 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 17(1); 2025 > Article
- Guideline A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part I. prescribing enteral nutrition orders
-
Ye Rim Chang1
 , Bo-Eun Kim2, In Seok Lee3, Youn Soo Cho4, Sung-Sik Han5, Eunjung Kim6, Hyunjung Kim2, Jae Hak Kim7, Jeong Wook Kim8, Sung Shin Kim9, Eunhee Kong10, Ja Kyung Min11, Chi-Min Park12, Jeongyun Park13, Seungwan Ryu14, Kyung Won Seo15, Jung Mi Song16, Minji Seok17, Eun-Mi Seol18, Jinhee Yoon19, Jeong Meen Seo20, for KSPEN Enteral Nutrition Committee
, Bo-Eun Kim2, In Seok Lee3, Youn Soo Cho4, Sung-Sik Han5, Eunjung Kim6, Hyunjung Kim2, Jae Hak Kim7, Jeong Wook Kim8, Sung Shin Kim9, Eunhee Kong10, Ja Kyung Min11, Chi-Min Park12, Jeongyun Park13, Seungwan Ryu14, Kyung Won Seo15, Jung Mi Song16, Minji Seok17, Eun-Mi Seol18, Jinhee Yoon19, Jeong Meen Seo20, for KSPEN Enteral Nutrition Committee -
Annals of Clinical Nutrition and Metabolism 2025;17(1):3-8.
DOI: https://doi.org/10.15747/ACNM.25.0002
Published online: April 1, 2025
1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
2Department of Dietetics, Samsung Medical Center, Seoul, Korea
3Department of Nutrition, Kyung Hee University Medical Center, Seoul, Korea
4Department of Nutrition Care, Severance Hospital, Yonsei University Health System, Seoul, Korea
5Center for Liver and Pancreatobiliary Cancer, National Cancer Center, Goyang, Korea
6Department of Nutritional Support Team, Seoul National University Hospital, Seoul, Korea
7Department of Internal Medicine, Myongji Hospital, Goyang, Korea
8Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea
9Department of Pediatrics, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
10Department of Family Medicine, Kosin University Gospel Hospital, Busan, Korea
11Graduate School of Nursing Science, Sungkyunkwan University, Seoul, Korea
12Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
13Department of Clinical Nursing, University of Ulsan, Ulsan, Korea
14Department of Surgery, Keimyung University Dongsan Hospital, Daegu, Korea
15Department of Surgery, Kosin University College of Medicine, Busan, Korea
16Nutrition Support Team, Asan Medical Center, Seoul, Korea
17Department of Nursing, Keimyung University Dongsan Medical Center, Daegu, Korea
18Department of Nursing, Seoul National University Hospital, Seoul, Korea
19Department of Home Health Care, Samsung Medical Center, Seoul, Korea
20Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- Corresponding author: Jeong Meen Seo, e-mail: jm0815.seo@samsung.com
• Received: March 4, 2025 • Revised: March 19, 2025 • Accepted: March 28, 2025
© 2025 Korean Society of Surgical Metabolism and Nutrition · Korean Society for Parenteral and Enteral Nutrition · Asian Society of Surgical Metabolism and Nutrition · Japanese Society for Surgical Metabolism and Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 9,323 Views
- 243 Download
- 2 Crossref
This article has been corrected. See "Correction: article type revision" in Volume 17 on page 212.
Abstract
-
Purpose This study aimed to develop a comprehensive practical guide for enteral nutrition (EN) designed to enhance patient safety and reduce complications in Korea. Under the leadership of the Korean Society for Parenteral and Enteral Nutrition (KSPEN), the initiative sought to standardize EN procedures, improve decision-making, and promote effective multidisciplinary communication.
-
Methods The KSPEN EN committee identified key questions related to EN practices and organized them into seven sections such as prescribing, delivery route selection, formula preparation, administration, and quality management. Twenty-one experts, selected based on their expertise, conducted a thorough literature review to formulate evidence-based recommendations. Drafts underwent peer review both within and across disciplines, with final revisions completed by the KSPEN Guideline Committee. The guide, which will be published in three installments, addresses critical elements of EN therapy and safety protocols.
-
Results The practical guide recommends that EN orders include detailed elements and advocates the use of electronic medical records for communication. Standardized prescription forms and supplementary safety measures are outlined. Review frequency is adjusted according to patient condition—daily for critically ill or unstable patients and as dictated by institutional protocols for stable patients. Evidence indicates that adherence to these protocols reduces mortality, complications, and prescription errors.
