 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 15(3); 2023 > Article
- Review Role of nutrition in wound healing and nutritional recommendations for promotion of wound healing: a narrative review
-
Myoungjean Ju1
 , Yoonhong Kim2, Kyung Won Seo2
, Yoonhong Kim2, Kyung Won Seo2 -
Annals of Clinical Nutrition and Metabolism 2023;15(3):67-71.
DOI: https://doi.org/10.15747/ACNM.2023.15.3.67
Published online: December 1, 2023
1Department of Nursing, Kosin University Gospel Hospital, Busan, Korea
2Department of Surgery, Kosin University Gospel Hospital, Busan, Korea
- Corresponding author: Kyung Won Seo, email: hahachristi@gmail.com
• Received: June 8, 2023 • Revised: September 5, 2023 • Accepted: September 14, 2023
© 2023 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 65,535 Views
- 2,276 Download
- 17 Crossref
Abstract
-
Purpose Addressing both malnutrition and wound healing requires strategic intervention. However, guidelines for adequate nutrition for a variety of wounds are lacking. Based on the latest literature review, we summarize the role of nutrition in each stage of wound healing and nutritional recommendations for wound healing.
-
Current concept Wounds undergo three healing phases inflammatory, proliferative, and remodeling. The inflammatory phase involves clotting and cleaning the wound. The proliferative phase builds the wound bed through tissue growth. In the remodeling phase, collagen strength increases. Proper nutrition is crucial throughout. During inflammation, calcium, vitamin K, A, and E, zinc, and proteins are essential. In proliferation, amino acids, B vitamins, lipids, zinc, and iron play key roles. During remodeling, vitamins C and E, zinc, and water are critical for collagen synthesis and skin cell maturation. Vulnerable groups like the elderly, newborns, and obese patients need proper nutrition for skin maintenance. For pressure ulcers with malnutrition risk, recommendations are 30–35 kcal/kg/day energy, 1.25–1.5 g/kg/day protein, and 30 mL/kg water. Supplements might be added if regular meals don’t meet needs. For diabetic foot ulcers, despite common deficiencies, the 2019 International Working Group on the Diabetic Foot advises against prioritizing nutritional interventions over standard care due to limited high-quality evidence.
-
Conclusion Despite limited guidelines, nutrition assessment is vital for wound evaluation. A multidisciplinary approach is key, emphasizing nutrition’s role in wound healing. Implementing nutritional interventions tailored to the wound and the individual’s nutritional status is essential. This comprehensive strategy ensures the best wound care outcomes.
Introduction
Normal wound healing involves four stages: hemostasis after tissue damage, inflammation, proliferation, and remodeling. If the wound does not heal within a certain period owing to a delay in any stage of the healing process, the wound progresses to a chronic wound [1]. The pathogenesis of chronic wounds differs depending on the characteristics of the wound, but ultimately chronic wounds are caused by the deterioration or deficiency of healing factors that induce normal wound healing mechanisms. Impediments to wound healing include hypoxia, infection, cellular abnormalities, repetitive trauma due to sensory deterioration caused by neuropathies, decreased blood circulation due to pressure, and ischemia. Representative wounds include pressure injuries, diabetic foot ulcers, venous ulcers, and radiation wounds [2].
Pressure injuries are wounds in which tissue is deformed due to pressure generated at bony protrusions or when cellular damage is induced by such deformities. In particular, the sacral bone is bent and sharp; therefore, tissue deformation occurs more severely when pressure is applied in this area. In malnourished patients, the risk of developing pressure ulcers in the sacral region increases because of decreased tissue tolerance and reduced fat and muscle mass [3].
Diabetic foot ulcers are among the most common complications in patients with poorly controlled diabetes. These ulcers usually result from poor blood glucose control, underlying neuropathy, peripheral vascular disease, or poor foot care. Moreover, atherosclerosis accompanies diabetic foot ulcers in these patients; and ulcer healing is delayed due to the lack of blood contact with the wound, leading to necrosis and gangrene. Finally, chronic non-healing wounds lose nutrients through exudates and affect nutritional status because of the metabolic cost of repairing tissue damage [4].
Since chronic wounds significantly influence the metabolic pathway of nutrients, healing is delayed when nutrients are not adequately supplied even if active dressings are applied. In this scenario, simply adding an amino acid or vitamin does not promote wound healing. Moreover, although the relationship between wounds and nutrition has been established in many clinical studies, proper nutritional guidelines for various wounds are lacking. Thus, strategic interventions are required to address both malnutrition and wound healing.
