 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 15(1); 2023 > Article
- Original article Preoperative consumption of a carbohydrate drink before laparoscopic cholecystectomy is safe and beneficial in Korea: a non-randomized controlled study
-
Yoo Jin Choi1,2
 , Yoonhyeong Byun1,3, Seong Mi Yang4, Ho-Jin Lee4, Hongbeom Kim1,5
, Yoonhyeong Byun1,3, Seong Mi Yang4, Ho-Jin Lee4, Hongbeom Kim1,5 -
Annals of Clinical Nutrition and Metabolism 2023;15(1):15-21.
DOI: https://doi.org/10.15747/ACNM.2023.15.1.15
Published online: April 1, 2023
1Department of Surgery, Seoul National University College of Medicine, Seoul, Korea
2Department of Surgery, Korea University College of Medicine, Seoul, Korea
3Department of Surgery, Uijeongbu Eulji Medical Center, Uijeongbu, Korea
4Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul, Korea
5Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- Corresponding author: Hongbeom Kim, email: hongbeom.kim@samsung.com
• Received: November 11, 2022 • Revised: December 26, 2022 • Accepted: January 11, 2023
© 2023 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 11,027 Views
- 99 Download
- 1 Crossref
Abstract
-
Purpose Overnight fasting prior to elective surgery is the traditional way of avoiding the risk of aspiration during anesthesia induction. However, it causes mental and metabolic stress to patients. Therefore, we investigated the safety and potential benefits of the preoperative consumption of a carbohydrate drink.
-
Methods This was a single-center prospective, nonrandomized study with questionnaire. Patients scheduled for elective laparoscopic cholecystectomy were included. There was no restriction on age, underlying diseases, and biliary drainage prior to surgery. They were preoperatively given either a carbohydrate drink or were instructed to fast from midnight before surgery. Perioperative emotional status was measured using the visual analog scale.
-
Results The 132 patients completed the questionnaire, with 68 receiving the carbohydrate drink and 64 following nil per oral after-midnight instruction. There were no postoperative complications related to preoperative drink consumption or the cholecystectomy procedure itself in both groups. There were no significant differences in all the assessed feelings postoperatively except that preoperative discomforts, such as hunger and thirst, were significantly more alleviated in the group of preoperative consumption of a carbohydrate drink.
-
Conclusion Preoperative consumption of a carbohydrate drink was found to be safe and effective in alleviating preoperative discomfort in elective surgery patients, including older patients and those with underlying comorbidities, who were at greater risk for aspiration. Therefore, we recommend considering preoperative drink consumption as an alternative to traditional overnight fasting in elective surgery patients.
Introduction
Pulmonary aspiration, which causes chemical injury or pneumonitis in the lungs, is considered one of the most fatal complications during induction of general anesthesia [1]. To prevent this complication, most surgeons and anesthesiologists recommend stomach emptying before surgery, and patients are given the common nil per oral (NPO) after midnight instructions the day before the surgery.
However, patients who fast often experience hunger and thirst during the wait time for surgery [2,3]. Moreover, fast-ing induces metabolic stress and insulin resistance, which may increase risk of postoperative complications [4,5]. Therefore, at present, according to the guidelines outlined by the Cochrane Review 2003 [6], American Society of Anesthesiologists (ASA) 2017 [7], and Enhanced Recovery after Surgery (ERAS) [8], preoperative overnight fasting is not recommended and can be shortened to six hours for solids and two hours for liquids. Moreover, preoperative carbohydrate loading, instead of clear water, is recommended before surgery.
However, for most surgeons and anesthesiologists, it is still challenging to disregard this traditional regimen of overnight fasting. Moreover, little consideration is given to the evidence-based guidelines, and NPO after midnight before surgery is still being imposed on surgical patients.
In this study, as medical trends are heading toward implementing ERAS protocol for patients, we aimed to demonstrate that preoperative oral carbohydrate supplements are safe and can improve the quality of life in our patients, who generally have a high risk of pulmonary aspiration.
Methods
This study was approved by the Institutional Review Board of Seoul National University Hospital (approval number: 2007-030-1139). All patients were given written informed consent outlining a full explanation of the procedure in the study.
This was a single-center prospective, non-randomized study with questionnaire. It was described according to the TREND statement (https://www.cdc.gov/trendstatement/index.html).
A total of 170 patients were electively scheduled for laparoscopic or robotic cholecystectomy under general anesthesia from April 2020 to November 2020. Patients who could not comprehend the study protocol or miswrote the questionnaire were excluded. There were no restrictions on age, ASA grade, history of abdominal surgery, and whether percutaneous transhepatic gallbladder drainage (PTGBD) or endoscopic retrograde biliary drainage (ERBD) was inserted before the surgery.
The NPO and carbohydrate drink (CHOd) groups. First, we enrolled only the NPO group, because NPO from midnight was the traditional protocol for preoperative preparation, which requires patients to fast for at least six hours before surgery. After enrolling approximately 60 patients in the NPO group, we consulted with the anesthesiologists to change the traditional protocol to the ERAS protocol. Both departments approved a preoperative carbohydrate drinking protocol as safe as possible according to our hospital circumstances. Then, we enrolled patients in the CHOd group.
The NPO group fasted after midnight before the surgery, following the usual preoperative protocol. The CHOd group was instructed to consume a 200 mL CHOd (NuCARE NO-NPO™: 100 kcal solution containing glucose 25.6 g, sodium 104 mg, and potassium 96 mg; DAESANG Wellife) at least two hours before surgery. For example, if the patients were scheduled for the first operation of the day, which started at 8 AM, or was expected to undergo surgery in the morning, they consumed the drink by 6 AM. If the patients were scheduled for surgery in the afternoon, they consumed the drink by 10 AM.