-
Conclusion The KSPEN practical guide offers a robust framework for the safe delivery of EN tailored to Korea’s healthcare context. It emphasizes standardized protocols and interdisciplinary collaboration to improve nutritional outcomes, patient safety, and operational efficiency. Rigorous implementation and monitoring of adherence are critical for its success.
Introduction
To reduce complications and improve patient safety in enteral nutrition (EN), it is essential to establish and adhere to policies and standardized procedures for routine practices and decision-making throughout the EN process. Effective communication among all members of the multidisciplinary team is also crucial. An interdisciplinary group from the Korean Society for Parenteral and Enteral Nutrition (KSPEN) has developed a practice guide that is essential for healthcare professionals in ensuring the safe delivery of EN, taking into account the domestic realities of EN administration in Korea.
Methodology
To develop this document, the KSPEN EN committee first identified key questions related to EN and subsequently categorized them into relevant sections, including prescribing EN orders, selecting the delivery route and initiating EN, preparing EN formulas, general administration, safe use of EN delivery systems, medication administration, and quality management.
Twenty-one experts were assigned to address these key questions based on their expertise and experience. Following a comprehensive literature review, evidence-based practice recommendations were formulated along with rationales supported by relevant references. Draft recommendations for each key question underwent peer review within the same professional discipline and cross-review by experts from other disciplines. Finally, the KSPEN Guideline Committee conducted an additional review to finalize the Practice Guide for EN. This guide will be published in seven installments.
Practice guide
Practice recommendation
• The following elements should be included in EN orders:
1. Indications and rationale for enteral feeding
2. Enteral feeding formula name (generic name, e.g., high-protein standard formula, or product name), concentration (kcal/mL), caloric value, and category of EN formula
3. Reasons for recommending or changing a specific formula
4. Tube information, including the delivery route (e.g., nasogastric tube, nasojejunal tube, gastrostomy tube, or jejunostomy tube)
5. Single dose volume (mL) or total daily volume (mL)
6. Administration method (e.g., continuous infusion, intermittent infusion, or bolus feeding)
7. Feeding rate, including initial rate, target rate, and progression schedule
8. Flush volume and schedule
9. Daily target or provided nutrient intake
- Mandatory: total volume, energy, protein, and fluid intake
- Optional: energy per body weight (kcal/kg), carbohydrate (g), and protein (g)
10. Monitoring parameters
- Adverse effects: refeeding syndrome, gastrointestinal complications, improper tube placement (to be monitored as early as possible)
- Trends in blood tests
- Trends in anthropometric measurements
- Tolerance to enteral feeding: symptoms such as abdominal distension, vomiting, diarrhea, and constipation
• Additional infusion protocols should be provided (e.g., patient positioning, oral care, conditions requiring discontinuation of feeding).
• Electronic medical records should be used to communicate and document responses and progress by the multidisciplinary team managing enteral-fed patients.
Rationale
Even among critically ill patients with a lower tolerance for enteral feeding, significant reductions in mortality [1], a decreased incidence of complications such as diarrhea, and improved early initiation with appropriate calorie delivery have been reported [2]. The implementation of an enteral feeding protocol in the intensive care unit resulted in a shorter time to initiate feeding, a higher rate of achieving target nutritional intake [3], and decreased reliance on parenteral nutrition [1]. Additionally, incorporating nutrition assessment findings into nutritional support recommendations [4] led to increased energy and protein intake, shorter hospital stays, and improvements in serum albumin levels and body weight [5]. The integration of nutrition assessments and prescription recommendations via electronic medical records has been reported to facilitate efficient communication among healthcare professionals and specialists, thereby contributing to improved nutritional status, better maintenance of electrolyte balance and optimal blood glucose levels, reduced medical costs, and fewer prescription errors [6].
