 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 18(1); 2026 > Article
- Review Bedside support for neurologically impaired patients via nutritional evaluations, swallowing function assessments, and gastrointestinal function tests: a narrative review
-
Daisuke Masui
 , Naoki Hashizume, Yoshinori Koga, Hiroto Eto, Hiroki Yoshida, Shotaro Taki, Takato Aikoh, Shiori Tsuruhisa, Tomohiro Kurahachi, Naruki Higashidate, Tatsuru Kaji
, Naoki Hashizume, Yoshinori Koga, Hiroto Eto, Hiroki Yoshida, Shotaro Taki, Takato Aikoh, Shiori Tsuruhisa, Tomohiro Kurahachi, Naruki Higashidate, Tatsuru Kaji -
Annals of Clinical Nutrition and Metabolism 2026;18(1):10-17.
DOI: https://doi.org/10.15747/ACNM.25.0018
Published online: March 30, 2026
Department of Pediatric Surgery, Kurume University School of Medicine, Kurume, Japan
- Corresponding author: Tatsuru Kaji, e-mail: kaji_tatsuru@med.kurume-u.ac.jp
This article is a secondary publication of an article in Japanese published in the Japanese Journal of Surgical Metabolism and Nutrition, 2024;58(4):130-135. https://doi.org/10.11638/jssmn.58.4_130. The editors of both journals have granted permission for secondary publication.
This study was presented at the 60th Annual Meeting of the Japanese Society for Surgical Metabolism and Nutrition, held on July 7, 2023, in Tokyo, Japan.
• Received: February 9, 2026 • Revised: March 2, 2026 • Accepted: March 14, 2026
© 2026 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition · Asian Society of Surgical Metabolism and Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 485 Views
- 18 Download
- Abstract
- Introduction
- Medical care at SMID facilities and trends in referred patients
- Collaborative medical system between SMID facilities and Kurume University Hospital
- Examinations for status evaluation and clinical research achievements
- Current status and issues from the start of rounds to the present
- Conclusion
- Notes
- References
Abstract
-
Purpose Neurologically impaired patients often experience complex challenges in respiratory and nutritional management that may necessitate surgical intervention. Furthermore, some patients admitted to specialized facilities for neurologically impaired individuals do not receive adequate postoperative follow-up after being transferred. Kurume University Hospital has established a system of continuous routine rounds at such facilities. This review aims to describe the rationale, methods, and outcomes of multidisciplinary bedside support, with particular emphasis on nutritional evaluation, swallowing function assessment, and gastrointestinal function testing.
-
Current concept Routine collaboration between pediatric surgeons and facility-based pediatricians enables continuous perioperative management. Preoperatively, patient background, nutritional status, and family preferences are recorded through structured communication and shared decision-making tools, such as the Ottawa Personal Decision Guide. During hospitalization, multidisciplinary evaluations include bioelectrical impedance analysis for nutritional assessment, endoscopic and pH impedance testing for swallowing function, and multichannel intraluminal impedance monitoring for gastroesophageal reflux. Postoperatively, periodic facility rounds ensure ongoing evaluation, with repeated assessments guiding nutritional optimization, early complication detection, and timely surgical consultation. This approach provides families and healthcare teams with detailed information on functional outcomes, strengthens trust, and enhances continuity of care. Sustained bedside engagement at facilities for neurologically impaired patients improves pre- and postoperative monitoring, promotes seamless collaboration between institutions, and ensures individualized evaluation of nutrition, swallowing, and gastrointestinal function.
-
Conclusion By providing actionable data to families and multidisciplinary teams, this model strengthens shared decision-making and supports long-term outcomes. The system may serve as a framework for integrated perioperative care in similar high-risk patient populations.
Introduction
Patients with Severe Motor and Intellectual Disabilities (SMID) have a shortened life expectancy and suffer from numerous complications, including respiratory and gastrointestinal disorders. They are regarded as high-risk due to their need for continuous medical care and the presence of multiple comorbidities. The number of SMID patients nationwide is estimated to be approximately 47,000, with about 70% residing in facilities for children and adults with SMID (hereinafter referred to as SMID facilities) [1]. As of April 2022, there were 135 public corporation–run facilities (13,903 beds), 75 wards for children with SMID under the National Hospital Organization (8,148 beds), and one ward at the National Center for Advanced and Specialized Medical Care (60 beds) [2].
The recent increase in the number of SMID residents in such facilities is attributed to several factors, including a rise in patients requiring advanced medical care such as ventilator and gastrostomy management [3], the aging of caregivers; an increased caregiving burden related to environmental factors such as the limited capacity for therapeutic education [4,5]; and challenges in transitioning long-term patients from the NICU (neonatal intensive care unit) and pediatric wards to home care [6,7]. Additionally, it has been reported that approximately 20,000 children under 20 years of age nationwide require ongoing medical care [8]. As a result, pediatric surgeons are increasingly being consulted regarding surgical management.
However, among cases admitted to SMID facilities, postoperative functional evaluation is sometimes insufficient after transfer. Before our hospital began conducting regular rounds at these facilities, we often lacked comprehensive understanding of patients’ preoperative backgrounds and postoperative progress.
At SMID facilities, pediatricians routinely assess respiratory, mental, and physical functions. In general, pediatric surgeons are more likely to intervene surgically in conditions related to the respiratory system, gastrointestinal tract, and nutrition. As the number of patients requiring surgical intervention grows and postoperative recovery periods extend, requests for additional consultations from families and SMID facilities have also increased. To address these issues, we established a system of regular medical rounds at SMID facilities.
This paper introduces the ongoing efforts of the Department of Pediatric Surgery at Kurume University Hospital, which continuously evaluates the nutritional status, swallowing function, and gastrointestinal function of SMID patients in daily practice—from preadmission to postdischarge.
Medical care at SMID facilities and trends in referred patients
Kurume University Hospital is located in the southern part of Fukuoka Prefecture, with five SMID facilities situated within a 30 km radius. Since 2012, pediatric surgeons from our hospital have conducted rounds once or twice a month at four of these facilities. Medical care provided during these visits includes replacement of nutritional tubes such as gastrostomy tubes, elemental diet tubes, and gastrojejunostomy tubes, as well as tracheostomy cannula replacement. We also consult with facility physicians regarding nutritional content, medication prescriptions, and the necessity of surgical intervention. For patients who have undergone surgery at our hospital, regular inpatient evaluations are performed to assess postoperative function, as described later. The number of patients referred to our hospital was 10 before the initiation of rounds in 2012, but has steadily increased since the program’s introduction (Fig. 1).