Second-generation cephalosporin (1g iv) was injected for prophylaxis 30 minutes before the surgical incision. During the laparoscopic cholecystectomy, we used three trocars, which were inserted at the umbilical site (12 mm), epigastric area, and right mid-subclavian line (each 5 mm). We made a single 3 cm incision at the umbilicus for the robotic-assisted cholecystectomy. Gallbladder resection was performed following the usual surgical procedure.
The patients were allowed to drink clear water six hours after surgery and were provided a regular diet the morning after surgery. The patients completed the questionnaire after they were transported to their respective wards from the surgical unit. In addition, postoperative laboratory assessment, such as hemoglobin level, white-blood cell count, platelet level, liver function test, blood urea nitrogen level, and creatinine level, was conducted to examine any postoperative complications. Patients with no postoperative complications were routinely discharged one or two days postoperation.
Before the surgery, patients scored their feelings of anxiety, weakness, hunger, thirst, and discomfort on a scale from 0 to 10 according to the visual analogue scale (VAS) [9] After surgery, patients were asked about nausea and pain in addition to the preoperative questions. The variables of the questionnaire were adapted from previous studies [10,11]. Both groups were asked to answer the questionnaire in the ward immediately before going to the surgical unit so that the two groups were in the same situation, and any feelings they had toward the surgery during that time could be compared with a minimal bias. The questionnaire was translated in English and provided (Supplement 1).
Sample size was not estimated. Participants were recruited from April 2020 to November 2020 till the number of enrolled NPO group reached about 60.
Unit of assignment to study condition is a group of NPO or none. The earlier individuals were assigned to NPO group. There was no matching of the participants for two groups.
There was no blinding to study condition assignment.
The unit of analysis is same to the unit of assignment.
The VAS score, which was a continuous variable, was presented as a mean±standard deviation and compared using an independent t-test. P<0.05 was considered statistically significant. Nominal variables were compared using Pearson’s chi-square and Fisher’s exact test analysis. IBM SPSS Statistics 23.0 (IBM Corp.) software was used for statistical analysis.
Results
Of the 170 patients who underwent elective laparoscopic or robotic cholecystectomy, 132 completed the questionnaire. Among them, 64 and 68 were in the NPO and CHOd groups, respectively (Table 1). Variables in the preoperative demographics were comparable between the two groups, except for the preoperative diagnosis. Overall, the patients were middle-aged (mean, 57.27±12.95 years; range, 24–84 years); 44.7% had comorbidities according to ASA classification, with 31.1% of them diagnosed with critical diseases, such as neurovascular, cardiopulmonary, renal, and hepatic diseases that required surgical interventions. Further, 24.2% had a history of abdominal surgery, which might affect the outcome of cholecystectomy.
Preoperative radiology diagnosis revealed that calculous cholecystitis was the most common case (34.8%), and acute cholecystitis accounted for only 6.8%. For some patients initially diagnosed with acute cholecystitis, biliary drainages were performed before surgery (7.6% PTGBD or ERBD). There was no open conversion case.
Operative data and postoperative complications
Most patients (88.6%) underwent the laparoscopic procedure with three trocar insertion methods (Table 2). According to the intraoperative findings, gallbladder stones and inflammation were observed in 71.2% and 42.4% of the patients, respectively. Patients with severe inflammation had drains inserted (n=26) at the operative site. There were no significant differences in operative data between the two groups.
There were no postoperative complications related to preoperative drink consumption or cholecystectomy procedure itself, such as pulmonary aspiration, pneumonia, vomiting after surgery, bleeding, infection, and bile leakage that could lengthen the patient’s hospital stay. The mean hospital stay was 1.93±1.00 days (data not shown).
Evaluation of perioperative emotional status
Perioperative emotional status was measured using the VAS system (Table 3). In the CHOd group, the preoperative VAS of only hunger and thirst scored significantly lower than that of the NPO group (hunger, P=0.035; thirst, P=0.001) before surgery (Fig. 1).
However, there were no significant differences in all the assessed feelings postoperatively, including postoperative nausea and pain (Fig. 2).
Discussion
In general, with advancements in surgical techniques and perioperative management, clinicians are beginning to focus more on improving the patients’ perioperative quality of life. Since the 1990s, ERAS or “fast-track” programs have been introduced in various surgical fields to ensure early recovery from surgery or improve the catabolic conditions of patients [12,13]. Among the many issues considered in ERAS protocols, reducing perioperative NPO time has been one of the main principles in most surgical fields. Despite considerable efforts, we and many other centers have not adopted these evidence-based suggestions, and still instruct patients to follow the traditional regimen of overnight fasting before elective surgery. However, we believe that the recommendation for overnight fasting should be discontinued.
Since general anesthesia inhibits coughing and airway reflexes, reflux of gastric contents during general anesthesia increases the risk of lung aspiration. Therefore, it is a common practice for many surgeons and anesthesiologists to instruct the patients to fast for six to eight hours before surgery. However, the operation time is not exact for each patient, and if the surgery is delayed, certain patients are required to fast for more than the expected time. These patients are required to endure the inconveniences associated with such a delay, including hunger and thirst, in addition to the fear of the surgery. Furthermore, prolonged fasting may lead to a catabolic reaction that is similar to the condition after trauma. For example, increased insulin resistance or catabolism may increase the risk of postoperative complications [5,14].
Previous studies have demonstrated the usefulness of a preoperative CHOd in various aspects, such as stabilizing the emotional [2,3,10,11] and metabolic [15,16] states of patients. Hausel et al. [2,10] reported that carbohydrate reduces preoperative hunger, thirst, and anxiety. Likewise, the present study revealed that the preoperative consumption of a carbohydrate-containing drink alleviates preoperative hunger and thirst, which are the main factors of discomfort that affect patients immediately before surgery [17].