Practice recommendation
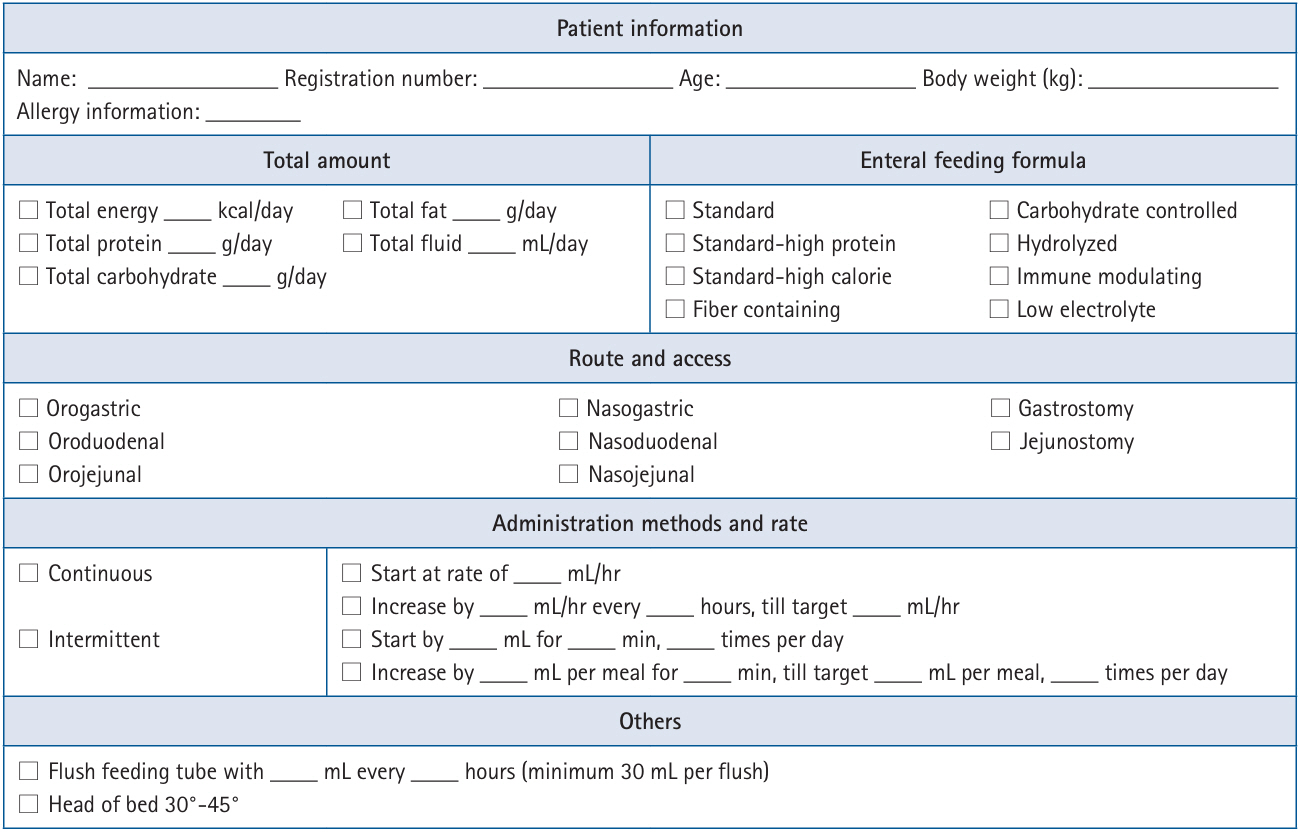
• Standardized enteral feeding prescription form
A standardized enteral feeding prescription form should include the following essential components (Figs. 1, 2):
1. Patient information
- Name and registration number
- Height and weight
- Specific considerations such as allergies that must be taken into account for enteral feeding administration
2. Total amount
- Total energy ______ kcal/day
- Total protein ______ g/day
- Total carbohydrate ______ g/day
- Total fat ______ g/day
- Total fluid ______ mL/day
3. Enteral feeding formula
- Name of the enteral feeding formula (e.g., high-protein standard) or product name
- For pediatric patients, the concentration (kcal/mL) should be specified
4. Administration route and enteral access device
- Administration route (e.g., nasogastric, gastrostomy, nasojejunal, or jejunostomy)
5. Administration method and rate
- Method of administration (e.g., continuous infusion or intermittent feeding)
- Volume and rate of administration
- Guidelines for dose escalation and progression of nutritional support
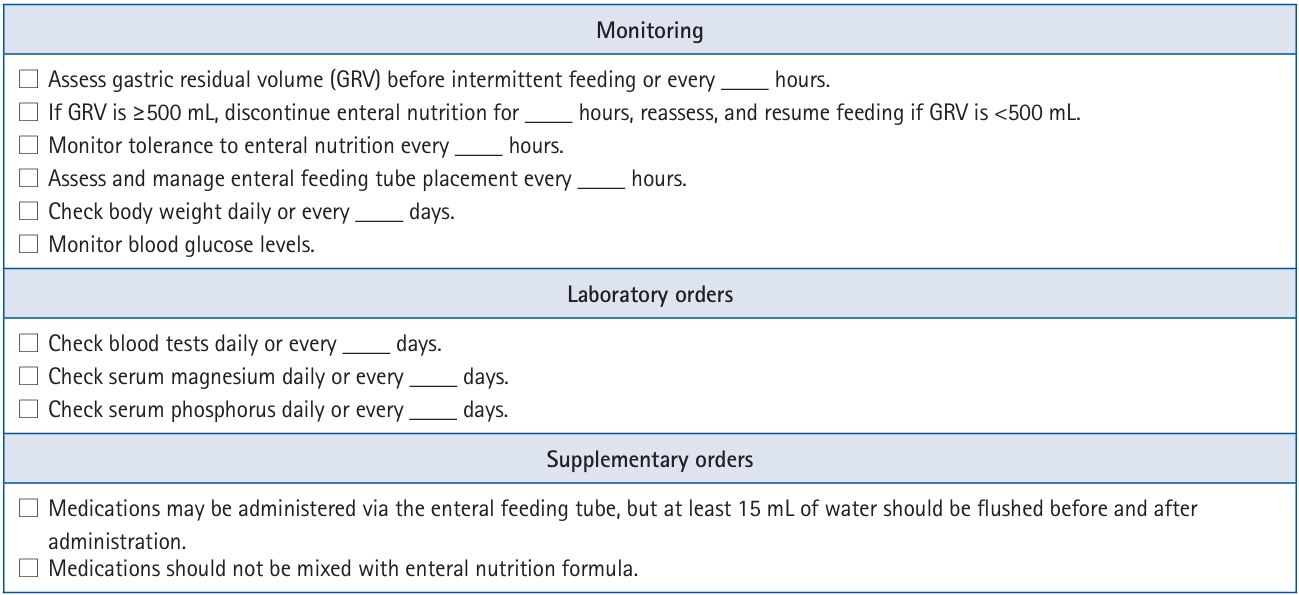
• Supplementary items for patient safety
To improve patient safety, guidelines and procedures should be established to integrate the following enteral feeding prescription directives within the ordering communication system:
1. Confirmation of tube placement via radiography at the initiation of EN (except in neonates and pediatric patients with multiple inserted tubes to minimize radiation exposure)
2. Establishment of standardized methods for enteral tube flushing
3. Monitoring the appropriateness of bed elevation and EN tolerance
4. Management and evaluation of enteral access devices based on infection control guidelines
