDF
- 14. Elia M, Normand C, Norman K, Laviano A. A systematic review of the cost and cost effectiveness of using standard oral nutritional supplements in the hospital setting. Clin Nutr 2016;35:370-80. ArticlePubMed
- 15. Stratton RJ, Hébuterne X, Elia M. A systematic review and meta-analysis of the impact of oral nutritional supplements on hospital readmissions. Ageing Res Rev 2013;12:884-97. ArticlePubMed
- 16. Wischmeyer PE, Carli F, Evans DC, Guilbert S, Kozar R, Pryor A, et al. Perioperative Quality Initiative (POQI) 2 Workgroup. American Society for Enhanced Recovery and Perioperative Quality Initiative joint consensus statement on nutrition screening and therapy within a surgical enhanced recovery pathway. Anesth Analg 2018;126:1883-95; Erratum in: Anesth Analg 2018;127:e95. ArticlePubMed
- 17. Yeh DD, Ortiz LA, Lee JM, Chan J, McKenzie K, Young B, et al. PEP uP (enhanced protein-energy provision via the enteral route feeding protocol) in surgical patients-a multicenter pilot randomized controlled trial. JPEN J Parenter Enteral Nutr 2020;44:197-204. ArticlePubMedPDF
- 18. Sachdev G, Backes K, Thomas BW, Sing RF, Huynh T. Volume-based protocol improves delivery of enteral nutrition in critically ill trauma patients. JPEN J Parenter Enteral Nutr 2020;44:874-9. ArticlePubMedPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Early initiation of gastric tube feeding: ultrasound assessment. A prospective interventional study
Islam M. Elbardan, Ahmed A. Alla Ossman, Nada El Kayal, Assem A. ElRazek Abd-Rabih
Research and Opinion in Anesthesia & Intensive Care.2024; 11(4): 270. CrossRef
 Cite
Cite- Figure
-
- Related articles
-
- Association of soy oil-based lipid injectable emulsion with early body weight loss after minimally invasive esophagectomy in Japan: a retrospective cohort study
- Association between decreased dietary intake during hospitalization and long-term weight loss in postoperative gastric cancer patients over 75 years of age: a retrospective cohort study
