 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 18(1); 2026 > Article
- Review Effectiveness of perioperative rehabilitation and nutrition in esophageal cancer: a narrative review
-
Ryoma Haneda1
 , Yuki Sakai1, Kenichi Sekimori1, Tomohiro Murakami1, Eisuke Booka1, Tomohiro Matsumoto1, Hirotoshi Kikuchi1, Yoshihiro Hiramatsu1,2, Hiroya Takeuchi1
, Yuki Sakai1, Kenichi Sekimori1, Tomohiro Murakami1, Eisuke Booka1, Tomohiro Matsumoto1, Hirotoshi Kikuchi1, Yoshihiro Hiramatsu1,2, Hiroya Takeuchi1 -
Annals of Clinical Nutrition and Metabolism 2026;18(1):18-26.
DOI: https://doi.org/10.15747/ACNM.25.0021
Published online: March 30, 2026
1Department of Surgery, Hamamatsu University School of Medicine, Hamamatsu, Japan
2Department of Perioperative Functioning Care and Support, Hamamatsu University School of Medicine, Hamamatsu, Japan
- Corresponding author: Hiroya Takeuchi, email: takeuchi@hama-med.ac.jp
This article is a secondary publication of an article in Japanese published in the Japanese Journal of Surgical Metabolism and Nutrition, 2024;58(6):216-222. https://doi.org/10.11638/jssmn.58.6_216. The editors of both journals have granted permission for secondary publication.
This study was presented at the 60th Annual Meeting of the Japanese Society of Surgical Metabolism and Nutrition, held on July 7, 2023, in Tokyo, Japan.
• Received: December 21, 2025 • Revised: January 18, 2026 • Accepted: January 21, 2026
© 2026 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition · Asian Society of Surgical Metabolism and Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,293 Views
- 18 Download
Abstract
-
Purpose Esophageal cancer surgery requires robust perioperative management to reduce its high rate of complications. This review evaluates the clinical utility of comprehensive exercise and nutritional therapy, with a specific focus on initiatives led by the multidisciplinary Hamamatsu Perioperative Care Team (HOPE), established at Hamamatsu University Hospital to optimize patient safety and postoperative recovery outcomes.
-
Current concept The HOPE protocol involves a diverse team, including surgeons, nurses, pharmacists, and dietitians, who collaboratively implement a multifaceted perioperative care bundle. These interventions include strict smoking cessation, intensive oral care, and immunonutrition incorporating n-3 fatty acids. A distinctive feature of this program is the integration of patient-reported treatment diaries and wearable fitness tracking devices (WFTs) to visualize daily activity, thereby helping to sustain patient motivation. Preoperative rehabilitation focuses on preventing sarcopenia through combined aerobic and resistance training, while postoperative care emphasizes immediate enteral nutrition and early mobilization. Retrospective analyses demonstrated that HOPE implementation reduced Clavien-Dindo grade III or higher infectious complications, pneumonia and surgical site infections, compared with historical controls. In addition, a propensity score–matched analysis showed that WFT users experienced lower pneumonia rates, shorter hospital stays, and better preservation of nutritional markers, including albumin and transthyretin, during the recovery phase compared with non-users.
-
Conclusion The HOPE strategy illustrates that combining standard nutritional support and exercise therapy with digital tools enables individualized rehabilitation. This integrated approach reduces morbidity and preserves function, strongly suggesting that incorporation of wearable technology into established surgical care protocols represents a strategy for improving long-term outcomes in high-risk cancer patients.
Introduction
Esophageal cancer is associated with a poor prognosis and ranks as the sixth leading cause of cancer-related death worldwide [1]. The standard surgical procedure for esophageal cancer is subtotal esophagectomy, which involves operative manipulation of three anatomical regions: the cervical, thoracic, and abdominal areas. Consequently, the degree of surgical invasiveness is substantial, and the incidence of postoperative complications is higher than that observed in other gastrointestinal surgeries. To promote rapid postoperative recovery and prevent complications, the concept of Enhanced Recovery After Surgery (ERAS), also referred to as fast-track surgery, has been introduced and widely established in surgical practice. The ERAS protocol was proposed by the ERAS group of the European Society for Clinical Nutrition and Metabolism and aims to prevent postoperative complications, shorten hospital stay, and improve patient safety through the comprehensive implementation of recovery-enhancing measures [2]. Among these components, exercise therapy recommends muscle strength training and respiratory rehabilitation beginning in the preoperative period, along with early mobilization after surgery. In recent years, the usefulness of these interventions has been increasingly recognized, as reflected by their approval for reimbursement within medical fee systems. With respect to nutritional therapy, systematic nutritional assessment and early intervention starting in the preoperative period are required, and early postoperative enteral nutrition has been shown to reduce the incidence of postoperative complications.