Although previous studies support the safety and feasibility of preoperative administration of carbohydrate-rich drinks, most of them examined patients with a low aspiration risk. However, since our center is a tertiary hospital, patients tended to be older, had more comorbidities, and had a history of abdominal surgery or inflammation in the gallbladder. Older patients usually have more functional gag reflexes than that in younger patients. In addition, patients who have undergone abdominal surgery or had gallbladder inflammation may cause abnormal bowel motility, increasing the risk of reflux. Thus, we needed to confirm that a preoperative CHOd was also safe in our cohort. However, perioperative complications were not observed, and longer hospital stay was not required for these patients.
We adopted a questionnaire based on the VAS score system since this system is convenient and simple for patients to answer and for physicians to evaluate patients’ symptoms and thoughts. Moreover, it is widely used to evaluate perioperative discomfort variables, such as thirst, hunger, anxiety, nausea, and pain [3,10,18,19].
There were some limitations in this single-center study. First, the time to answer the questionnaire differs between patients. For example, patients who were scheduled for surgery in the afternoon may feel more discomfort than those with a scheduled surgery in the morning. Since the start time of the surgery could not be controlled, it was difficult to tightly control the 2 to 3-hour interval between drinking a carbohydrate solution and the actual time of surgery, which might affect patients’ feelings and the subsequent VAS score. Thus, we requested the patients to provide the time when the questionnaire was completed and excluded those with a response time that deviated too much. Second, we included patients with cholecystitis via a PTGBD insertion. Although there is no data on patients with intraabdominal inflammation for this type of study, preoperative consumption should be avoided in these patients since intraabdominal inflammation negatively affects the bowel. Third, most previous studies provided the patients with 400 mL of CHOd before surgery instead of 200 mL, which was given to the patients in our study. This might affect the results of our study, as the