Based on the latest research, we summarize the role of nutrition in each phase of wound healing. We also provide nutritional recommendations for promotion of wound healing.
Role of nutrients in each phase of wound healing
Wounds heal through inflammatory, proliferative, and remodeling phases. During the inflammatory phase, the wound is hemostatic through vasoconstriction and fibrin coagulation. The wound bed is cleaned through the activity of neutrophils and macrophages. In the proliferative phase, a wound bed is built by increasing the number of fibroblasts to form new granulation tissue. The wound bed facilitates wound closure through wound contraction and epithelialization. Finally, in the remodeling phase, collagen is remodeled to increase tensile strength. Surgical wounds may open or healed wounds may recur. Returning tissue to its pre-injury state may require as much as two years [5].
During the wound healing process, overall metabolism increases, increasing demand for calories and proteins. Malnutrition or deficiency in certain nutrients can hinder wound healing through various mechanisms. The roles of nutrients required at each stage of the healing process are shown in Fig. 1 [6].
Calcium and vitamin K are required for the activation of the coagulation process and for fibrin clot formation during inflammation. These two nutrients are also involved in modifying some proteins used in clotting and bone metabolism. Moreover, vitamin A is required for macrophage, monocyte, and fibroblast migration during the early stages of inflammation; and vitamin E is essential for anti-inflammatory action and cell membrane stability. Zinc helps to regulate the immune response [7-11]. Proteins play a role in the immune system and facilitate tissue growth and repair. Specifically, arginine prepares cells for proliferation, and glutamine provides a source of glucose and is necessary for glutathione sulfonate synthesis to reduce oxidative stress [12-14].
Lipids contribute to anti-inflammatory responses, provide energy, and play a role in cell protection [15].
Amino acids are essential during the proliferation phase. Arginine helps regulate collagen deposition, strengthens neovascularization, and aids wound contraction [16,17]. Also, the vitamin B complex plays essential roles in metabolism and promotes cell proliferation. Lipids provide energy for wound healing and proliferation, act as building blocks for epidermal and dermal tissues, and are involved in the synthesis of cell membranes and the composition of the intracellular matrix [8,9]. Zinc is involved in cell proliferation and contributes to wound reconstruction. Iron forms hemoglobin, which is important for tissue perfusion throughout the healing process and aids in collagen synthesis [10,18].
Vitamin C (ascorbic acid) is necessary for collagen synthesis and stabilizes collagen’s triple-helical structure, and vitamin E reduces scarring. Furthermore, zinc is a cofactor in collagen synthesis that aids in collagen maturation. Finally, water is an important factor in wound healing but is often overlooked. Water helps with the movement and maturation of epidermal cells and provides structural elements to the cytoplasm of skin cells [13,19,20].
Nutritional assessment
Various nutrients affect wound healing depending on the wound stage; therefore, having all the necessary nutrients for wound healing at the appropriate time is important. Nutritional factors that increase the risk of developing chronic wounds include decreased body mass index (BMI), being underweight, having changes in the ability to eat independently, decreased food intake, low dietary protein intake, low serum albumin concentration, and decreased total lymphocyte count. Although a causal relationship between malnutrition and wound formation cannot be established, nutritional screening is important for identifying patients at potential risk of nutritional deficiency [21].
The National Institute for Health and Care Excellence (2012) recommends evaluating a patient’s BMI and unintentional weight loss rate and assessing the time frame for decreased nutritional intake and/or potential future nutritional intake disorders as a nutritional screening method. The Mini Nutritional Assessment and Malnutrition Universal Screening Tool is the recommended screening tool [22].
Nutritional assessment during wound healing is necessary to evaluate wound healing stages and nutritional status and to provide appropriate nutrients.
Nutrition guidelines for various wounds
Certain patient groups, such as the elderly, newborns, obese patients, and critically ill patients, are vulnerable to pressure ulcer formation. Generally, appropriate nutrition is necessary for skin maintenance. However, in the case of protein-calorie malnutrition, the skin’s elasticity decreases, often leading to pressure injury. Evidence-based management plans centered on individualized nutritional interventions can prevent skin damage [23].