Collaborative medical system between SMID facilities and Kurume University Hospital
Surgical procedures commonly performed on patients referred to our hospital include gastrostomy for nutritional supplementation, fundoplication for gastroesophageal reflux disease (GERD), and tracheostomy or laryngotracheal separation for swallowing disorders and pharyngolaryngeal reflux. Since the start of regular rounds, a collaborative system has been established in which pediatricians at SMID facilities and pediatric surgeons at our hospital coordinate care from the preoperative stage onward. After transfer to our hospital, pediatric surgeons conduct preoperative evaluations, while pediatricians provide perioperative support for underlying conditions. Following postoperative transfer back to the SMID facilities, pediatricians at the facilities continue observation, and our pediatric surgeons perform regular rounds to assess the patient’s status. This arrangement has established a truly collaborative system of care (Fig. 2). The following sections describe our initiatives from the preoperative through postoperative periods since the introduction of this system.
Preoperatively, we collect detailed patient information—including medical history, past history, family background, and nutritional methods—at SMID facilities and listen carefully to the wishes of the patient’s family to fully understand the patient’s condition before admission. Since the initiation of regular rounds, communication with the primary physicians at SMID facilities has become more detailed and effective. Furthermore, by explaining the content of preoperative examinations and anticipated treatments to the patient’s family before transfer to our hospital, we have been able to establish trusting relationships even before admission.
Information sharing and decision-making support for families using the Ottawa Personal Decision Guide
For SMID patients who are unable to express their own wishes, decision-making regarding treatment is typically delegated to their families. Our hospital employs the Ottawa Personal Decision Guide developed by Dr. O’Connor and colleagues at the University of Ottawa [9]. Nurses use this guide to help families clarify their values, understand their emotional state, and receive the information necessary to make informed decisions. Unlike traditional informed consent, this structured approach facilitates mutual understanding of family perspectives regarding examinations and treatments, thereby fostering more meaningful communication and trust.
Nutritional evaluation
Nutritional assessments are performed using blood tests, indirect calorimetry, and bioelectrical impedance analysis (BIA) to quantify nutritional status and guide perioperative management.
Swallowing function tests
Swallowing endoscopy conducted by an otolaryngologist and hypopharyngeal pH impedance testing are performed to evaluate swallowing function. In cases of recurrent aspiration pneumonia, laryngotracheal separation is performed to prevent further respiratory complications.
Pre-gastrostomy evaluation for GERD and pharyngolaryngeal reflux
To assess for GERD and pharyngolaryngeal reflux prior to gastrostomy, patients undergo an upper gastrointestinal contrast study, 24-hour esophageal pH impedance monitoring (multichannel intraluminal impedance–pH monitoring [MII-pH]), and upper gastrointestinal endoscopy. When severe GERD is identified, both fundoplication and gastrostomy are performed; if no reflux is observed, only gastrostomy is carried out.
In addition to regular rounds for postoperative assessment, nutritional consultation, and medication management, postoperative examinations are scheduled as necessary to ensure continuous follow-up and optimization of care.
Examinations for status evaluation and clinical research achievements
In a study examining the relationship between phase angle (PhA) measured by BIA and serum albumin levels, it was shown that PhA in SMID patients is lower than in healthy individuals and that SMID patients with hypoalbuminemia (serum albumin <3.5 g/dL) have significantly lower PhA values than normal cases [10]. In another study evaluating resting energy expenditure (REE), fat-free mass (FFM), and fat mass in SMID patients, a significant correlation was found between FFM and REE. The predictive formula for REE (kcal/day)=550.6+166.6×FFM (kg) was established [11]. Appropriate nutritional management during hospitalization before surgery contributes to improved perioperative nutritional control in SMID patients.
According to the Swallowing Disorder Clinical Practice Guidelines, swallowing endoscopy is a valuable and essential tool for evaluating swallowing function [12]. In SMID patients, videofluoroscopic swallowing studies pose a high risk of aspiration; therefore, our hospital employs swallowing endoscopy and hypopharyngeal pH impedance testing instead. Swallowing endoscopy is scored using the Hyodo system, which assesses saliva retention, laryngeal sensation, elicitation of the swallowing reflex, pharyngeal clearance, and the degree of aspiration. Hypopharyngeal pH impedance testing enables evaluation not only of reflux reaching the hypopharynx but also of impedance values around the pyriform sinus. Because impedance values decrease when fluid accumulates, we reported that the Hyodo score and pharyngeal baseline impedance are negatively correlated, and that a low hypopharyngeal impedance value indicates saliva retention (Fig. 3) [13], with a cutoff value of 1,552 Ω. While swallowing endoscopy allows assessment of saliva retention and glottic penetration, SMID patients often cannot follow instructions. Therefore, for patients with hyperactivity or strong muscle tone, hypopharyngeal pH impedance testing is considered particularly useful. In the past, when SMID facilities consulted us regarding tracheostomy or laryngotracheal separation, there was often a gap between the family’s understanding and the patient’s actual condition. Since the introduction of regular rounds, however, we have been able to provide families with more accurate information based on accumulated test results and direct examinations. This approach has enabled us to better understand patients’ current conditions and to explain both the necessity of surgery and the expected postoperative course.
In our department, MII-pH testing is performed before and after fundoplication in SMID patients with GERD. We reported that each measured parameter showed significant improvement following surgery (Fig. 4) [14]. Furthermore, we demonstrated that 70 reflux episodes identified by MII-pH testing correspond to a pH index of 9% and a baseline impedance value of approximately 1,000 Ω, and that these thresholds can serve as useful indicators for performing fundoplication [15]. Based on these findings, we have established a treatment flowchart for GERD management in our department (Fig. 5) [16]. In a separate evaluation of MII-pH testing before and after gastrostomy, we found no significant differences in parameters between pre- and postoperative assessments. However, we experienced one case—a 3-year-old girl—in whom fundoplication was performed 3 years after gastrostomy. This patient showed a tendency toward a high number of reflux episodes before the initial surgery, and we consider such cases to require special attention (Fig. 6) [16]. As with swallowing function testing, gastrointestinal function testing enables us to provide families with clear and objective information. Conducting treatment with the family’s understanding and continuing careful postoperative observation fosters stronger trust between the medical team and the family.
Current status and issues from the start of rounds to the present
Children requiring home medical care can be continuously monitored for postoperative function because they regularly visit outpatient clinics for tracheostomy site observation and gastrostomy tube replacement. However, in cases where patients are transferred to SMID facilities after surgery, there are currently no formal reports from the surgical facility regarding the implementation of rounds or the content of postoperative evaluations. According to 2018 data, the number of children using ventilators was reported to be 4,178, and the total number of children requiring medical care has doubled in the past 10 years, while the number requiring ventilator management has increased more than tenfold. The increase is particularly notable among children aged 0–4 years [17], suggesting that the number of children requiring medical care in SMID facilities will continue to grow. At our hospital, the current system allows us to assess each patient’s condition in advance through preoperative rounds, enabling information sharing with hospital physicians prior to admission. In addition, based on accumulated test results, we can now provide more detailed explanations to key persons (typically the patient’s family). Surgical policies can be determined more clearly using objective functional assessments, and by directly observing patients’ postoperative progress, not only physicians at SMID facilities but also nurses can offer more specific explanations to families, fostering a deeper understanding of both disease and treatment.