volume of the drink given to the patients may be insufficient to cause any complications. However, we can conclude that consumption of a ≥200 mL CHOd prior to surgery is safe for patients who are older and have comorbidities and inflammation. Lastly, we could not calculate the actual sample size for this study, but extrapolated it from the study of Hausel et al. [2] in 2005. Since the VAS score is used for the ordinal data, there was no information about the true mean and standard deviation from previous studies, but only median value or interquartile range. Thus, future research would be needed with the corrected sample size according to this study.
This study demonstrated that oral liquid consumption of 200 mL is safe and does not cause aspiration during anesthesia induction. It also reduced preoperative discomfort, such as hunger and thirst, thereby increasing patients’ quality of life. Thus, based on the findings of our study and previous studies, we can discontinue the traditional practice of overnight fasting prior to surgery to reduce patients’ perioperative discomfort.
Supplementary materials
Supplementary materials can be found via https://doi.org/10.15747/ACNM.2023.15.1.15.
Supplement 1. Anxiety scale questionnaire for pre/post laparoscopic cholecystectomy.
Acknowledgments
None.
Authors’ contribution
Conceptualization: YJC, HK. Data curation: YB, SMY. Formal analysis: YJC, HJL. Funding acquisition: HK. Methodology: YJC, YB. Supervision: HJL, HK. Validation: SMY. Writing – original draft: YJC. Writing – review & editing: YJC, HK.
Conflict of interest
The authors of this manuscript have no conflicts of interest to declare.
Funding
This study was supported by the 2021 Korean Society of Surgical Metabolism and Nutrition Research Grant.
Data availability
Contact the corresponding author for data availability.
Fig. 1
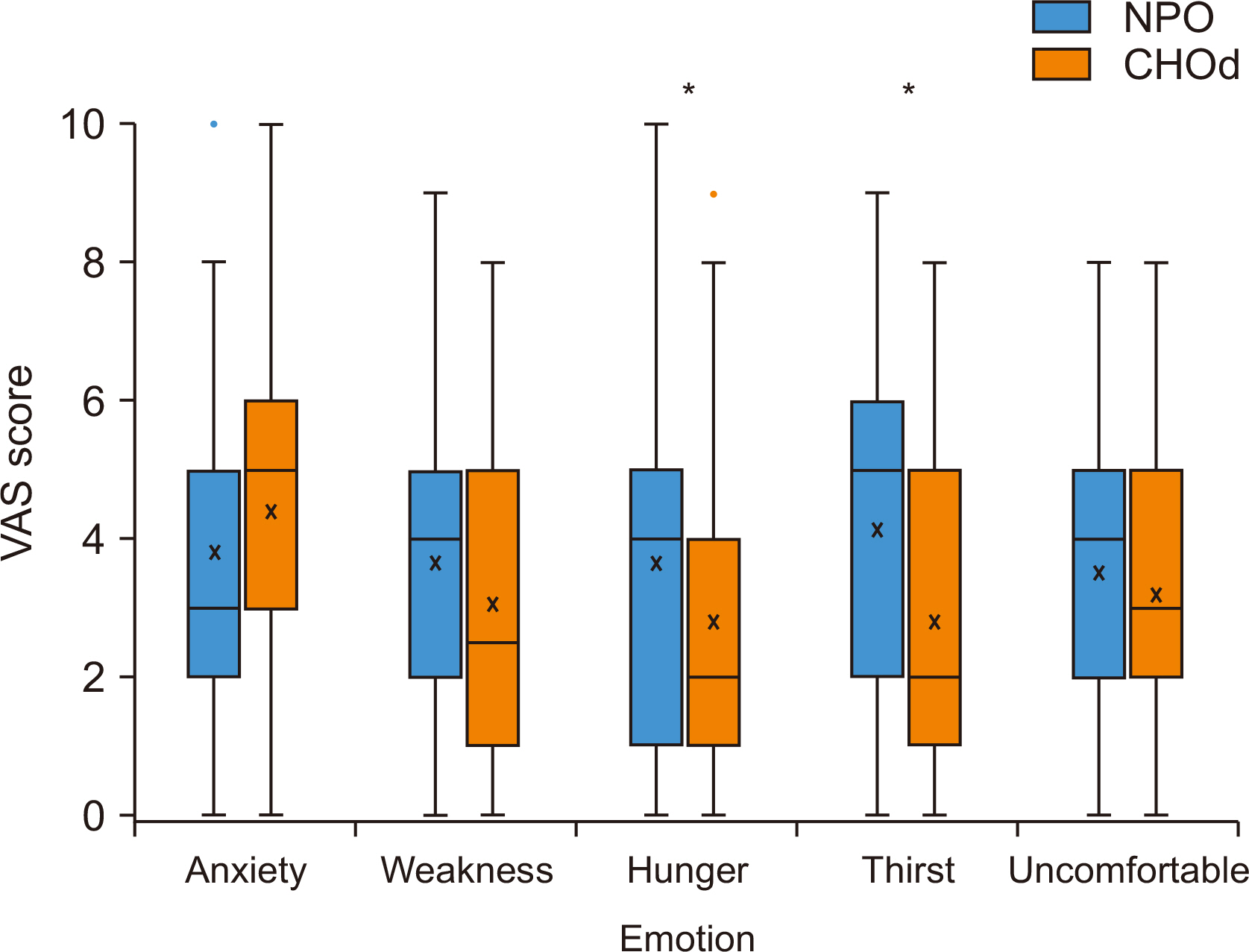
Preoperative emotional status. Comparison of visual analogue scale (VAS) of preoperative emotional states between the nil per oral (NPO) group and carbohydrate drink (CHOd) group.
*P<0.05.
Fig. 2
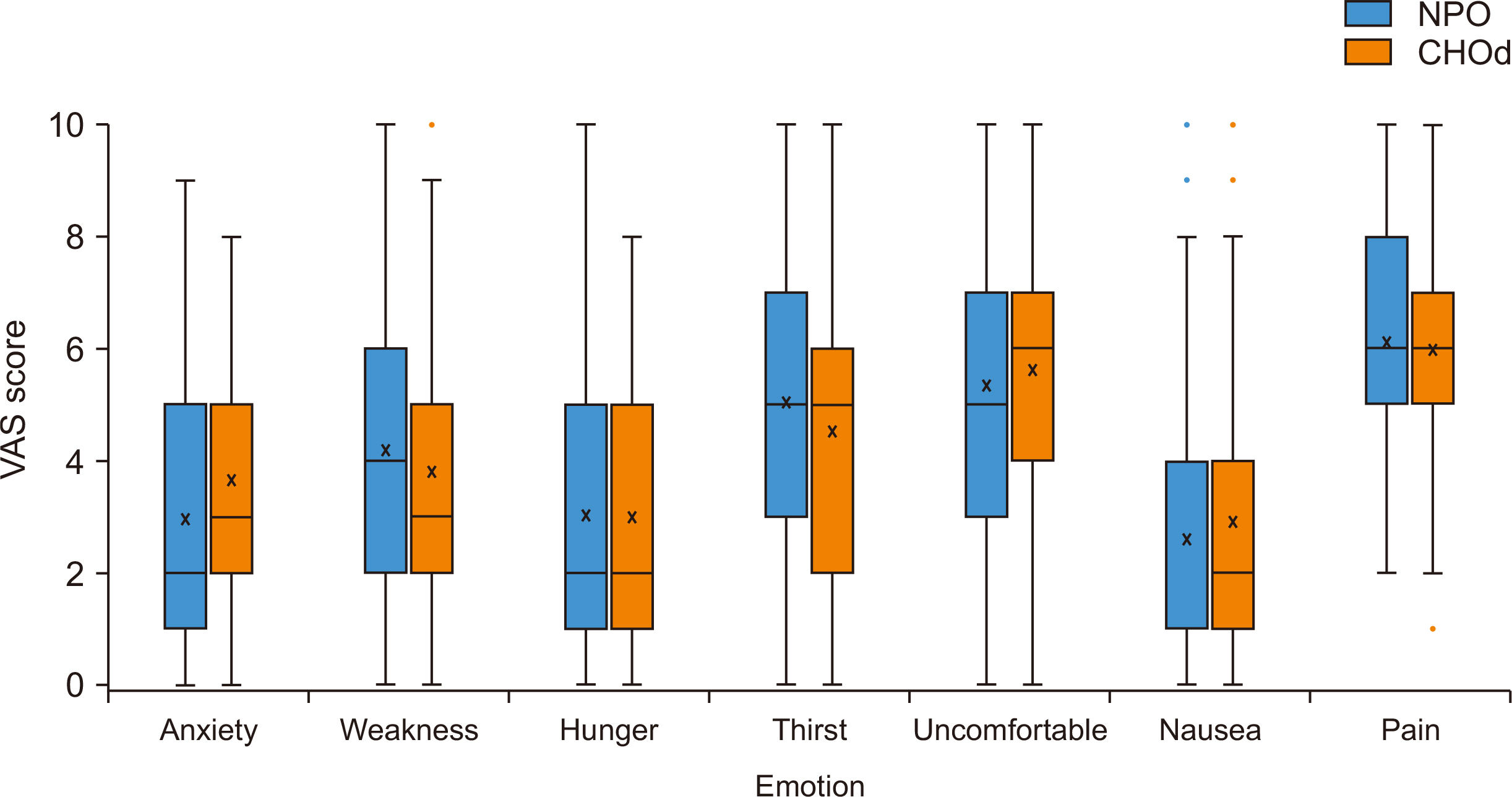
Postoperative emotional status. Comparison of visual analogue scale (VAS) of postoperative emotional states between the nil per oral (NPO) group and carbohydrate drink (CHOd) group.