The 2019 International Clinical Practice Guidelines propose the following nutritional interventions for pressure ulcer risk and pressure ulcer groups (Table 1) [23].
Pressure ulcer risk group with malnutrition risk
∙ Energy: 30–35 kcal/kg/day
∙ Protein: 1.25–1.5 g/kg/day
∙ Water: 30 mL/kg or 1 mL/kcal
∙ If nutritional requirements cannot be met through meals, offer high-calorie, high-protein fortified foods and/or nutritional supplements in addition to the usual diet for adults.
Patients with stage 2 or higher pressure injuries and malnutrition risk or malnutrition
∙ Energy: 30–35 kcal/kg/day
∙ Protein: 1.25–1.5 g/kg/day
∙ Water: 30 mL/kg or 1 mL/kcal
∙ If nutritional requirements cannot be met through meals, offer high-calorie, high-protein nutritional supplements in addition to the usual diet for adults.
∙ Provide high-calorie, high-protein, arginine, zinc, and antioxidant oral nutritional supplements or enteral formulas for adults.
Nutritional deficiencies are common in patients with chronic diabetic foot ulcers, and specific micronutrient deficiencies are common and associated with impaired wound healing and increased amputation risk in diabetic foot ulcer patients [14-16]. Recent studies have found that patients newly diagnosed with diabetes are commonly malnourished, which is associated with impaired wound healing. However, the number of high-quality randomized controlled trials is small, and the evidence on the effects of nutritional interventions in patients with diabetic foot ulcers is uncertain. The IWGDF (International Working Group on the Diabetic Foot) 2019 guidelines [24] are as follows:
Do not use interventions aimed at correcting the nutritional status (including supplementation of protein, vitamins, trace elements, and pharmacotherapy with agents promoting angiogenesis) of patients with diabetic foot ulcers to improve healing, in preference to the best standard of care (GRADE recommendation: Strong; Quality of evidence: Low) [25].
Conclusion