5. Monitoring parameters: biochemical test results, intake and output measurements, weight and physical examination, gastrointestinal tolerance
6. Specification of product type, prescribed amount, and administration schedule when using calorie- or nutrition-dense food products
• Consultation with the nutrition support team
Collaboration with the nutrition support team or the clinical nutrition department should be sought when necessary.
Rationale
A clear protocol outlining the essential components of an enteral feeding prescription ensures that patients receive the appropriate formula via the correct route in a timely manner. Healthcare providers should document these essential components in electronic medical records (Fig. 1). A prospective study evaluating the implementation of an ordering communication system demonstrated a significant reduction in prescription error rates after its adoption [7].
The use of enteral feeding protocols improves the delivery of energy, protein, and fluids in critically ill patients—who may experience interruptions in EN due to procedures such as intubation, extubation, gastrointestinal interventions, or imaging studies [8,9]. The nutrition support team or clinical nutrition department should determine which enteral feeding protocol is most suitable for each patient and how to effectively implement the prescription process.
Supplementary prescription orders (Fig. 2) help ensure adequate energy and protein intake, maintain patient safety, and assist healthcare providers in monitoring EN therapy. Although not mandatory, these supplementary orders enhance the clarity and accuracy of EN prescriptions.
Practice recommendation
• The frequency of reviewing EN prescriptions should be determined based on the EN protocol of each healthcare institution.
• Every time the EN prescription is modified or re-prescribed, all items included in the prescription should be re-evaluated.