Table 1
Preoperative demographics
| Variable | Total (n=132) | NPO (n=64) | CHOd (n=68) | P-value |
|---|---|---|---|---|
| Age (yr) | 57.27±12.95 | 58.06±13.89 | 56.61±12.06 | 0.495 |
| Sex, male | 52 (39.4) | 21 (32.8) | 31 (45.6) | 0.133 |
| Body mass index (kg/m2) | 23.97±3.96 | 23.87±3.60 | 24.05±4.29 | 0.795 |
| ASA (≥2) | 59 (44.7) | 23 (35.9) | 35 (51.5) | 0.089 |
| HTN | 36 (27.3) | 18 (28.1) | 18 (26.5) | 0.788 |
| DM | 20 (15.2) | 12 (18.8) | 8 (11.8) | 0.247 |
| Other critical diseasea | 41 (31.1) | 15 (23.4) | 25 (36.8) | 0.108 |
| Cancer | 20 (15.2) | 10 (15.6) | 10 (14.7) | 0.853 |
| Past abdominal operative history | 32 (24.2) | 18 (28.1) | 14 (20.6) | 0.389 |
| Preoperative diagnosis | 0.043 | |||
| GB stone | 42 (31.8) | 19 (29.7) | 23 (33.8) | |
| GB polyp | 24 (18.2) | 13 (20.3) | 11 (16.2) | |
| Chronic cholecystitisb | 11 (8.3) | 2 (3.1) | 9 (13.2) | |
| Calculous cholecystitisb | 46 (34.8) | 28 (43.8) | 18 (26.5) | |
| Acute (calculous) cholecystitis | 9 (6.8) | 2 (3.1) | 7 (10.3) | |
| PTGBD | 10 (7.6) | 4 (6.3) | 6 (8.8) | 0.594 |
| ERBD or PTBD | 10 (7.6) | 6 (9.4) | 4 (5.9) | 0.433 |
Values are presented as mean±standard deviation or number (%).
NPO = nil per oral; CHOd = carbohydrate drink; ASA = American Society of Anesthesiologists; HTN = hypertension; DM = diabetes mellitus; GB = gallbladder; PTGBD = percutaneous transhepatic gallbladder drainage; ERBD=endoscopic retrograde biliary drainage; PTBD = percutaneous transhepatic biliary drainage.
aPatients with neurovascular, cardiopulmonary, renal, and hepatic diseases.
bCalculous cholecystitis and chronic cholecystitis had symptoms related GB.
Table 2
Operative data
Table 3
Preoperative and postoperative emotional status
| Variable |
NPO (n=64) |
CHOd (n=68) |
P-value |
|---|---|---|---|
| Preoperative | |||
| Anxiety | 3.81±2.24 | 4.41±2.33 | 0.134 |
| Weakness | 3.68±2.21 | 3.07±2.22 | 0.118 |
| Hunger | 3.67±2.50 | 2.79±2.20 | 0.035* |
| Thirst | 4.11±2.44 | 2.78±1.97 | 0.001* |
| Uncomfortable | 3.51±2.25 | 3.21±1.86 | 0.302 |
| Postoperative | |||
| Anxiety | 2.97±2.55 | 3.66±2.37 | 0.109 |
| Weakness | 4.19±2.60 | 3.81±2.49 | 0.392 |
| Hunger | 3.03±2.48 | 3.00±2.33 | 0.940 |
| Thirst | 5.05±2.81 | 4.53±2.67 | 0.281 |
| Uncomfortable | 5.33±2.53 | 5.62±2.29 | 0.501 |