Comparison of a volume-based feeding protocol with standard feeding for trauma patients in intensive care units in Korea: a retrospective cohort study
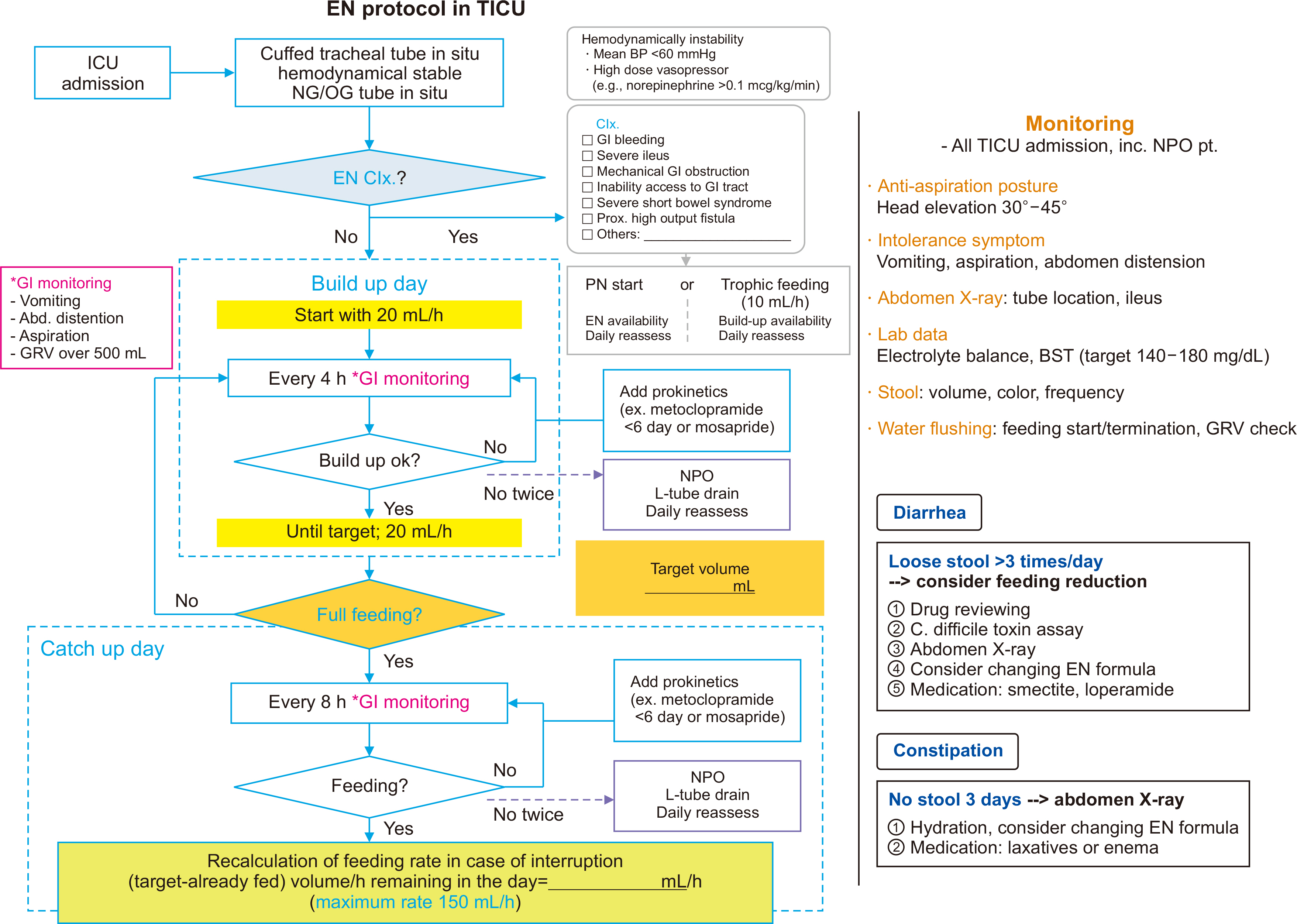
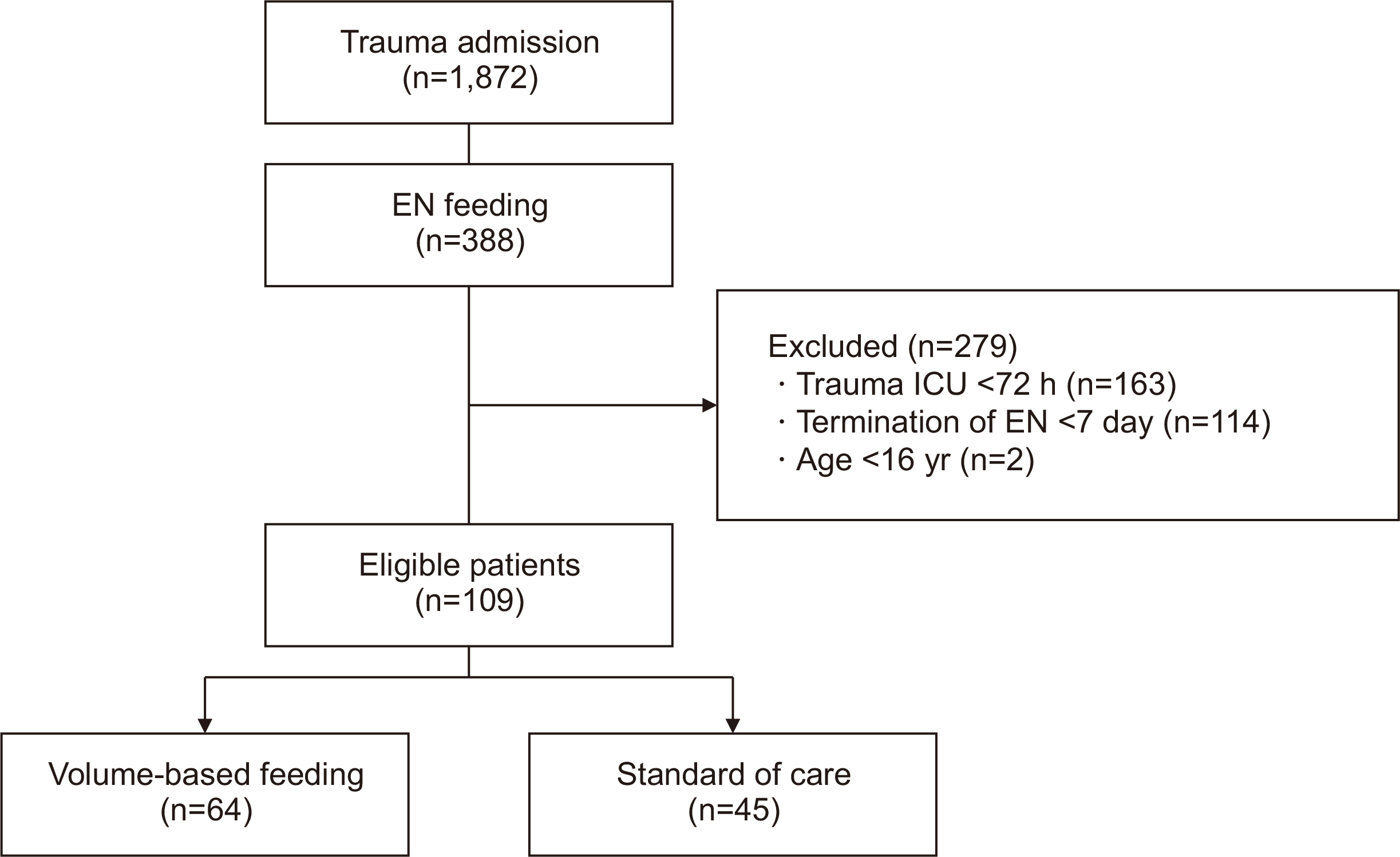
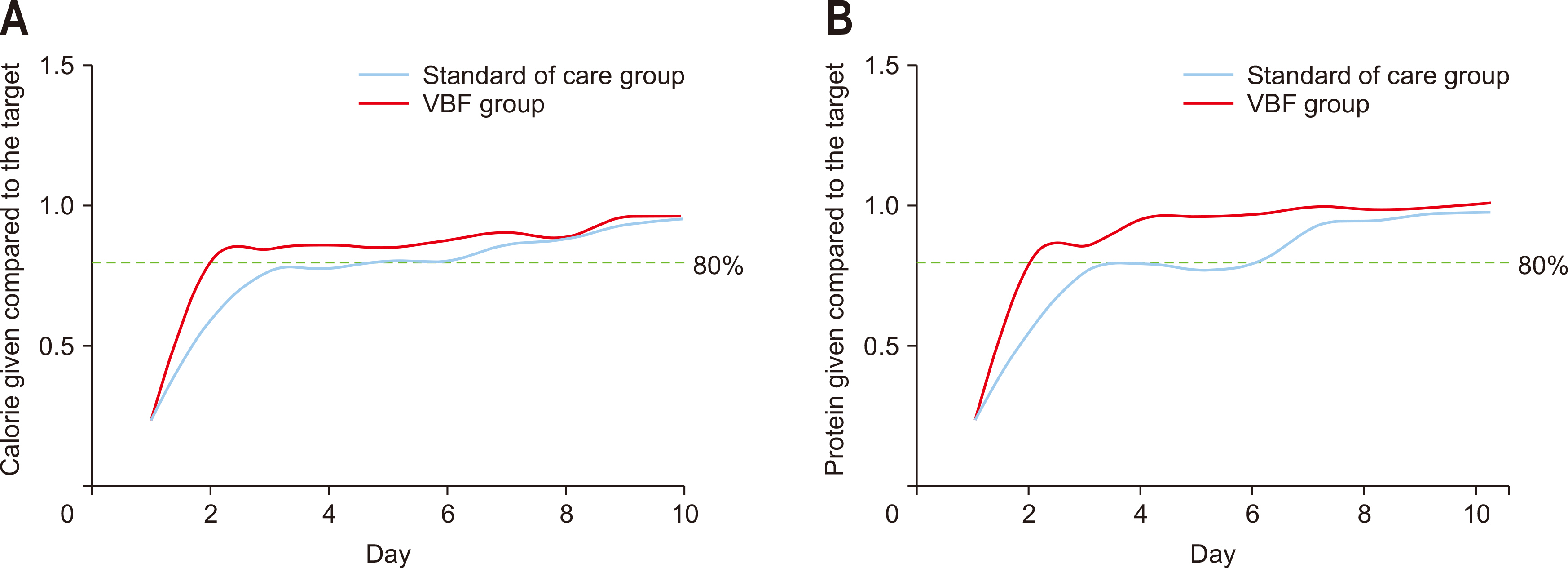
Fig. 1
Volume-based feeding algorithm.
EN = enteral nutrition; TICU = trauma intensive care unit; ICU = intensive care unit; NG = nasogastric; OG = orogastric; CIx. = contraindication; GI = gastrointestinal; Abd. = abdominal; GRV = gastric residual volume; BP = blood pressure; Prox. = proximal; PN = parenteral nutrition; NPO = nil per os; BST = blood sugar test; C. difficile = clostridium difficile.
Fig. 2
Flow diagram for participants.
EN = enteral nutrition; ICU = intensive care unit.
Fig. 3
Daily achievement rate of calorie (A) and protein (B) supply ratio against target.
Fig. 1
Fig. 2
Fig. 3
Comparison of a volume-based feeding protocol with standard feeding for trauma patients in intensive care units in Korea: a retrospective cohort study
Patient demographics and enteral nutrition tolerances