• Critically ill patients, postoperative patients, patients with poor blood sugar control, patients with unstable fluid and electrolyte status, high-risk patients with refeeding syndrome, and neonatal and pediatric intensive care patients should be monitored daily, and their EN prescriptions should be reviewed [10].
• For stable hospitalized patients, those in long-term care facilities, and home care patients, the monitoring and EN prescription review frequency should be determined according to the protocol of each healthcare institution [11,12].
Rationale
Regular review and monitoring of EN prescriptions allow early identification of clinical and metabolic complications and ensure that nutritional support is provided safely. Each healthcare institution should establish protocols for the review and renewal frequency of EN prescriptions, involving nutrition support specialists from various fields. Additionally, institutions should monitor adherence to these protocols to ensure patient safety and evaluate the effectiveness of nutritional interventions.
Authors’ contribution
Conceptualization: all authors. Data curation: all authors. Formal analysis: all authors. Methodology: all authors. Project administration: all authors. Visualization: all authors. Funding acquisition: Not applicable. Writing – original draft: all authors. Writing – review & editing: all authors. All authors read and approved the final manuscript.
Conflict of interest
Ye Rim Chang has served as the editor of the Annals of Clinical Nutrition and Metabolism since 2024. However, she was not involved in the peer review process or decision-making regarding publication. Otherwise, no potential conflict of interest relevant to this article was reported.
Funding
None.
Data availability
Not applicable.
Acknowledgments
We would like to express our sincere gratitude to the Korean Society for Parenteral and Enteral Nutrition (KSPEN) Guideline Committee members—In Gyu Kwon (Department of Surgery, Yonsei University Gangnam Severance Hospital, Seoul, Korea), Mina Kim (Department of Nursing, Inha University Hospital, Incheon, Korea), Bomi Kim (Department of Pharmacy, Seoul National University Hospital, Seoul, Korea), Seong Eun Kim (Department of Internal Medicine, Ewha Womans University Mokdong Hospital, Seoul, Korea), Jiyeon Kim (Department of Clinical Nutrition, National Cancer Center, Goyang, Korea), Ye Won Sung (Department of Pharmacy, Chungnam National University Hospital, Daejeon, Korea), Junghyun Yu (Nutritional Support Team, Yongin Severance Hospital, Yongin, Korea), Seung Hwan Lee (Department of Traumatology, Gachon University College of Medicine, Incheon, Korea), Jae Gil Lee (Department of Surgery, Ewha Womans University Mokdong Hospital, Seoul, Korea), Jee Young Lee (Department of Nursing, Kosin University Gospel Hospital, Busan, Korea), A Young Lim (Department of Clinical Nutrition, Seoul National University Bundang Hospital, Seongnam, Korea), Ji Yoon Cho (Department of Pharmacy, Daegu Fatima Hospital, Daegu, Korea)—for their invaluable contributions in reviewing and updating this practical guide for enteral nutrition.
Supplementary materials
None.
Correction
This article was corrected on November 13, 2025, to revise the article type.
- 1. Padar M, Uusvel G, Starkopf L, Starkopf J, Reintam Blaser A. Implementation of enteral feeding protocol in an intensive care unit: before-and-after study. World J Crit Care Med 2017;6:56-64. ArticlePubMedPMC
- 2. Kim SH, Park CM, Seo JM, Choi M, Lee DS, Chang DK, et al. The impact of implementation of an enteral feeding protocol on the improvement of enteral nutrition in critically ill adults. Asia Pac J Clin Nutr 2017;26:27-35. PubMed
- 3. Heyland DK, Cahill NE, Dhaliwal R, Sun X, Day AG, McClave SA. Impact of enteral feeding protocols on enteral nutrition delivery: results of a multicenter observational study. JPEN J Parenter Enteral Nutr 2010;34:675-84. PubMed
- 4. Roberts SR. Improving patient outcomes through registered dietitian order writing. Nutr Clin Pract 2013;28:556-65. ArticlePubMedPDF
- 5. Braga JM, Hunt A, Pope J, Molaison E. Implementation of dietitian recommendations for enteral nutrition results in improved outcomes. J Am Diet Assoc 2006;106:281-4. ArticlePubMed
- 6. Vanek VW. Providing nutrition support in the electronic health record era: the good, the bad, and the ugly. Nutr Clin Pract 2012;27:718-37. PubMed
- 7. Armada ER, Villamanan E, Lopez-de-Sa E, Rosillo S, Rey-Blas JR, Testillano ML, et al. Computerized physician order entry in the cardiac intensive care unit: effects on prescription errors and workflow conditions. J Crit Care 2014;29:188-93. ArticlePubMed
- 8. Heyland DK, Dhaliwal R, Lemieux M, Wang M, Day AG. Implementing the PEP uP protocol in critical care units in Canada: results of a multicenter, quality improvement study. JPEN J Parenter Enteral Nutr 2015;39:698-706. PubMed
- 9. Taylor B, Brody R, Denmark R, Southard R, Byham-Gray L. Improving enteral delivery through the adoption of the “Feed Early Enteral Diet adequately for Maximum Effect (FEED ME)” protocol in a surgical trauma ICU: a quality improvement review. Nutr Clin Pract 2014;29:639-48. PubMed
- 10. McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2016;40:159-211. PubMed
- 11. NSW Agency for Clinical Innovation. Guidelines for home enteral nutrition (HEN) services. 2nd ed. Agency for Clinical Innovation; 2012.