For pediatric surgeons, it is also advantageous to monitor postoperative conditions closely and to verify the appropriateness and effectiveness of surgical procedures. However, after transfer to a facility, there are cases where marked weight gain is observed. One possible explanation is that tracheostomy or laryngotracheal separation, performed in patients who previously required substantial respiratory effort, reduces the energy expenditure needed for breathing, thereby increasing available calories for weight gain. Continuing regular rounds enables early recognition and management of such issues.
Moreover, since the introduction of rounds, an environment has been created in which consultations are more readily initiated. Face-to-face contact between facility pediatricians and hospital surgeons has facilitated smoother communication and is thought to have contributed to the increased number of referrals. Ongoing rounds before and after surgery, combined with active medical collaboration, have had a positive impact on SMID patients, their families, and healthcare providers. We believe this system could serve as a model for medical systems.
Conclusion
We have described initiatives aimed at providing continuous, integrated medical care for SMID patients. Through the implementation of regular rounds, it has become possible to observe both preoperative and postoperative conditions systematically and to maintain effective collaboration with SMID facilities, thereby strengthening continuity and quality of care.
Authors’ contribution
Conceptualization: DM, TK (Tatsuru Kaji). Data curation: DM. Formal analysis: DM, NH (Naoki Hashizume), YK. Investigation: DM, TA, HE, HY, ST (Shotaro Taki). Methodology: DM, TK (Tomohiro Kurahachi), ST (Shiori Tsuruhisa). Project administration: DM, NH (Naoki Hashizume). Supervision: NH (Naoki Hashizume), TK (Tatsuru Kaji). Validation: DM, YK. Visualization: NH (Naruki Higashidate), TK (Tomohiro Kurahachi). Writing–original draft: DM, NH (Naoki Hashizume). Writing–review & editing: KH, HE, HY, ST (Shiori Tsuruhisa), TA, TK (Tomohiro Kurahachi), ST (Shotaro Taki), NH (Naruki Higashidate), TK (Tatsuru Kaji). All authors read and approved the final manuscript.
Conflict of interest
The author of this manuscript has no conflicts of interest to disclose.
Funding
None.
Data availability
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
None.
Supplementary materials
None.
Fig. 1.
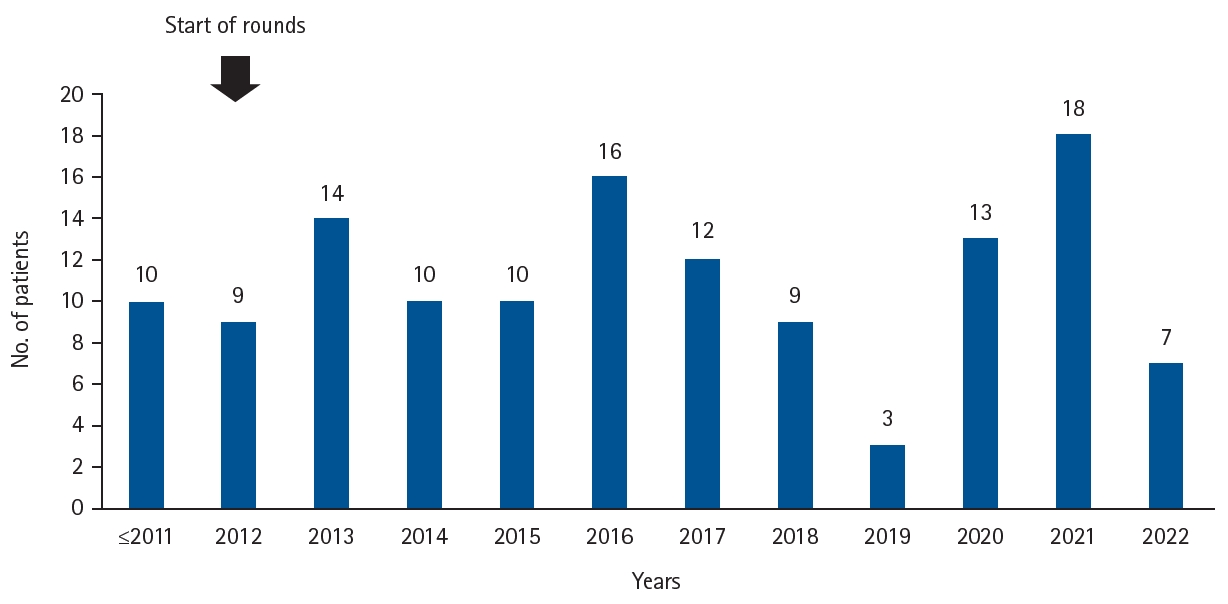
Trends in the number of patients referred from facilities for neurologically impaired patients to our hospital. Before the start of regular rounds in 2012, the total number of patients was about 10. After the start of rounds, the number of referrals gradually increased.
Fig. 2.