Although nutritional guidelines for each type of wound have been presented along with the importance of nutrition in healing delayed chronic wounds, nutritional evaluation is often overlooked in clinical practice because the focus is on local wound treatments. Furthermore, although detailed guidelines are lacking, nutritional assessment is essential for evaluating wounds. To this end, a multidisciplinary approach is needed to include nutritional assessment in wound evaluation items and to actively perform nutritional interventions according to wound and nutritional status.
Supplementary materials
None.
Acknowledgments
None.
Authors’ contribution
Conceptualization: KWS. Formal analysis: MJ, KWS. Investigation: MJ, YK, KWS. Methodology: MJ, KWS. Project administration: MJ, KWS. Writing – original draft: MJ, KWS. Writing – review & editing: MJ, YK, KWS.
Conflict of interest
Kyung Won Seo is an editorial board member of the journal, but was not involved in the review process of this manuscript. Otherwise, there is no conflict of interest to disclose.
Funding
None.
Data availability
None.
Fig. 1
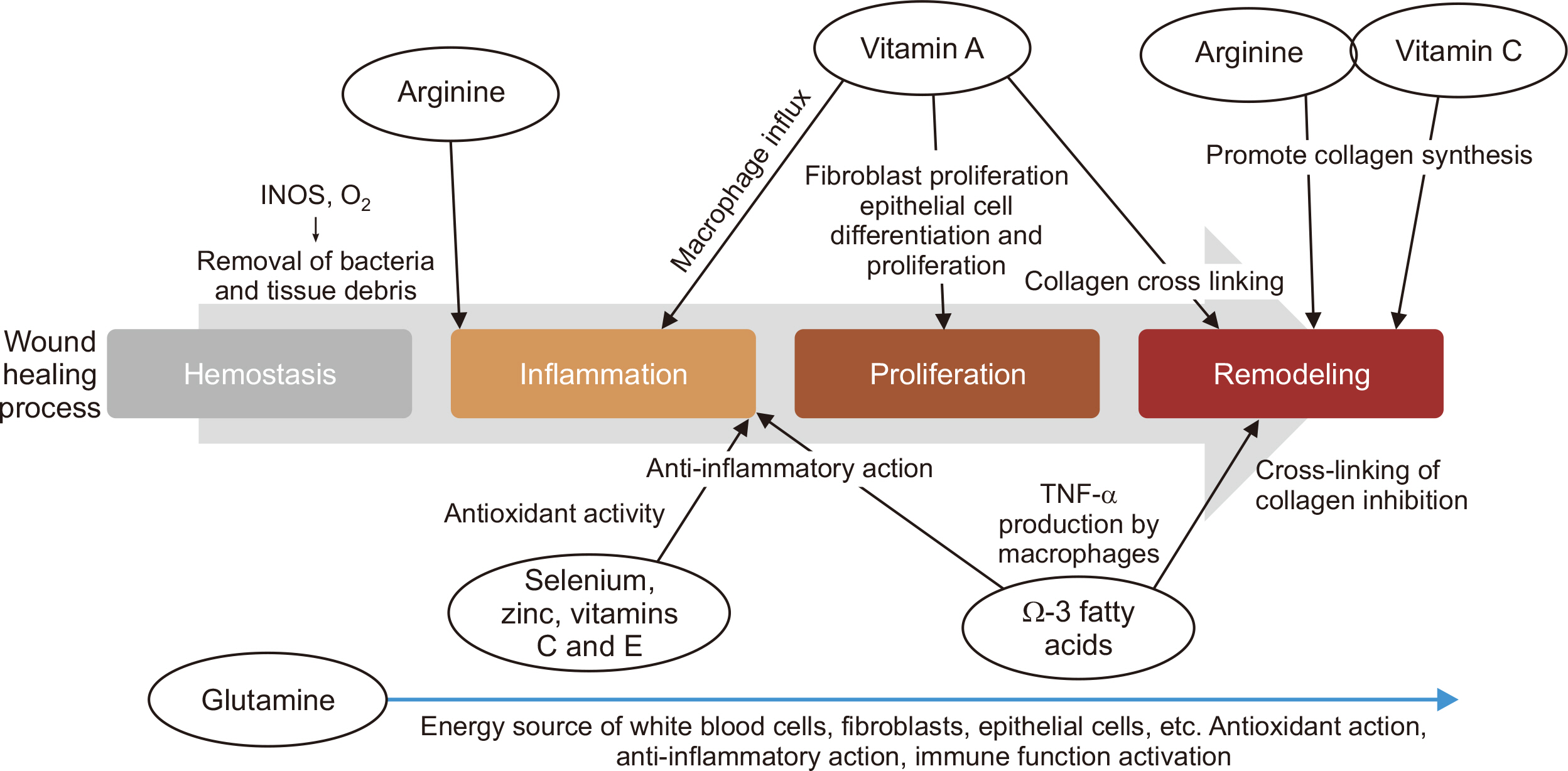
Role of nutrients in the wound healing process. Data from Korean Society of Surgical Metabolism and Nutrition (Clinical metabolism and nutrition for surgical patients; 2016) [6].
Table 1
Suggestion of supplementation regimen for malnourished or at risk of malnutrition
Data from European Pressure Ulcer Advisory Panel, 2019 [23].
- 1. Spear M. Acute or chronic? What's the difference? Plast Surg Nurs 2013;33:98-100. ArticlePubMed
- 2. Rhie JW. Chronic wound. J Korean Med Assoc 2015;58:784-5. Article
- 3. Santamaria N, Creehan S, Fletcher J, Alves P, Gefen A. Preventing pressure injuries in the emergency department: current evidence and practice considerations. Int Wound J 2019;16:746-52. ArticlePubMedPMCPDF
- 4. Choi SW, Seo KB. Treatment of diabetic foot ulcer. J Korean Wound Manag 2014;10:20-2.
- 5. Medlin S. Nutrition for wound healing. Br J Nurs 2012;21:S11-2. S14-5. Article
- 6. Korean Society of Surgical Metabolism and Nutrition. Clinical metabolism and nutrition for surgical patients. Gabon Medical Book; 2016.