In this paper, we outline the usefulness of perioperative exercise and nutritional therapy in esophageal cancer surgery and describe the specific efforts undertaken by our perioperative management team to implement these interventions in clinical practice.
Perioperative team medicine
The usefulness of perioperative management teams has been widely reported as a means of achieving safer perioperative care by enabling multidisciplinary medical staff to apply the specific strengths of each profession while sharing patient information across organizational boundaries. Shirakawa et al. [3] established the Perioperative Management Center (PERiO) in 2008. For patients with esophageal cancer, PERiO provides a comprehensive range of services, including preoperative smoking cessation guidance; assessment of physical function and general condition before and after surgery; exercise therapy; oral care delivered by the dental department; postoperative eating and swallowing rehabilitation; respiratory physical therapy; and assistance with basic movement (Table 1) [3]. Following the introduction of PERiO, reductions were reported in both the time to postoperative ambulation and the length of postoperative hospital stay among patients undergoing esophageal cancer surgery. Additionally, the incidence of adverse events during preoperative chemotherapy was reported to have significantly decreased after PERiO implementation [4].
Watanabe et al. [5] established a Perioperative Team at the Cancer Institute Hospital (PeriCan) in 2013. This team provides preoperative guidance on abstinence from alcohol and smoking, oral care, early postoperative mobilization, rehabilitation, assessment of swallowing function, and dietary guidance (Table 1). In a comparison of short-term outcomes before and after the introduction of PeriCan in 113 patients who underwent esophagectomy, postoperative complications, particularly postoperative pneumonia, were reported to be significantly reduced [5]. Furthermore, even among patients who developed postoperative recurrent laryngeal nerve palsy, the incidence of postoperative pneumonia was significantly lower after the introduction of PeriCan [5]. In Japan, the Ministry of Health, Labour and Welfare actively promotes team-based medical care to enhance the quality of healthcare delivery and improve efficiency through the effective utilization of specialized professionals and strengthened interprofessional collaboration. In line with this policy, numerous reports on perioperative management teams have been published (Table 1) [6-10].
At our hospital, beginning in April 2017, we launched the Hamamatsu Perioperative Care Team (HOPE), which consists of doctors, nurses (outpatient, ward, intensive care unit [ICU], and operating room), the rehabilitation department, pharmacists, registered dietitians, the dental department, the infection control team, and the palliative care team. This multidisciplinary team aims to implement safe perioperative management while improving long-term prognosis and enhancing patients’ long-term quality of life. The perioperative management bundle implemented by HOPE is described below.
For esophageal cancer patients scheduled for surgery, HOPE staff intervene beginning at the first outpatient visit. After the physician explains the medical condition, the outpatient nurse provides psychological support and lifestyle guidance to the patient. In our department, all esophageal cancer patients are instructed to abstain from smoking and drinking for more than 1 month (Fig. 1). In the dental department, oral evaluation and oral care are performed, while rehabilitation specialists measure baseline physical function, including walking speed, grip strength, and knee extension muscle strength. They also conduct cardiopulmonary exercise testing and provide individualized aerobic and resistance exercise guidance for preoperative rehabilitation to prevent sarcopenia (Fig. 1). At the same time, respiratory physical therapy using an incentive spirometer is initiated, and guidance on sputum expectoration is provided.
In addition, registered dietitians conduct a detailed interview regarding the patient’s dietary intake, measure upper arm circumference, triceps skinfold thickness, upper arm muscle circumference, and lower limb circumference, and perform body composition analysis using InBody to comprehensively evaluate preoperative nutritional status (Fig. 1). In preoperative nutritional management, previous reports have shown that administration of n-3 fatty acid–enriched nutritional supplements from the preoperative period significantly shortens ICU stay and the duration of systemic inflammatory response syndrome and reduces postoperative infectious complications [11]. According to parenteral and enteral nutrition guidelines, enteral nutrition should be considered first as the route of nutritional administration. If oral intake is possible, semi-digested enteral nutrition is administered orally as oral nutritional support (ONS). When severe tumor-related stenosis is present, a nasogastric feeding tube or percutaneous endoscopic gastrostomy is performed to provide enteral nutrition (Fig. 1).