| Nausea | 2.61±2.64 | 2.90±2.45 | 0.526 |
| Pain | 6.13±2.22 | 5.99±2.25 | 0.142 |
- 1. Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology 1993;78:56-62. ArticlePubMedPDF
- 2. Hausel J, Nygren J, Thorell A, Lagerkranser M, Ljungqvist O. Randomized clinical trial of the effects of oral preoperative carbohydrates on postoperative nausea and vomiting after laparoscopic cholecystectomy. Br J Surg 2005;92:415-21. ArticlePubMedPDF
- 3. Yildiz H, Gunal SE, Yilmaz G, Yucel S. Oral carbohydrate supplementation reduces preoperative discomfort in laparoscopic cholecystectomy. J Invest Surg 2013;26:89-95. ArticlePubMed
- 4. Svanfeldt M, Thorell A, Hausel J, Soop M, Rooyackers O, Nygren J, et al. Randomized clinical trial of the effect of preoperative oral carbohydrate treatment on postoperative whole-body protein and glucose kinetics. Br J Surg 2007;94:1342-50. ArticlePubMedPDF
- 5. Awad S, Varadhan KK, Ljungqvist O, Lobo DN. A meta-analysis of randomised controlled trials on preoperative oral carbohydrate treatment in elective surgery. Clin Nutr 2013;32:34-44. ArticlePubMed
- 6. Brady M, Kinn S, Stuart P. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst Rev 2003;4:CD004423. Article
- 7. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Task Force on Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration. Anesthesiology 2017;126:376-93. PubMed
- 8. Feldheiser A, Aziz O, Baldini G, Cox BP, Fearon KC, Feldman LS, et al. Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 2: consensus statement for anaesthesia practice. Acta Anaesthesiol Scand 2016;60:289-334. ArticlePubMedPDF
- 9. Kindler CH, Harms C, Amsler F, Ihde-Scholl T, Scheidegger D. The visual analog scale allows effective measurement of preoperative anxiety and detection of patients' anesthetic concerns. Anesth Analg 2000;90:706-12. ArticlePubMed
- 10. Hausel J, Nygren J, Lagerkranser M, Hellström PM, Hammarqvist F, Almström C, et al. A carbohydrate-rich drink reduces preoperative discomfort in elective surgery patients. Anesth Analg 2001;93:1344-50. ArticlePubMed
- 11. Sada F, Krasniqi A, Hamza A, Gecaj-Gashi A, Bicaj B, Kavaja F. A randomized trial of preoperative oral carbohydrates in abdominal surgery. BMC Anesthesiol 2014;14:93.ArticlePubMedPMCPDF