| Variable | VBF (n=64) |
Standard of care (n=45) |
P-value |
|---|---|---|---|
| Age (yr) | 61 (46–72) | 60 (41–69) | 0.52 |
| Sex, male | 56 (87.5) | 34 (75.6) | 0.11 |
| Weight (kg) | 68.1 (54.2–75.4) | 67.1 (56.4–78.5) | 0.76 |
| Body mass index (kg/m2) | 23.7 (20.8–26.1) | 24.6 (22.0–26.0) | 0.64 |
| Injury Severity Score | 33 (23.5–43.0) | 29 (19–43) | 0.30 |
| TRISS | 0.87 (0.66–0.91) | 0.91 (0.68–0.95) | 0.30 |
| Glasgow Coma Scale | 11 (8–14) | 13 (7–15) | 0.43 |
| Mechanism | 0.79 | ||
| Blunt | 59 (92.2) | 45 (100) | |
| Penetration | 1 (1.6) | 0 | |
| Others | 4 (6.3) | 0 | |
| Red blood cell/24 h | 4 (2.0–10.5) | 4 (2.0–12.3) | 0.79 |
| Operation | 49 (76.6) | 36 (80.0) | 0.67 |
| Laparotomy | 11 (17.2) | 7 (15.6) | 0.82 |
| Ileus | 4 (6.3) | 2 (4.4) | >0.99 |
| Vomiting | 4 (6.3) | 3 (6.7) | >0.99 |
| Constipation | 8 (12.5) | 6 (13.3) | 0.90 |
| Diarrhea | 7 (10.9) | 4 (8.9) | >0.99 |
| Abdominal distension | 7 (10.9) | 4 (8.9) | >0.99 |
Values are presented as median (IQR) or number (%).