A HOPE conference is held once a week to share information regarding required nutritional intake, actual dietary intake, rehabilitation progress, and gastrointestinal symptoms such as vomiting and diarrhea. This process enables risk visualization and promotes information sharing among multiple professions. Since 2019, to encourage active patient participation in preoperative rehabilitation, a treatment diary has been provided. Patients record daily dietary intake, exercise volume, the number of respiratory rehabilitation sessions, tooth brushing frequency, and subjective symptoms (Fig. 2). In addition, patients wear a wearable fitness tracking device (WFT; Fitbit) to record heart rate, step count, physical activity, calories burned, and sleep duration. By visualizing physical activity using the WFT, the outcomes of perioperative rehabilitation become more apparent, and patient motivation is expected to improve. Patients are admitted 5 days before surgery, consume ONS orally, and receive daily rehabilitation interventions to implement intensive preoperative nutritional and exercise therapy.
In all cases, nasal screening for methicillin-resistant Staphylococcus aureus (MRSA) is performed. When results are positive, mupirocin calcium ointment, chlorhexidine disinfection, and perioperative anti-MRSA agents are administered to prevent postoperative pneumonia and surgical site infection (Fig. 1).
Surgery is performed with the aim of achieving safe and minimally invasive treatment, including the use of robot-assisted surgery when appropriate, with careful attention to avoiding recurrent laryngeal nerve palsy. Prolonged bed rest after surgery leads to the progression of respiratory dysfunction induced during the surgical procedure. In addition, the accumulation of airway secretions, exudate, and blood causes peripheral airway obstruction in the lower lungs, resulting in decreased alveolar ventilation and, ultimately, alveolar collapse. Furthermore, reduced physical activity associated with prolonged postoperative bed rest is known to cause secondary complications, including muscle atrophy, bone atrophy, orthostatic hypotension, and pressure ulcers. Therefore, provided there are no problems with the general condition, particularly respiratory and circulatory dynamics, early mobilization beginning on the first postoperative day is strongly recommended [13].
In addition to preventing disuse of the limbs through standing and walking, early mobilization improves ventilation–perfusion imbalance, increases respiratory airflow, and allows exercise-induced bronchial dilation, which is expected to promote sputum clearance. In our department, pain control is managed in consultation with anesthesiologists, and both early mobilization and early initiation of respiratory physical therapy are actively promoted (Fig. 1). Postoperative rehabilitation protocols are prepared for each hospital day, and patient progress is recorded in accordance with these protocols (Fig. 3). The minimum rehabilitation goals include ambulation by postoperative day 3, walking within the ward by postoperative week 1, and initiation of aerobic exercise, such as ergometer training, by postoperative week 2.
In addition, early initiation of enteral nutrition has been reported to be effective in suppressing postoperative weight loss and preventing postoperative pneumonia [14]. In our department, a gastrointestinal fistula, either a gastric tube fistula or jejunostomy, is created in all cases, and early enteral nutrition is initiated on the day of surgery. Enteral nutrition is started with continuous administration of elemental nutrition at a rate of 10 kcal per hour, and the infusion rate is increased daily while carefully monitoring for abdominal symptoms, with a target of 50 kcal per hour by postoperative day 5. To prevent essential fatty acid deficiency, the enteral nutrition formula is switched to a semi-digested preparation rich in n-3 fatty acids around postoperative day 7. During enteral nutrition therapy, bowel movement frequency, consistency, and volume are monitored, and if diarrhea occurs, adjustments to the infusion rate, stool culture testing, and the use of probiotics or antidiarrheal agents are considered as appropriate (Fig. 1) [12].
Before initiating oral intake, swallowing function is evaluated in all cases by rehabilitation specialists using swallowing videofluorography and swallowing endoscopy, and the form of the diet is adjusted and introduced according to swallowing function (Fig. 4). In addition, guidance on eating posture is provided to ensure safe oral intake and prevent aspiration. The amount of enteral nutrition is gradually reduced in accordance with increases in oral intake; however, when oral intake, including ONS, remains insufficient at discharge, enteral nutrition is continued at home after discharge.