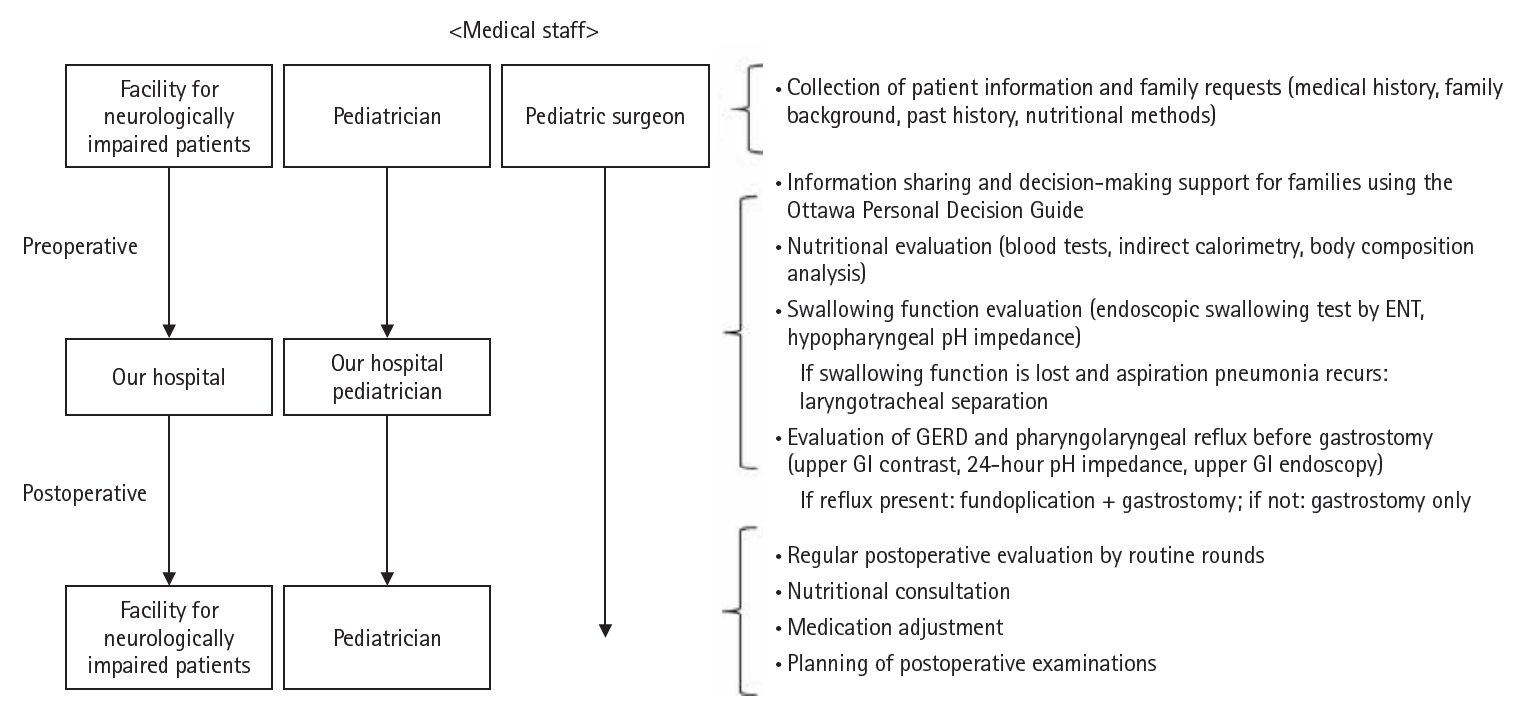
Medical collaboration system between facilities and our hospital. After the start of rounds, seamless care is provided for patients requiring respiratory and nutritional management. From the preoperative stage, pediatricians at the facility and pediatric surgeons at our hospital collaborate, and after transfer, pediatric surgeons perform preoperative evaluation and pediatricians provide perioperative support for underlying diseases. GERD, gastroesophageal reflux disease; GI, gastrointestinal.
Fig. 3.
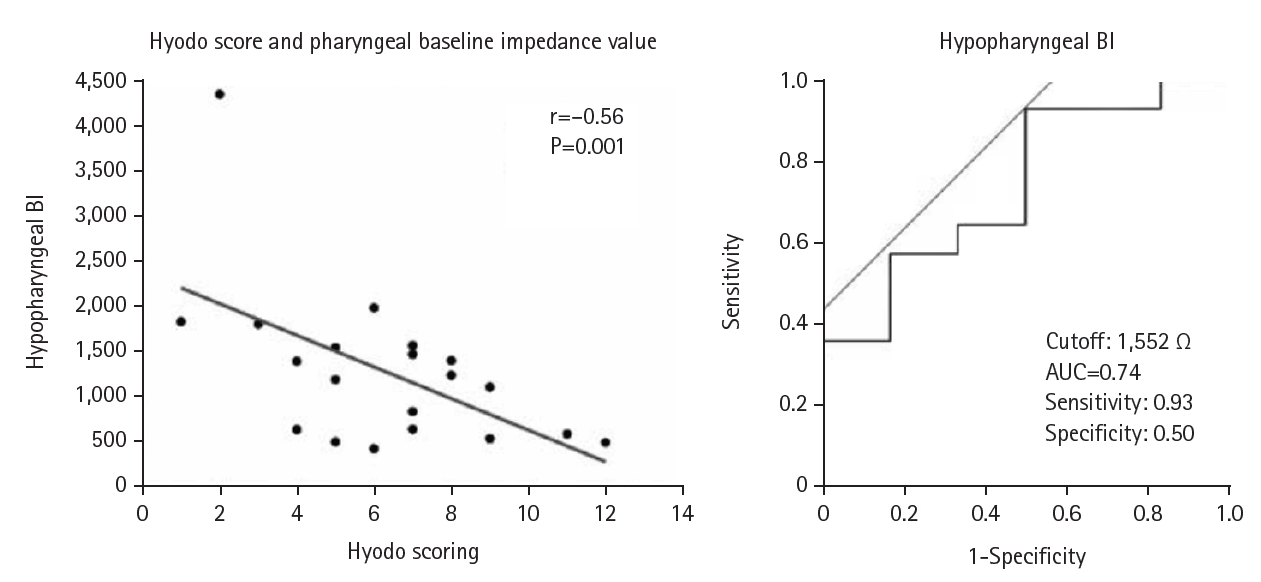
Swallowing function evaluation using hypopharyngeal pH impedance test. The negative correlation between Hyodo score and baseline pharyngeal impedance value suggests that low hypopharyngeal impedance indicates saliva retention. BI, baseline impedance; AUC, area under the curve. Adapted from Masui et al. [13].
Fig. 4.
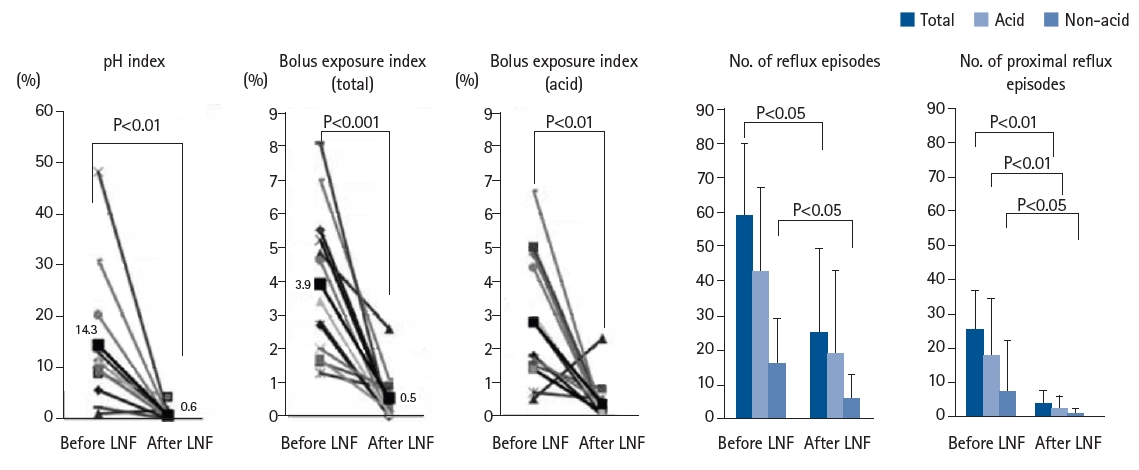
24-Hour pH impedance test: pre- and post-fundoplication evaluation. Each parameter showed significant improvement after surgery. LNF, laparoscopic Nissen fundoplication. Adapted from Fukahori et al., with permission of Elsever [14].