- 7. Tsugawa N, Shiraki M. Vitamin K nutrition and bone health. Nutrients 2020;12:1909.ArticlePubMedPMC
- 8. Lansdown AB. Nutrition 2: a vital consideration in the management of skin wounds. Br J Nurs 2004;13:1199-210. ArticlePubMed
- 9. Brown KL, Phillips TJ. Nutrition and wound healing. Clin Dermatol 2010;28:432-9. ArticlePubMed
- 10. Deng L, Du C, Song P, Chen T, Rui S, Armstrong DG, et al. The role of oxidative stress and antioxidants in diabetic wound healing. Oxid Med Cell Longev 2021;2021:8852759. ArticlePubMedPMCPDF
- 11. Demling RH. 2009;Nutrition, anabolism, and the wound healing process: an overview. Eplasty 9:e9. PubMedPMC
- 12. Munoz N, Litchford M, Cereda E. 2022;Nutrition and wound care. Phys Med Rehabil Clin N Am 33:811-22. ArticlePubMed
- 13. Wild T, Rahbarnia A, Kellner M, Sobotka L, Eberlein T. Basics in nutrition and wound healing. Nutrition 2010;26:862-6. ArticlePubMed
- 14. Sherman AR, Barkley M. Nutrition and wound healing. J Wound Care 2011;20:357-8. 360. 362-7. ArticlePubMed
- 15. Grada A, Phillips TJ. Nutrition and cutaneous wound healing. Clin Dermatol 2022;40:103-13. ArticlePubMed
- 16. Langer G, Fink A. Nutritional interventions for preventing and treating pressure ulcers. Cochrane Database Syst Rev 2014;2014:CD003216. ArticlePubMedPMC
- 17. Saeg F, Orazi R, Bowers GM, Janis JE. 2021;Evidence-based nutritional interventions in wound care. Plast Reconstr Surg 148:226-38. ArticlePubMed
- 18. Flanigan KH. Nutritional aspects of wound healing. Adv Wound Care 1997;10:48-52. PubMed
- 19. Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res 2010;89:219-29. ArticlePubMedPMCPDF
- 20. Mukherjee K, Kavalukas SL, Barbul A. Nutritional aspects of gastrointestinal wound healing. Adv Wound Care (New Rochelle) 2016;5:507-15. ArticlePubMedPMC
- 21. Jaffe L, Wu S. The role of nutrition in chronic wound care management: what patients eat affects how they heal. Podiatry Manag 2017;11/12:77-83.
- 22. National Institute for Health and Care Excellence (NICE). Nutrition support in adults (QS24). NICE; 2012.
- 23. European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance. The 2019 international prevention and treatment of pressure ulcers/injuries: clinical practice guideline. EPUAP; 2019.
- 24. Da Porto A, Miranda C, Brosolo G, Zanette G, Michelli A, Ros RD. Nutritional supplementation on wound healing in diabetic foot: what is known and what is new? World J Diabetes 2022;13:940-8. ArticlePubMedPMC
- 25. Rayman G, Vas P, Dhatariya K, Driver V, Hartemann A, Londahl M, et al. 2020;; International Working Group on the Diabetic Foot (IWGDF). Guidelines on use of interventions to enhance healing of chronic foot ulcers in diabetes (IWGDF 2019 update). Diabetes Metab Res Rev 36 Suppl 1:e3283. PubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Assessment of energy requirements in patients with obesity: A narrative review