VBF = volume-based feeding; TRISS = Trauma and Injury Severity Score.
Enteral nutrition status at the end of follow-up
| EN status | VBF (n=64) |
Standard of care (n=45) |
|---|---|---|
| No cessation of EN | 28 (43.8) | 19 (42.2) |
| Transition to oral feeding | 32 (50.0) | 19 (42.2) |
| Deceased | 1 (1.6) | 0 |
| Terminated due to feeding intolerance |
3 (4.7) | 7 (15.6) |
Values are presented as number (%).
EN = enteral nutrition; VBF = volume-based feeding.
Primary and secondary outcomes of patients
| Outcome | VBF (n=64) |
Standard of care (n=45) |
P-value |
|---|---|---|---|
| Primary outcomes | |||
| Mortality | 6 (9.4) | 2 (4.4) | 0.47 |
| ICU LOS (day) | 16.5 (12.0–25.5) | 19 (11–30) | 0.71 |
| Hospital LOS (day) | 31.5 (22.8–46.0) | 39 (20–51) | 0.40 |
| Total ventilator days (day) | 10.5 (6.0–15.5) | 12 (8–22) | 0.28 |
| Sepsis | 6 (9.4) | 2 (4.4) | 0.47 |
| Pneumonia | 25 (39.1) | 16 (35.6) | 0.71 |
| ARDS | 7 (10.9) | 6 (13.3) | 0.70 |
| AKI | 4 (6.3) | 4 (8.9) | 0.72 |
| UTI | 3 (4.7) | 2 (4.4) | >0.99 |
| Delirium | 23 (35.9) | 18 (40.0) | 0.67 |
| Secondary outcomes | |||
| Time to EN initiation (h) | 24.6 (18.7–41.1) | 41.5 (22.0–58.1) | <0.01 |
| Target calorie (kcal/day) | 1,730.5 (1,581–1,860) | 1,725 (1,473–1,905) | 0.49 |
| Target 80% of calories achieved | 59 (92.2) | 37 (82.2) | 0.11 |
| Day on which 80% was achieved (day) | 2 (2–3) | 3 (2–5) | <0.01 |
| Calorie per body weight (kcal/kg/day) | 20.5 (16.0–24.7) | 15.6 (12.8–18.6) | <0.01 |
| Target protein (g/day) | 82 (74.5–88.6) | 77.7 (68.0–87.4) | 0.15 |
| Target 80% of calories achieved | 57 (89.1) | 37 (82.2) | 0.31 |
| Day when 80% protein was achieved (day) | 2 (2–3) | 3 (2–4) | 0.04 |
| Protein per body weight (g/kg/day) | 1.0 (0.8–1.2) | 0.8 (0.6–0.9) | <0.01 |
Values are presented as number (%) or median (IQR).
VBF = volume-based feeding; ICU = intensive care unit; LOS = length of stay; ARDS = acute respiratory distress syndrome; AKI = acute kidney injury; UTI = urinary tract infection; EN = enteral nutrition.
*p<0.05.
Table 1
Patient demographics and enteral nutrition tolerances
Values are presented as median (IQR) or number (%). VBF = volume-based feeding; TRISS = Trauma and Injury Severity Score.
Table 2
Enteral nutrition status at the end of follow-up
Values are presented as number (%). EN = enteral nutrition; VBF = volume-based feeding.
Table 3
Primary and secondary outcomes of patients
Values are presented as number (%) or median (IQR). VBF = volume-based feeding; ICU = intensive care unit; LOS = length of stay; ARDS = acute respiratory distress syndrome; AKI = acute kidney injury; UTI = urinary tract infection; EN = enteral nutrition. *p<0.05.