Fig. 5.
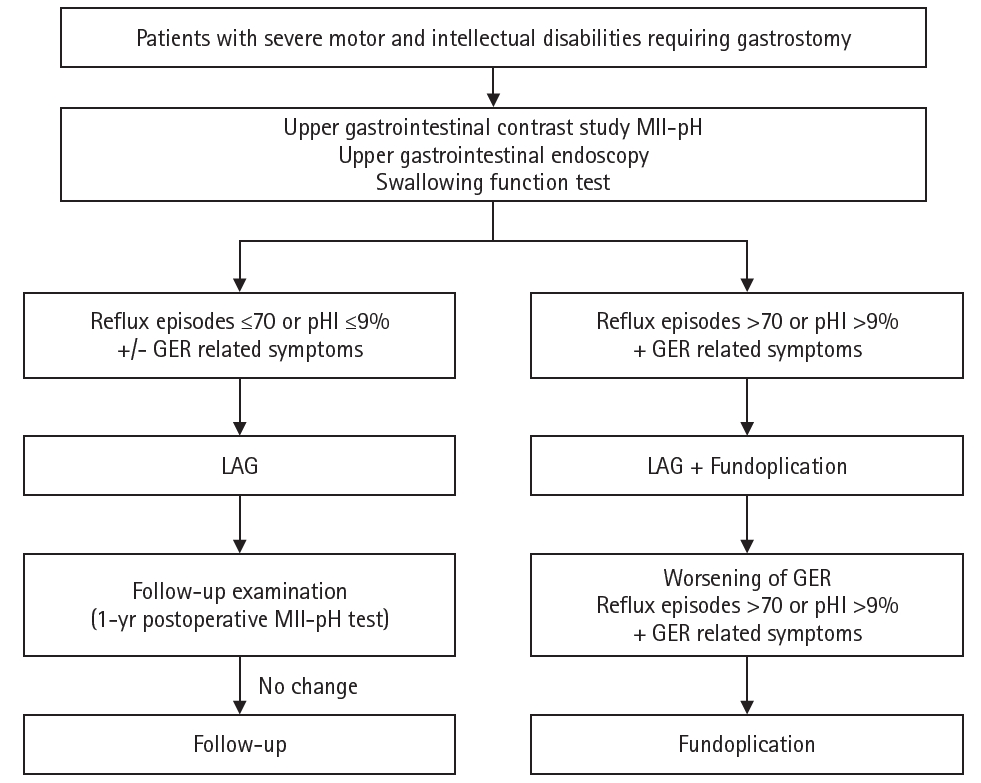
Flowchart for surgical decision-making. A flowchart has been created to determine whether to perform LAG alone or in combination with fundoplication for neurologically impaired patients requiring gastrostomy. MII-pH, multichannel intraluminal impedance–pH monitoring; GER, gastroesophageal reflux; LAG, laparoscopy-aided gastrostomy. Reprinted from Masui et al., with permission of Springer Nature [16].
Fig. 6.
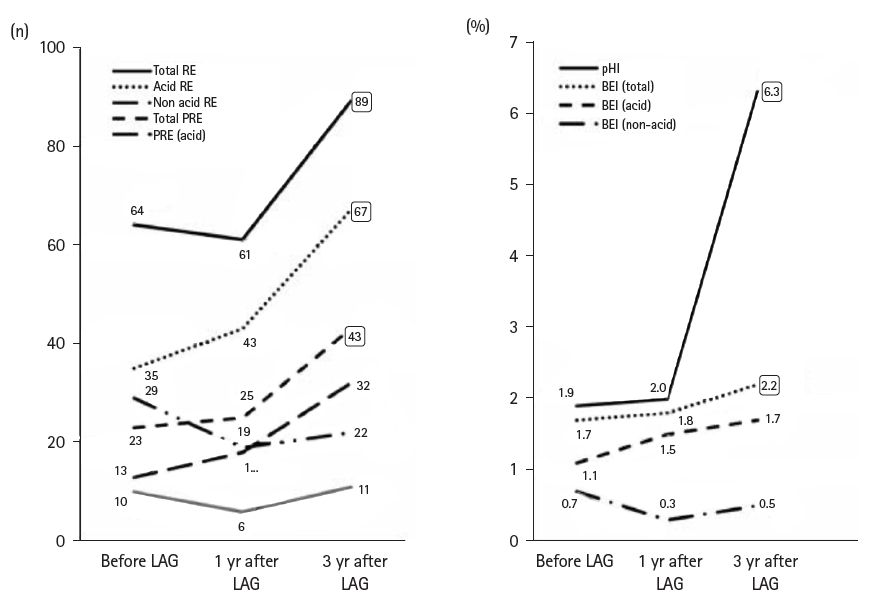
Comparison of MII-pH parameters before and after laparoscopy-aided gastrostomy. In one case (a 3-year-old girl), fundoplication was added 3 years after gastrostomy due to worsening parameters. Patients with a high number of reflux episodes before surgery should be carefully monitored. RE, reflux episodes; PRE, proximal reflux episodes; BEI, bolus exposure index; MII-pH, multichannel intraluminal impedance–pH monitoring; LAG, laparoscopy-aided gastrostomy. Reprinted from Masui et al., with permission of Springer Nature [16].
- 1. Matsuba S. Frequency and causes of severe motor and intellectual disabilities. In: Okada Y, Konishi T, Igai M, Ishii Mi, eds. New edition: manual for the care of patients with severe motor and intellectual disabilities. Ishiyaku Publishers; 2015. p. 41-6.
- 2. National Association for the Protection of Children (and Adults) with Severe Motor and Intellectual Disabilities. List of Facilities for Children and Adults with Severe Motor and Intellectual Disabilities [Internet]. National Association for the Protection of Children (and Adults) with Severe Motor and Intellectual Disabilities; 2022. [cited 2025 Oct 20]. Available from: https://www.mamorukai.jp/wp-content/uploads/2023/01/shisetsuR4.pdf
- 3. Tamura M. Comprehensive Research Project on Disability Policy. Research on Actual Conditions and Collaboration in Medical, Welfare, Health, and Education for Children Requiring Medical Care: 2016 General and Joint Research Report. Ministry of Health, Labour and Welfare; 2017.
- 4. Takahara S, Yumitate Y, Yamamoto T. The current state of child-rearing burden on families of patients using short-term medical care facilities. Chugoku Shikoku Natl Hosp Org J Nurs 2015;11:303-6.