Cagney Cristancho, Kris M. Mogensen, Malcolm K. Robinson
Nutrition in Clinical Practice.2026; 41(1): 54. CrossRef - Lueyang Black‐Boned Chicken and Black Bean Soup Promoting the Acute Healing of Skin Wounds, Accompanying Special Flavor Substances
Mengya Zhao, Zining Luo, Pengyan Tong, Yining Jia, Xin Yang, Jing Liu, Fangyu Long
Food Chemistry International.2026; 2(1): 46. CrossRef - Zinc supplementation and 60-day mortality in patients receiving total parenteral nutrition: a single-center experience
Mei-Yuan Liu, Chia-Yin Kuo, Hwung-Chung Lee, Jheng-Yan Wu
Frontiers in Nutrition.2026;[Epub] CrossRef - Prevalence of infection in amputations in patients with diabetic foot ulcer: a retrospective study
Kaitlyn Depinet, Bryce Hockman, Rodica Muraru, David A. Ajayi, Zachary Carr, Beth Altenburger, Jaimee Haan, Gregory Westin, Emma Holler, Christopher A. Harle, Mithun Sinha
Frontiers in Clinical Diabetes and Healthcare.2026;[Epub] CrossRef - Efficacy of Oral Cicaglocal for Wound Healing and Pruritus Alleviation in Patients with Epidermolysis Bullosa: A Single-Arm Clinical Trial
Mohammad Mahdi Parvizi, Sara Nayebi, Mohammad Kamali, Sara Ranjbar, Nasrin Saki
Dermatology Practical & Conceptual.2026; 16(2): 6549. CrossRef - Predicting Morbidity in Pancreaticoduodenectomy: A Focus on Nutritional Status
Sadaf Ali, Mohammad Younis Bhat, Mohd Riyaz Lattoo, Akashdeep S Sohi, Ajay Vane
Cureus.2026;[Epub] CrossRef - Electrospun-based nanofibers as ROS-scavenging scaffolds for accelerated wound healing: a narrative review
Mohammad Ebrahim Astaneh, Narges Fereydouni
International Journal of Polymeric Materials and Polymeric Biomaterials.2025; 74(15): 1349. CrossRef - Implementing a screening protocol for food insecure patients within a long‐term acute care hospital (LTACH): A community health needs assessment (CHNA)
Molly MacDonald, Christopher Stimson, Marti Samsel, Tina Gross
Nutrition in Clinical Practice.2025; 40(6): 1598. CrossRef - Nanoformulations Loaded with Phytochemicals for Combating Wound Infections and Promoting Wound Healing: Current Applications and Innovations
Panoraia I. Siafaka, Androulla N. Miliotou, Mehmet Evren Okur, Gökçe Karaotmarlı Güven, Ioannis D. Karantas, Neslihan Üstündağ Okur
Applied Sciences.2025; 15(10): 5413. CrossRef - Combining Topical Oxygen and Negative-Pressure Wound Therapy: New Insights from a Pilot Study on Chronic Wound Treatment
Bartosz Molasy, Mateusz Frydrych, Rafał Kuchciński, Stanisław Głuszek