With the aging of the population, the average age of patients undergoing esophageal cancer surgery in our department has also increased. For older patients, discharge directly to home after surgery is often difficult, and therefore, in the future, it will be necessary to strengthen inter-hospital cooperation to facilitate home discharge through structured rehabilitation at convalescent hospitals.
Even after discharge, follow-up is continued in cooperation with rehabilitation specialists during outpatient visits. Specifically, physical fitness measurements and evaluations of physical function are conducted at 1, 3, 6, and 12 months after surgery. At the same time, registered dietitians provide outpatient nutritional counseling, assess nutritional intake in the home setting, and offer guidance on oral intake, introduction of ONS products, and enteral nutrition management tailored to individual lifestyles. The treatment diary and WFT are used continuously from the start of intervention until 1 month after discharge.
Results and future issues of perioperative team medicine
We compared short-term outcomes among 137 patients who underwent esophagectomy with gastric tube reconstruction at our hospital between January 2015 and October 2019. Patients were categorized into three groups: before HOPE introduction (n=43), early HOPE period (until April 2018, n=40), and late HOPE period (from April 2018 to October 2019, n=54). When comparing the incidence of infectious complications classified as Clavien-Dindo (C-D) grade III or higher, including anastomotic leakage, pneumonia, and wound infection, no significant difference was observed between the pre-HOPE group and the early HOPE period (18.6% vs. 15.0%). In contrast, the incidence was significantly lower in the late HOPE period compared with the pre-HOPE group (18.6% vs. 5.6%; P=0.001) (Fig. 5). In addition, rates of postoperative weight loss at 1, 3, and 6 months after surgery were significantly improved in both the early and late HOPE periods compared with the pre-HOPE period (Fig. 6) [15].
To examine the effects of using a treatment diary and WFT, 62 patients were selected by propensity score matching from 94 patients who underwent subtotal esophagectomy between 2019 and 2021. Outcomes were compared between the WFT group (n=31) and the non-WFT group (n=31) [12]. The average WFT wearing rate was 91.8%. The incidence of postoperative complications of C-D grade II or higher was significantly lower in the WFT group, and in particular, the incidence of postoperative pneumonia of C-D grade II or higher was significantly reduced (WFT group 16.1% vs. non-WFT group 38.7%; P=0.043) (Table 2) [12]. Postoperative hospital stay was also significantly shorter in the WFT group (median, 22 days vs. 29 days; P=0.012) (Table 2).
Regarding nutritional indicators at 1 month after surgery, serum albumin levels (median, WFT group 3.9 g/dL vs. non-WFT group 3.6 g/dL; P=0.013), serum transthyretin levels (median, WFT group 24.4 mg/dL vs. non-WFT group 19.4 mg/dL; P=0.001), and the prognostic nutritional index (PNI) (median, WFT group 46.2 vs. non-WFT group 42.6; P=0.034) were all significantly higher in the WFT group (Table 2) [16].
Currently, we are conducting a randomized, non-blinded, controlled trial to evaluate the effects of our institution’s preoperative short-term nutrition and exercise therapy program, referred to as the STEP-NEXT (Preoperative Short-Term Program for Nutrition and Exercise Trial), on postoperative nutritional status and physical function following esophagectomy.
Authors’ contribution
Conceptualization: HT. Data curation: YS, KS, TM (Tomohiro Murakami), EB, TM (Tomohiro Matsumoto), HK, YH. Methodology/formal analysis/validation: YS, KS, TM (Tomohiro Murakami), EB, TM (Tomohiro Matsumoto), HK, YH. Project administration: HT. Writing–original draft: RH. Writing–review & editing: RH, YS, KS, TM (Tomohiro Murakami), EB, TM (Tomohiro Matsumoto), HK, YH, HT. All authors read and approved the final manuscript.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
None.
Data availability
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
None.
Supplementary materials
None.
Fig. 1.