- 5. Nishigaki K, Kuroki H, Fujioka H. Factors related to the desire for respite care among primary caregivers of children with severe physical and mental disabilities at home. J Child Health 2014;73:475-83.
- 6. Iwasaki Y, Kamuro K, Miyanomae T, Kurasawa T, Masuyama T, Tamura M. Survey on the current status of admissions to nursing homes for children requiring medical care and children admitted to NICUs for long periods. Jpn J Soc Severe Phys Ment Disabil 2012;37:117-24.
- 7. Funamoto J, Mori T, Umehara M, Ebara A. Issues in transition to home care or facilities for children with long-term hospitalization. J Jpn Pediatr Soc 2013;117:1321-5.
- 8. Nakamura T. Current status and future aspects of home care medicine for children with medical complexity. Organ Biol 2020;27:21-30.
- 9. Stacey D, Legare F, Boland L, Lewis KB, Loiselle MC, Hoefel L, et al. 20th Anniversary Ottawa Decision Support Framework: Part 3 Overview of Systematic Reviews and Updated Framework. Med Decis Making 2020;40:379-98. ArticlePubMedPDF
- 10. Yoshida M, Asagiri K, Fukahori S, Tanaka Y, Hashizume N, Ishii S, et al. The utility of a phase angle analysis in patients with severe motor and intellectual disabilities. Brain Dev 2017;39:557-63. ArticlePubMed
- 11. Hashizume N, Tanaka Y, Yoshida M, Fukahori S, Ishii S, Saikusa N, et al. Resting energy expenditure prediction using bioelectrical impedance analysis in patients with severe motor and intellectual disabilities. Brain Dev 2019;41:352-8. ArticlePubMed
- 12. Hyodo M. Swallowing disorder clinical practice guidelines. Nihon Naika Gakkai Zasshi 2020;109:2370-7.
- 13. Masui D, Fukahori S, Hashizume N, Ishii S, Higashidate N, Sakamoto S, et al. Simultaneous evaluation of laryngopharyngeal reflux and swallowing function using hypopharyngeal multichannel intraluminal impedance measurements in neurologically impaired patients. J Neurogastroenterol Motil 2021;27:198-204. ArticlePubMedPMC