Journal of Clinical Medicine.2025; 14(15): 5564. CrossRef - Undifferentiated connective tissue dysplasia and skin: what to do? Dietitian’s position
E. A. Nikitina, S. V. Orlova, T. T. Batysheva, N. V. Balashova, M. V. Alekseeva
Medical alphabet.2025; 1(19): 60. CrossRef - Nutritional Immunity in Wound Infection: Unveiling the Role of Dietary Elements in Host–Pathogen Interaction
Chaoming Chen, Xuanfan Hu, Da He, Xuemei He, Lan Shen
Food Science & Nutrition.2025;[Epub] CrossRef - Role of Nutrients and Diet in Wound Healing: The Emerging Paradigm for Effective Therapy
Aishik Banerjee, Arup Ghosh, Subhrajyoty Basu, Soumitra Sahana, Amit Kundu, Sumanta Mondal
Current Indian Science.2025;[Epub] CrossRef - Cancer-Related Malnutrition and Oxidative Stress in Colorectal Cancer Surgery: A Narrative Review of Pathophysiology and Postoperative Outcomes
Andrii Zahorodnii, Alicja Jelska, Paulina Głuszyńska, Hady Razak Hady
Antioxidants.2025; 14(11): 1289. CrossRef - UCI Sports Nutrition Project: The Role of Nutrition in the Prevention and Management of Illnesses and Injuries in Elite Cycling
Patrick B. Wilson, David B. Pyne, Adrian Rotunno
International Journal of Sport Nutrition and Exercise Metabolism.2025; : 1. CrossRef - Clinical Impact of Nutritional Intervention on Pressure Injury Healing in a Paraplegic Patient: A Case Report
Young ran Kim, Mi young Jang, Jun ho Park
Clinical Nutrition Research.2025; 14(4): 241. CrossRef - Impact of Epigenetics, Diet, and Nutrition-Related Pathologies on Wound Healing
John Hajj, Brandon Sizemore, Kanhaiya Singh
International Journal of Molecular Sciences.2024; 25(19): 10474. CrossRef
 Cite
CiteRole of nutrition in wound healing and nutritional recommendations for promotion of wound healing: a narrative review
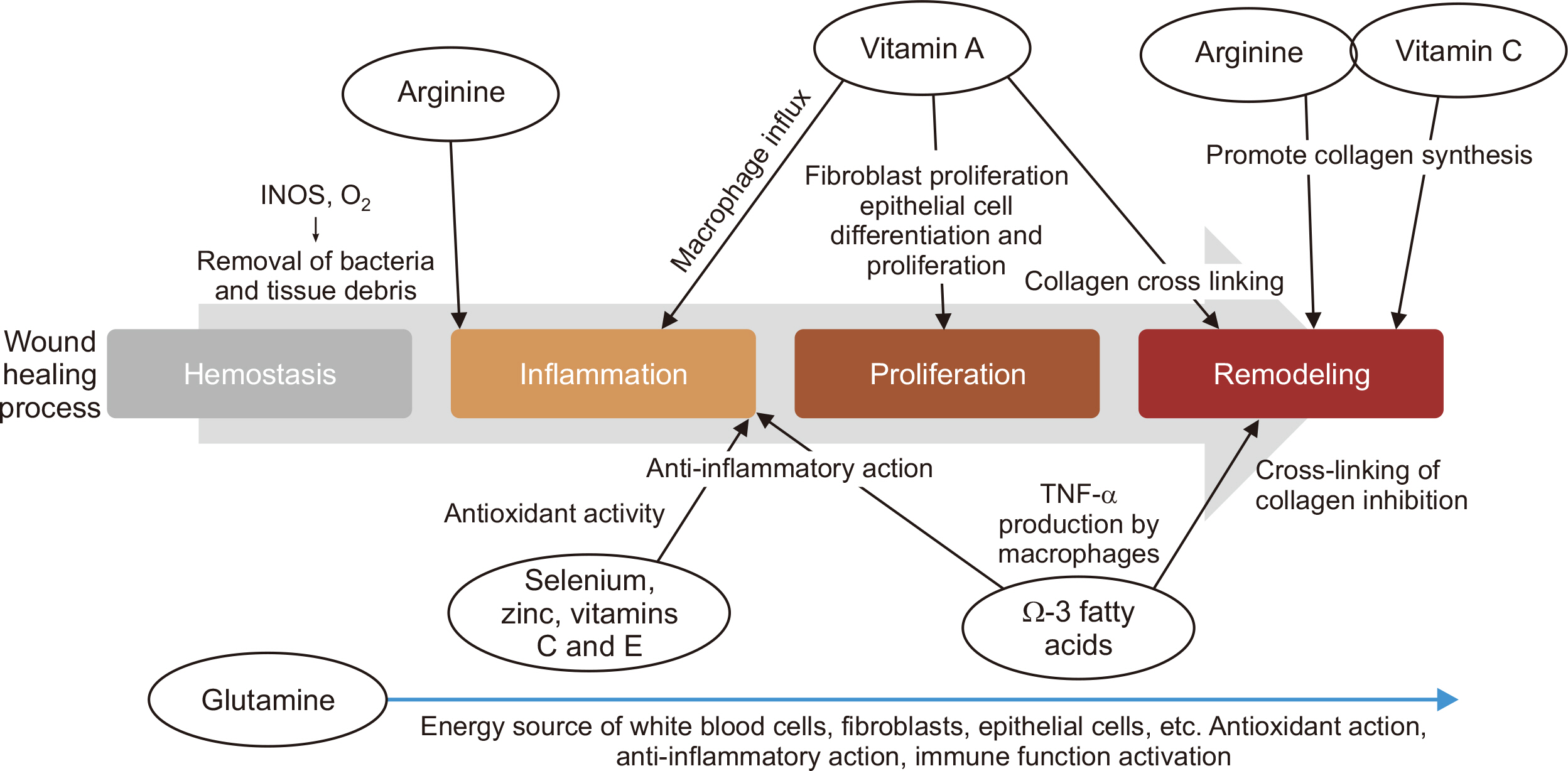
Fig. 1
Role of nutrients in the wound healing process. Data from Korean Society of Surgical Metabolism and Nutrition (Clinical metabolism and nutrition for surgical patients; 2016) [6].
Fig. 1
Role of nutrition in wound healing and nutritional recommendations for promotion of wound healing: a narrative review
Suggestion of supplementation regimen for malnourished or at risk of malnutrition
| Nutrient | Stage I pressure injury | Stage 2 or greater pressure injury |
|---|---|---|
| Calories | 30–35 kcal/kg/day | Over than 30–35 kcal/kg/day |
| Protein | 1.2–1.5 g/kg/day | Over than 1.2–1.5 g/kg/day |
| Additional oral nutritional supplement |
- | Arginine, zinc, antioxidant supplements |
Data from European Pressure Ulcer Advisory Panel, 2019 [
Table 1
Suggestion of supplementation regimen for malnourished or at risk of malnutrition
Data from European Pressure Ulcer Advisory Panel, 2019 [