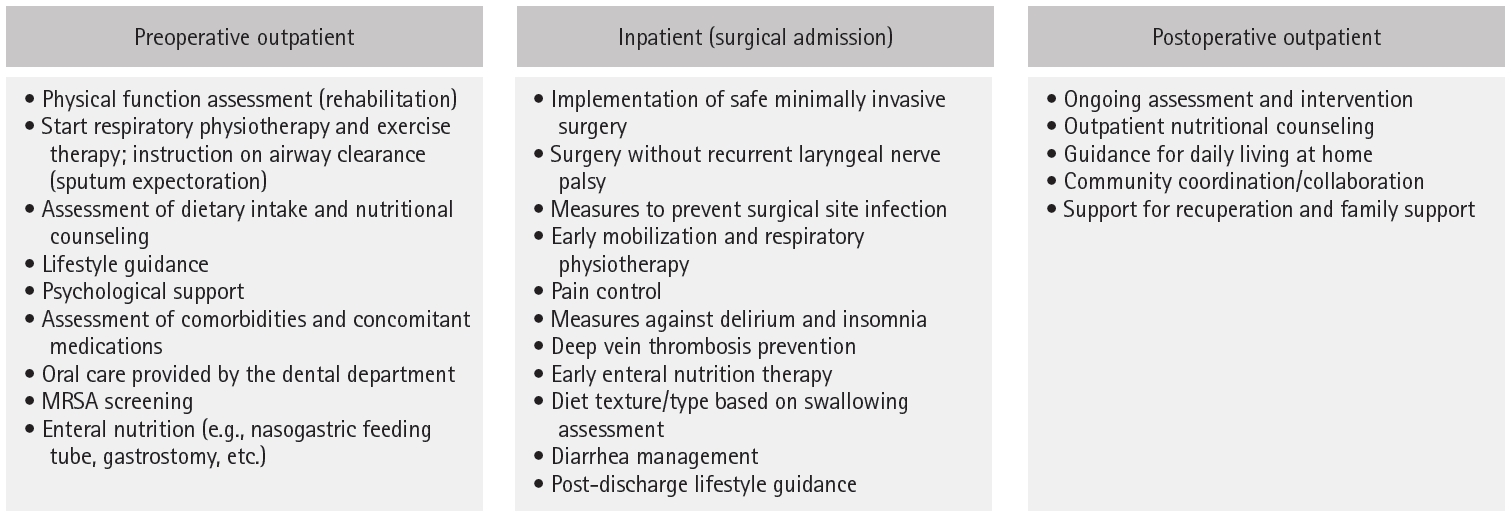
Hamamatsu Perioperative Care Team esophageal cancer perioperative management