- 14. Fukahori S, Yagi M, Ishii S, Asagiri K, Saikusa N, Hashizume N, et al. Laparoscopic Nissen fundoplication mainly reduces the volume of acid reflux and potentially improves mucosal integrity up to the middle esophagus in neurologically impaired children detected by esophageal combined pH-multichannel intraluminal impedance measurements. J Pediatr Surg 2016;51:1283-7. ArticlePubMed
- 15. Fukahori S, Yagi M, Ishii S, Asagiri K, Saikusa N, Hashizume N, et al. Analyses of the relationship between a 'number of reflux episodes' exceeding 70 and the pH index in neurologically impaired children by evaluating esophageal combined pH-multichannel intraluminal impedance measurements. Scand J Gastroenterol 2018;53:519-26. ArticlePubMed
- 16. Masui D, Fukahori S, Hashizume N, Ishii S, Higashidate N, Koga Y, et al. Influence of laparoscopy-aided gastrostomy on gastroesophageal reflux in neurologically impaired patients using multichannel intraluminal impedance pH measurements. Esophagus 2022;19:360-6. ArticlePubMedPDF
- 17. Tamura M. Comprehensive Research Project on Disability Policy. Research on Actual Conditions and Collaboration in Medical, Welfare, Health, and Education for Children Requiring Medical Care: 2018 General and Joint Research Report. Ministry of Health, Labour and Welfare; 2019.
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteBedside support for neurologically impaired patients via nutritional evaluations, swallowing function assessments, and gastrointestinal function tests: a narrative review
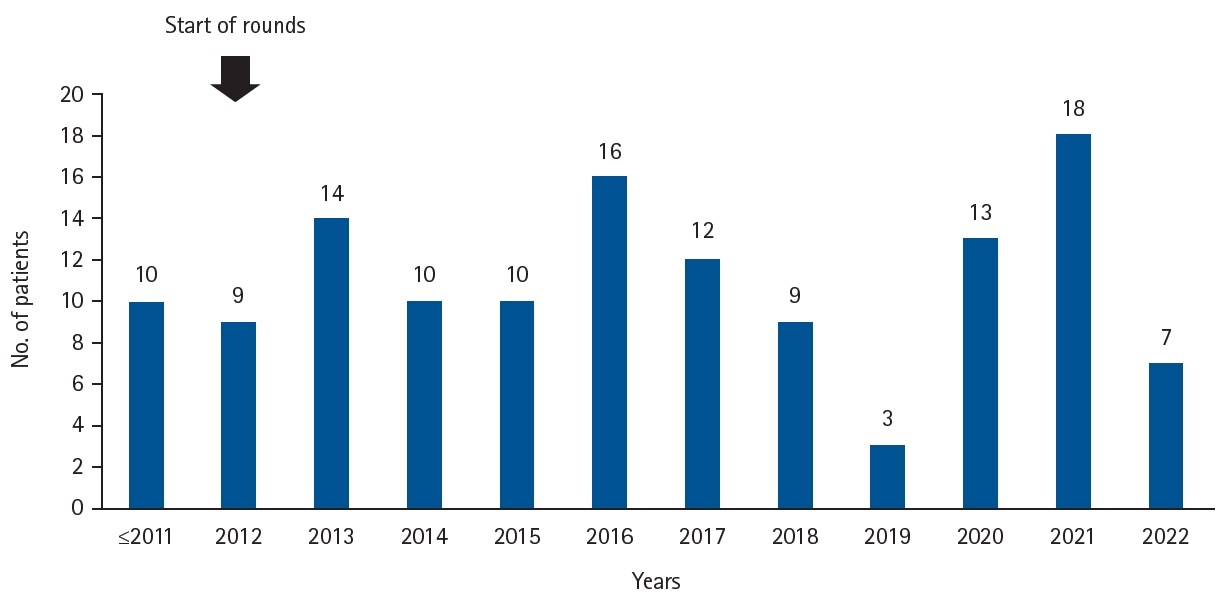
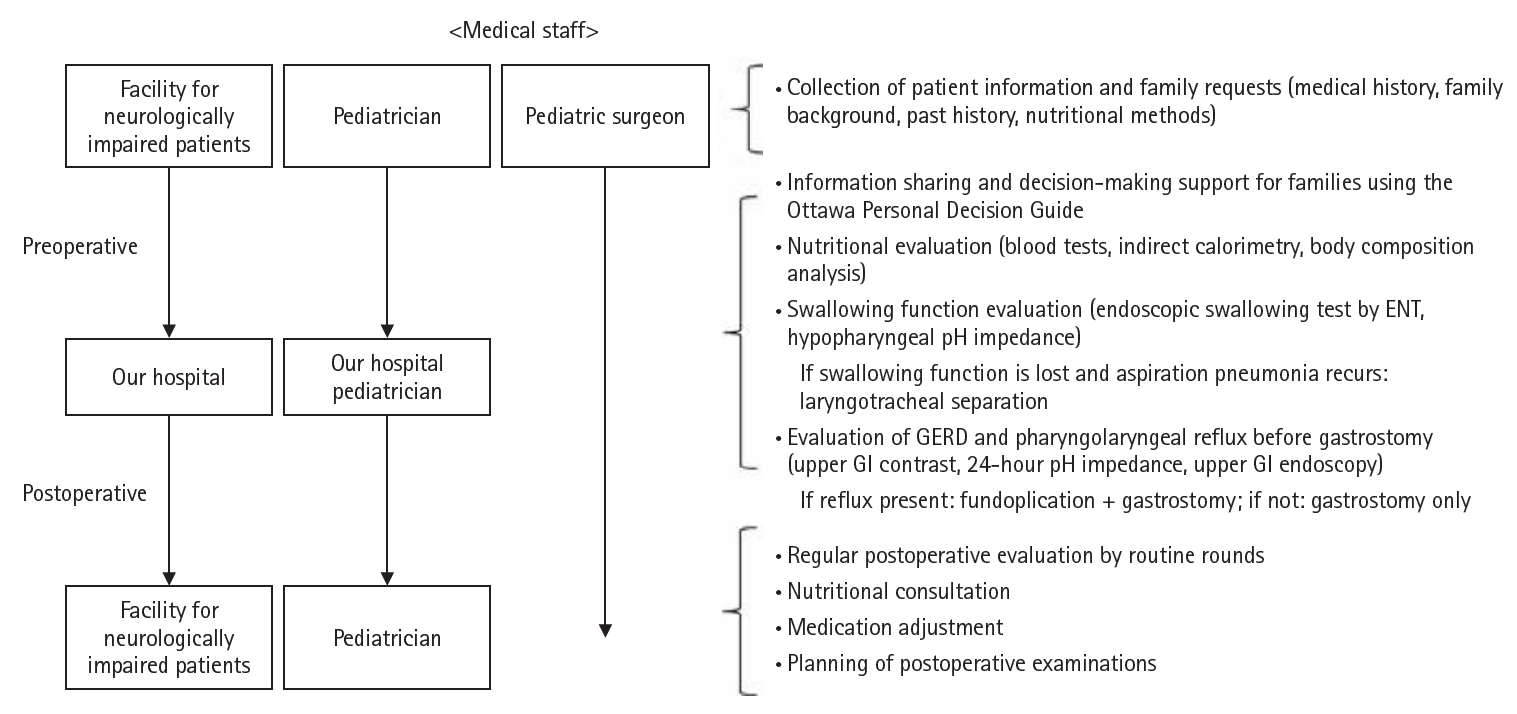
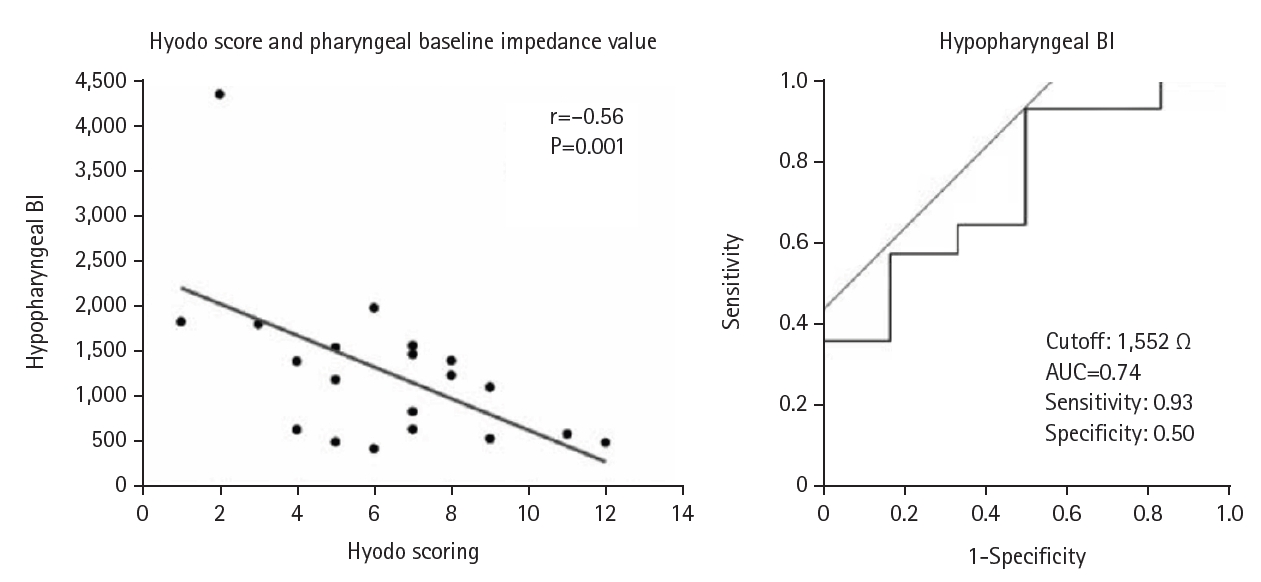
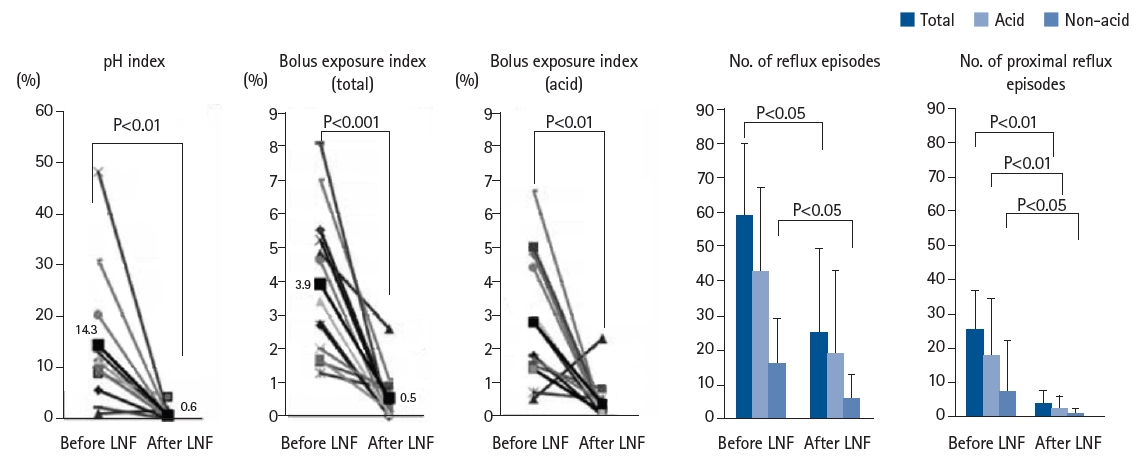
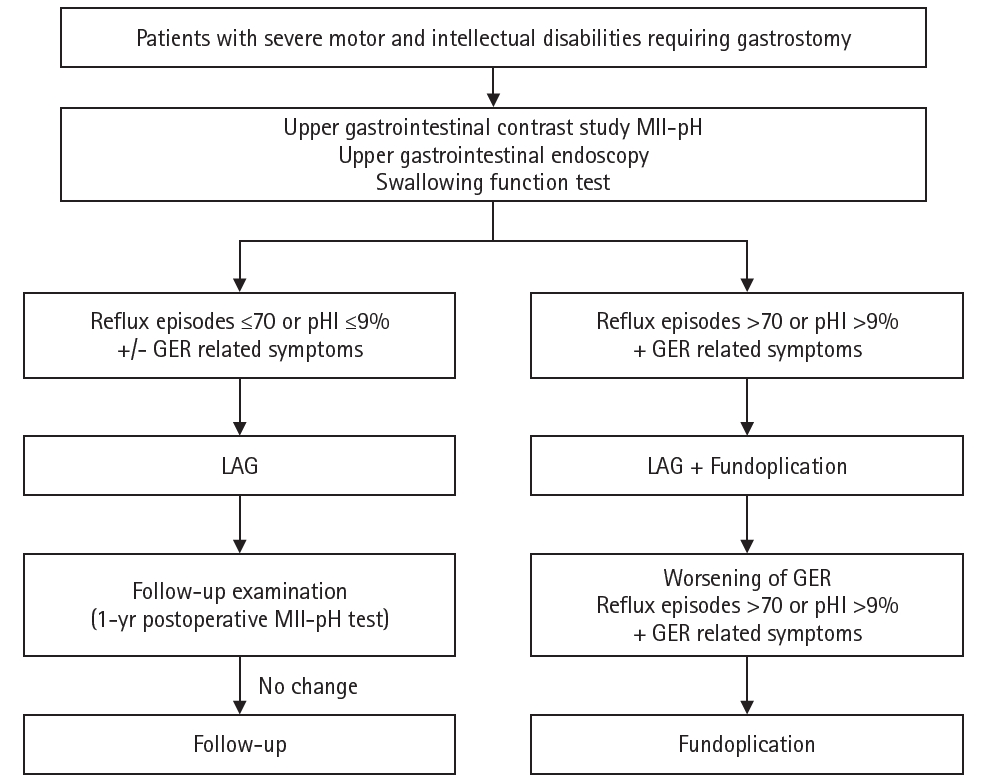
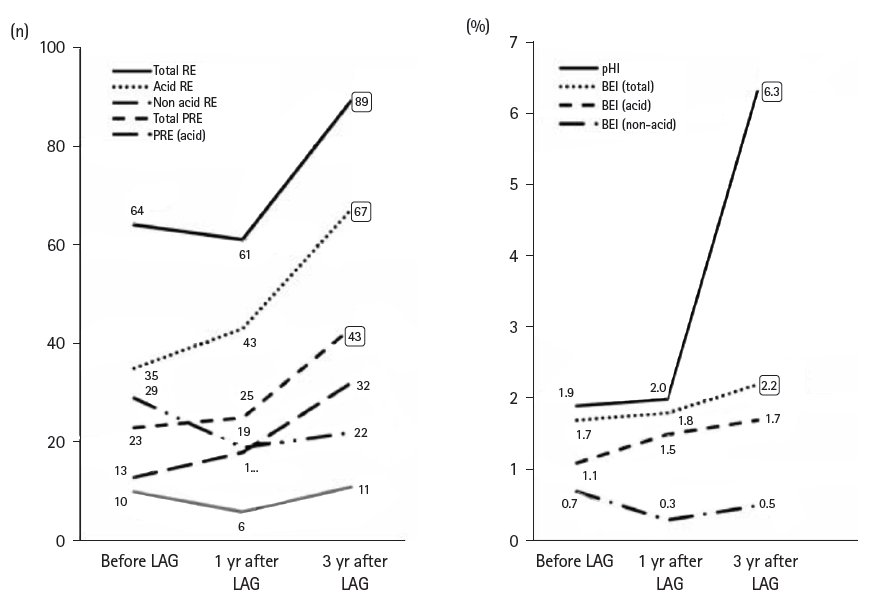
Fig. 1. Trends in the number of patients referred from facilities for neurologically impaired patients to our hospital. Before the start of regular rounds in 2012, the total number of patients was about 10. After the start of rounds, the number of referrals gradually increased.