- 12. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth 1997;78:606-17. ArticlePubMed
- 13. Melnyk M, Casey RG, Black P, Koupparis AJ. Enhanced recovery after surgery (ERAS) protocols: time to change practice? Can Urol Assoc J 2011;5:342-8. ArticlePubMedPMC
- 14. Nygren J, Thorell A, Jacobsson H, Larsson S, Schnell PO, Hylén L, et al. Preoperative gastric emptying. Effects of anxiety and oral carbohydrate administration. Ann Surg 1995;222:728-34. ArticlePubMedPMC
- 15. Yuill KA, Richardson RA, Davidson HI, Garden OJ, Parks RW. The administration of an oral carbohydrate-containing fluid prior to major elective upper-gastrointestinal surgery preserves skeletal muscle mass postoperatively--a randomised clinical trial. Clin Nutr 2005;24:32-7. ArticlePubMed
- 16. Can MF, Yagci G, Dag B, Ozturk E, Gorgulu S, Simsek A, et al. Preoperative administration of oral carbohydrate-rich solutions: comparison of glucometabolic responses and tolerability between patients with and without insulin resistance. Nutrition 2009;25:72-7. ArticlePubMed
- 17. Madsen M, Brosnan J, Nagy VT. Perioperative thirst: a patient perspective. J Perianesth Nurs 1998;13:225-8. ArticlePubMed
- 18. Boogaerts JG, Vanacker E, Seidel L, Albert A, Bardiau FM. Assessment of postoperative nausea using a visual analogue scale. Acta Anaesthesiol Scand 2000;44:470-4. ArticlePubMedPDF
- 19. Kindler CH, Harms C, Amsler F, Ihde-Scholl T, Scheidegger D. The visual analog scale allows effective measurement of preoperative anxiety and detection of patients' anesthetic concerns. Anesth Analg 2000;90:706-12. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- MODERN CONCEPT OF POSTOPERATIVE ANALGESIA IN PATIENTS UNDERGOING URGENT LAPAROSCOPIC CHOLECYSTECTOMY
O. PYLYPENKO, O. KRAVETS
Pain anesthesia and intensive care.2024; (4(109)): 55. CrossRef
 Cite
CitePreoperative consumption of a carbohydrate drink before laparoscopic cholecystectomy is safe and beneficial in Korea: a non-randomized controlled study
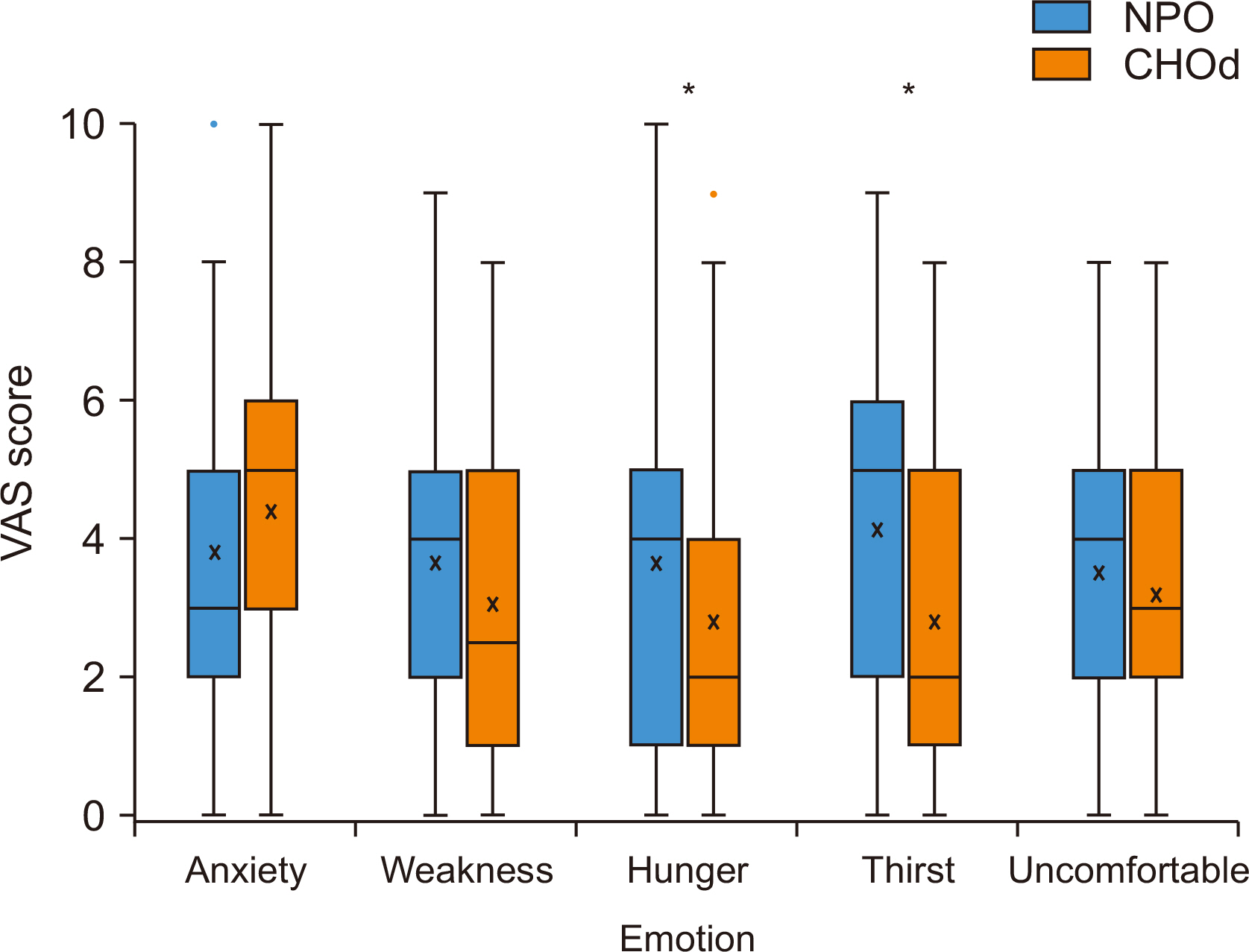
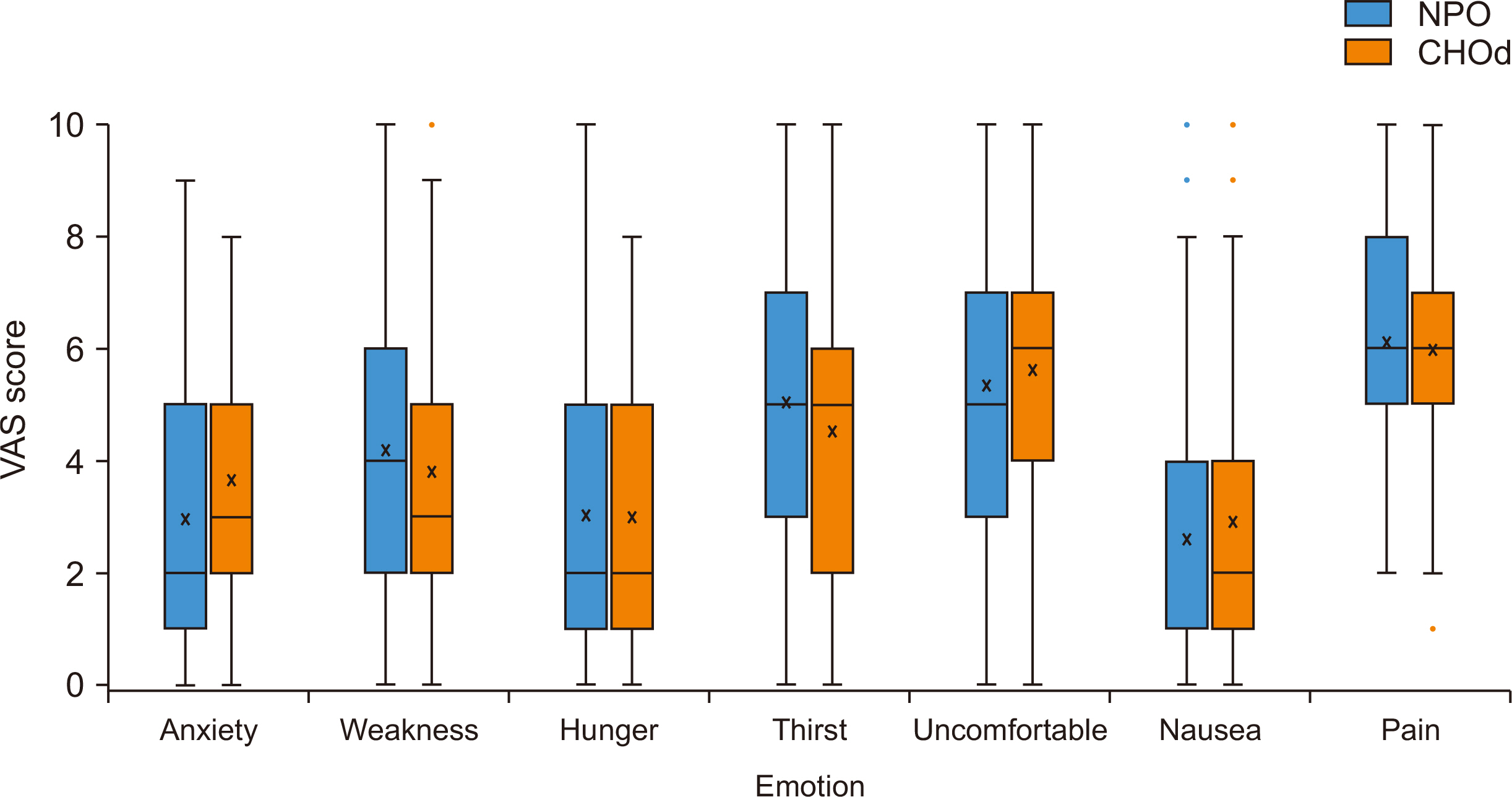
Fig. 1
Preoperative emotional status. Comparison of visual analogue scale (VAS) of preoperative emotional states between the nil per oral (NPO) group and carbohydrate drink (CHOd) group.
*P<0.05.