- 12. Bischoff SC, Austin P, Boeykens K, Chourdakis M, Cuerda C, Jonkers-Schuitema C, et al. ESPEN guideline on home enteral nutrition. Clin Nutr 2020;39:5-22. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Rationale for Determining Energy Requirement in Hospitalized Patients: A Narrative Review
Suk-Kyung Hong, Kyung Mo Kim
Pediatric Gastroenterology, Hepatology & Nutrition.2026; 29(3): 212. CrossRef - Bridging evidence and clinical practice: a practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition
Suk-Kyung Hong
Ann Clin Nutr Metab.2025; 17(1): 1. CrossRef
 Cite
Cite- Figure
-
- Related articles
-
- Nutritional support for critically ill patients by the Korean Society for Parenteral and Enteral Nutrition—part II: a clinical practice guideline
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part III. preparation of enteral nutrition formulas
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part II. selection and initiation of enteral feeding routes
- Bridging evidence and clinical practice: a practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition
- Nutritional support for critically ill patients by the Korean Society for Parenteral and Enteral Nutrition — part I: a clinical practice guideline
A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part I. prescribing enteral nutrition orders
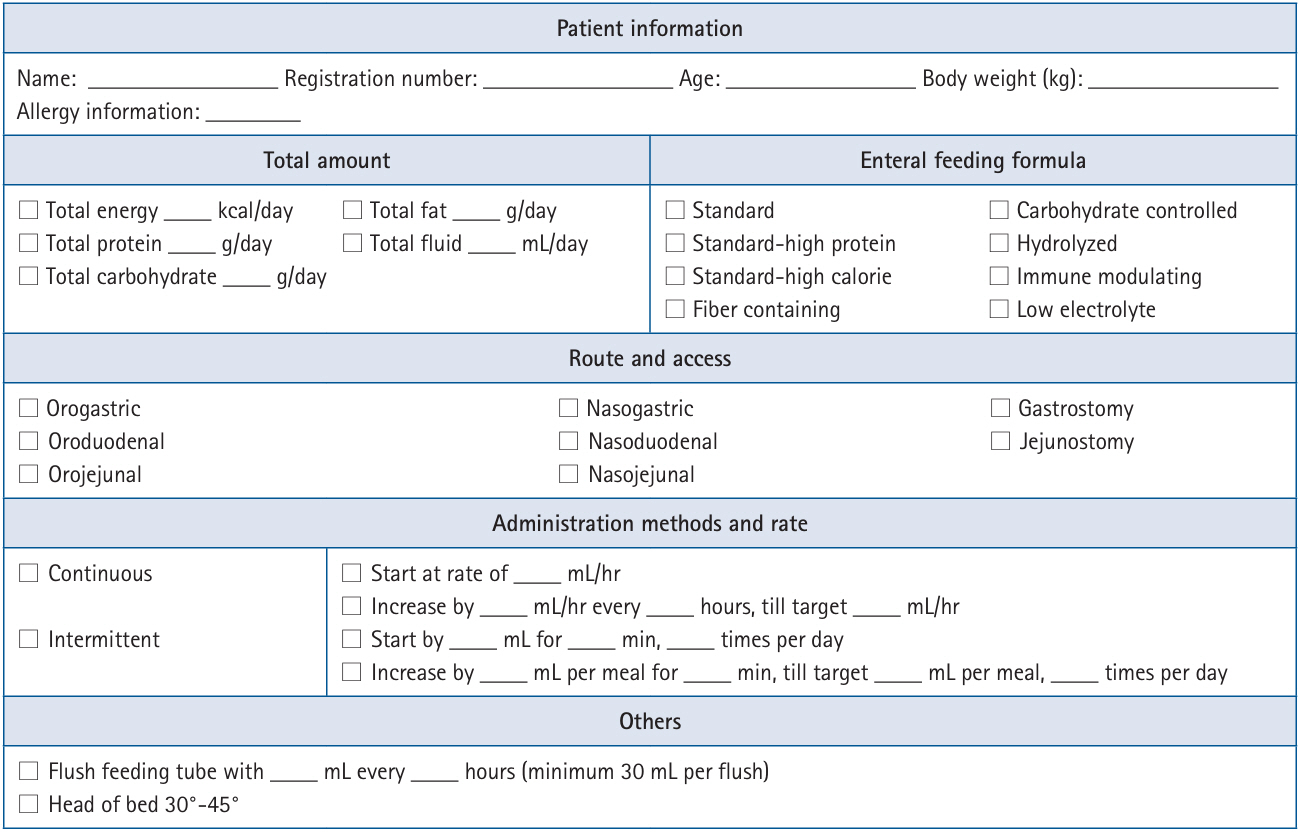
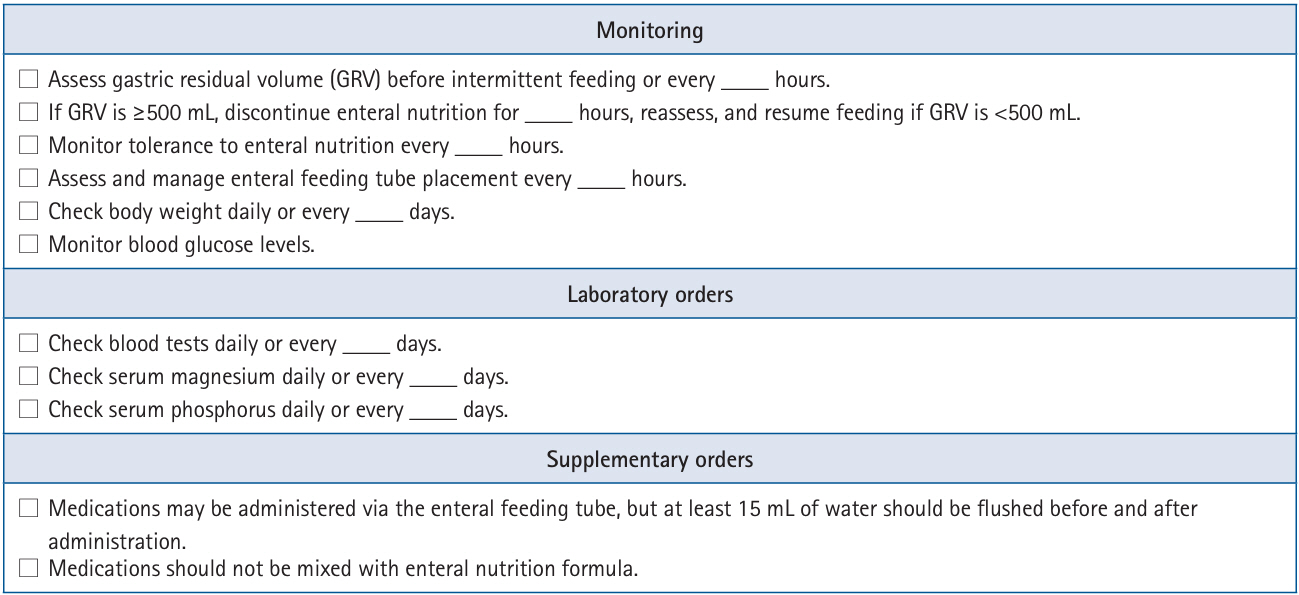
Fig. 1. Example of an enteral feeding prescription protocol.
Fig. 2. Example of supplementary orders.
Fig. 1.
Fig. 2.
A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part I. prescribing enteral nutrition orders