Fig. 2. Medical collaboration system between facilities and our hospital. After the start of rounds, seamless care is provided for patients requiring respiratory and nutritional management. From the preoperative stage, pediatricians at the facility and pediatric surgeons at our hospital collaborate, and after transfer, pediatric surgeons perform preoperative evaluation and pediatricians provide perioperative support for underlying diseases. GERD, gastroesophageal reflux disease; GI, gastrointestinal.
Fig. 3. Swallowing function evaluation using hypopharyngeal pH impedance test. The negative correlation between Hyodo score and baseline pharyngeal impedance value suggests that low hypopharyngeal impedance indicates saliva retention. BI, baseline impedance; AUC, area under the curve. Adapted from Masui et al. [13].
Fig. 4. 24-Hour pH impedance test: pre- and post-fundoplication evaluation. Each parameter showed significant improvement after surgery. LNF, laparoscopic Nissen fundoplication. Adapted from Fukahori et al., with permission of Elsever [14].
Fig. 5. Flowchart for surgical decision-making. A flowchart has been created to determine whether to perform LAG alone or in combination with fundoplication for neurologically impaired patients requiring gastrostomy. MII-pH, multichannel intraluminal impedance–pH monitoring; GER, gastroesophageal reflux; LAG, laparoscopy-aided gastrostomy. Reprinted from Masui et al., with permission of Springer Nature [16].
Fig. 6. Comparison of MII-pH parameters before and after laparoscopy-aided gastrostomy. In one case (a 3-year-old girl), fundoplication was added 3 years after gastrostomy due to worsening parameters. Patients with a high number of reflux episodes before surgery should be carefully monitored. RE, reflux episodes; PRE, proximal reflux episodes; BEI, bolus exposure index; MII-pH, multichannel intraluminal impedance–pH monitoring; LAG, laparoscopy-aided gastrostomy. Reprinted from Masui et al., with permission of Springer Nature [16].
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Bedside support for neurologically impaired patients via nutritional evaluations, swallowing function assessments, and gastrointestinal function tests: a narrative review