Fig. 2
Postoperative emotional status. Comparison of visual analogue scale (VAS) of postoperative emotional states between the nil per oral (NPO) group and carbohydrate drink (CHOd) group.
Fig. 1
Fig. 2
Preoperative consumption of a carbohydrate drink before laparoscopic cholecystectomy is safe and beneficial in Korea: a non-randomized controlled study
Preoperative demographics
| Variable | Total (n=132) | NPO (n=64) | CHOd (n=68) | P-value |
|---|---|---|---|---|
| Age (yr) | 57.27±12.95 | 58.06±13.89 | 56.61±12.06 | 0.495 |
| Sex, male | 52 (39.4) | 21 (32.8) | 31 (45.6) | 0.133 |
| Body mass index (kg/m2) | 23.97±3.96 | 23.87±3.60 | 24.05±4.29 | 0.795 |
| ASA (≥2) | 59 (44.7) | 23 (35.9) | 35 (51.5) | 0.089 |
| HTN | 36 (27.3) | 18 (28.1) | 18 (26.5) | 0.788 |
| DM | 20 (15.2) | 12 (18.8) | 8 (11.8) | 0.247 |
| Other critical disease |
41 (31.1) | 15 (23.4) | 25 (36.8) | 0.108 |
| Cancer | 20 (15.2) | 10 (15.6) | 10 (14.7) | 0.853 |
| Past abdominal operative history | 32 (24.2) | 18 (28.1) | 14 (20.6) | 0.389 |
| Preoperative diagnosis | 0.043 | |||
| GB stone | 42 (31.8) | 19 (29.7) | 23 (33.8) | |
| GB polyp | 24 (18.2) | 13 (20.3) | 11 (16.2) | |
| Chronic cholecystitis |
11 (8.3) | 2 (3.1) | 9 (13.2) | |
| Calculous cholecystitis |
46 (34.8) | 28 (43.8) | 18 (26.5) | |
| Acute (calculous) cholecystitis | 9 (6.8) | 2 (3.1) | 7 (10.3) | |
| PTGBD | 10 (7.6) | 4 (6.3) | 6 (8.8) | 0.594 |
| ERBD or PTBD | 10 (7.6) | 6 (9.4) | 4 (5.9) | 0.433 |
Values are presented as mean±standard deviation or number (%).
NPO = nil per oral; CHOd = carbohydrate drink; ASA = American Society of Anesthesiologists; HTN = hypertension; DM = diabetes mellitus; GB = gallbladder; PTGBD = percutaneous transhepatic gallbladder drainage; ERBD=endoscopic retrograde biliary drainage; PTBD = percutaneous transhepatic biliary drainage.
aPatients with neurovascular, cardiopulmonary, renal, and hepatic diseases.
bCalculous cholecystitis and chronic cholecystitis had symptoms related GB.
Operative data
| Variable | NPO (n=64) | CHOd (n=68) | P-value |
|---|---|---|---|
| Laparoscopic/robotic | 59 (92.2)/5 (7.8) | 59 (86.8)/9 (13.2) | 0.327 |
| Gallbladder stones | 45 (70.3) | 49 (72.1) | 0.825 |
| Inflammation (intraoperative) | 28 (43.8) | 28 (41.2) | 0.765 |
| Drain insertion | 9 (14.1) | 17 (25.0) | 0.114 |
Values are presented as number (%).
NPO = nil per oral; CHOd = carbohydrate drink.
Preoperative and postoperative emotional status
| Variable | NPO (n=64) |
CHOd (n=68) |
P-value |
|---|---|---|---|
| Preoperative | |||
| Anxiety | 3.81±2.24 | 4.41±2.33 | 0.134 |
| Weakness | 3.68±2.21 | 3.07±2.22 | 0.118 |
| Hunger | 3.67±2.50 | 2.79±2.20 | 0.035 |
| Thirst | 4.11±2.44 | 2.78±1.97 | 0.001 |
| Uncomfortable | 3.51±2.25 | 3.21±1.86 | 0.302 |
| Postoperative | |||
| Anxiety | 2.97±2.55 | 3.66±2.37 | 0.109 |
| Weakness | 4.19±2.60 | 3.81±2.49 | 0.392 |
| Hunger | 3.03±2.48 | 3.00±2.33 | 0.940 |
| Thirst | 5.05±2.81 | 4.53±2.67 | 0.281 |
| Uncomfortable | 5.33±2.53 | 5.62±2.29 | 0.501 |
| Nausea | 2.61±2.64 | 2.90±2.45 | 0.526 |
| Pain | 6.13±2.22 | 5.99±2.25 | 0.142 |
Values are presented as mean±standard deviation.
Visual analogue scale was used for measurements.
NPO = nil per oral; CHOd = carbohydrate drink.
*P<0.05.
Table 1
Preoperative demographics
Values are presented as mean±standard deviation or number (%). NPO = nil per oral; CHOd = carbohydrate drink; ASA = American Society of Anesthesiologists; HTN = hypertension; DM = diabetes mellitus; GB = gallbladder; PTGBD = percutaneous transhepatic gallbladder drainage; ERBD=endoscopic retrograde biliary drainage; PTBD = percutaneous transhepatic biliary drainage. aPatients with neurovascular, cardiopulmonary, renal, and hepatic diseases. bCalculous cholecystitis and chronic cholecystitis had symptoms related GB.
Table 2
Operative data
Values are presented as number (%). NPO = nil per oral; CHOd = carbohydrate drink.
Table 3
Preoperative and postoperative emotional status
Values are presented as mean±standard deviation. Visual analogue scale was used for measurements. NPO = nil per oral; CHOd = carbohydrate drink. *P<0.05.