bundle. MRSA, methicillin-resistant Staphylococcus aureus [12].
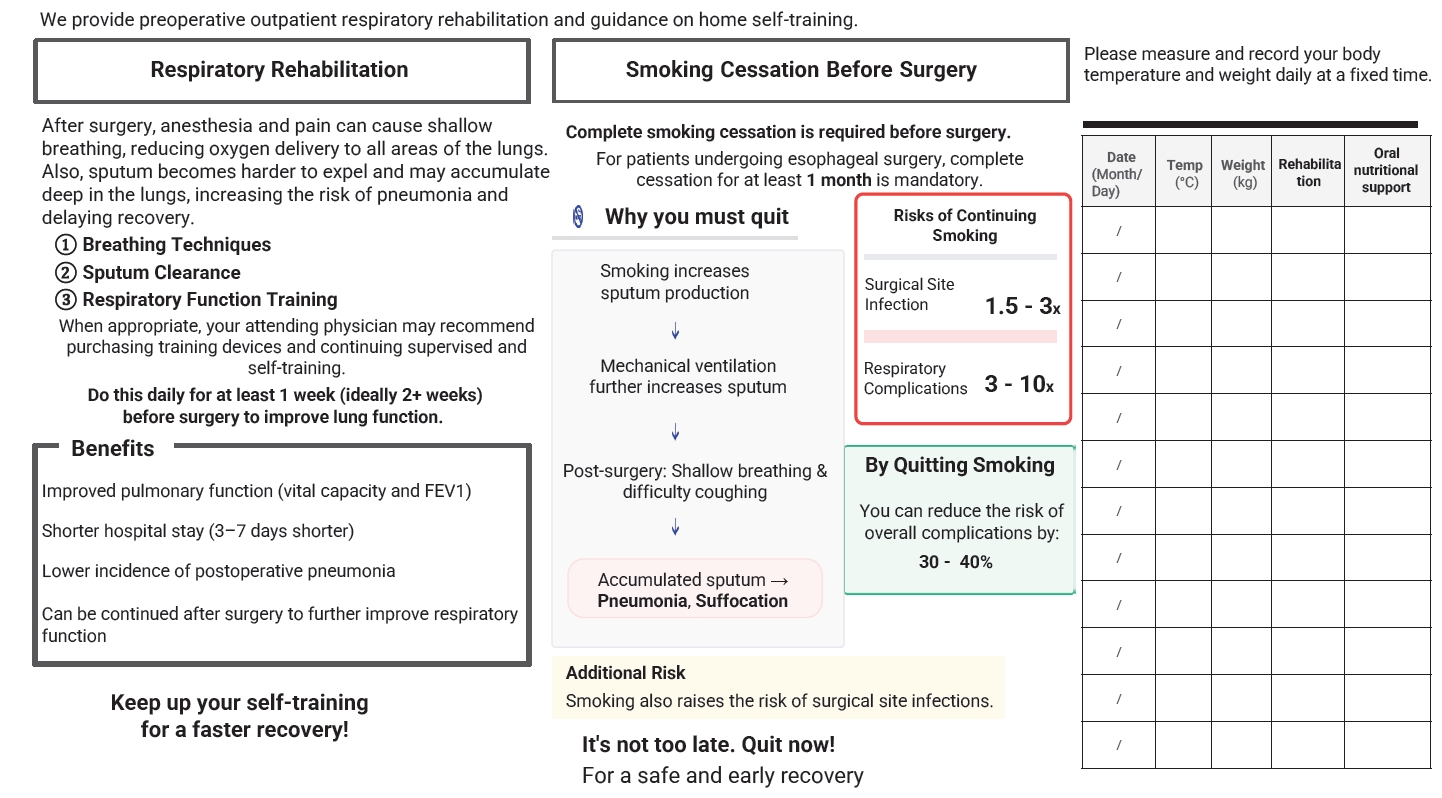
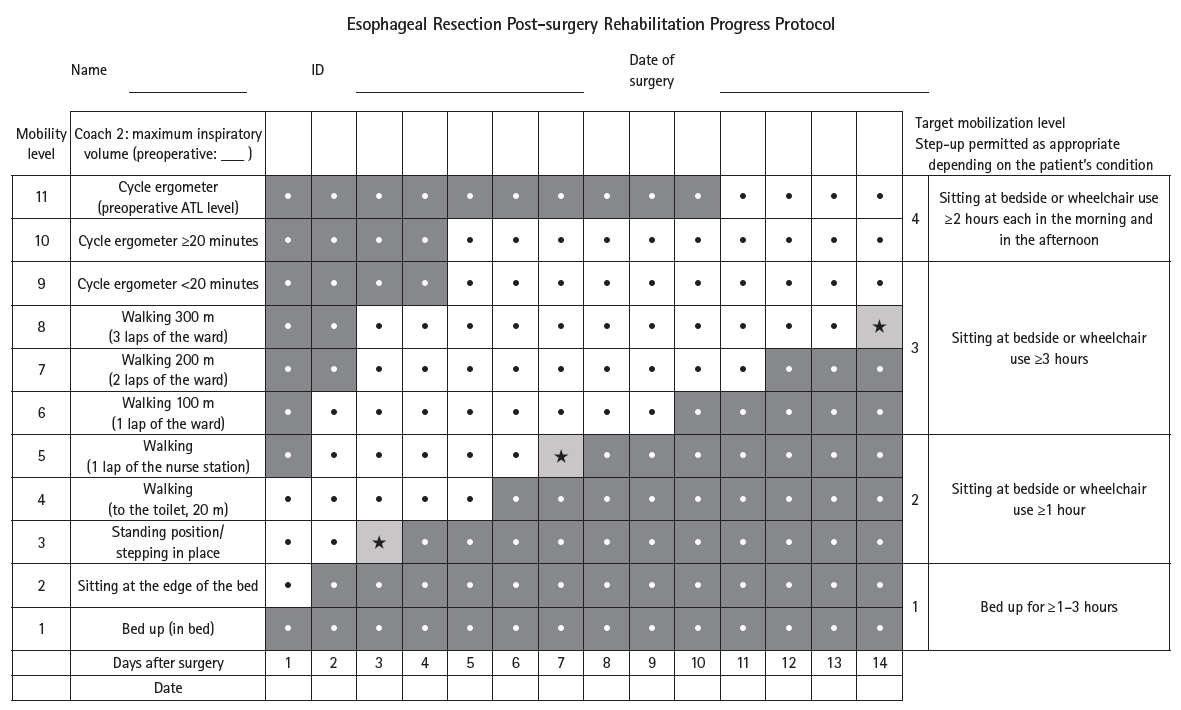
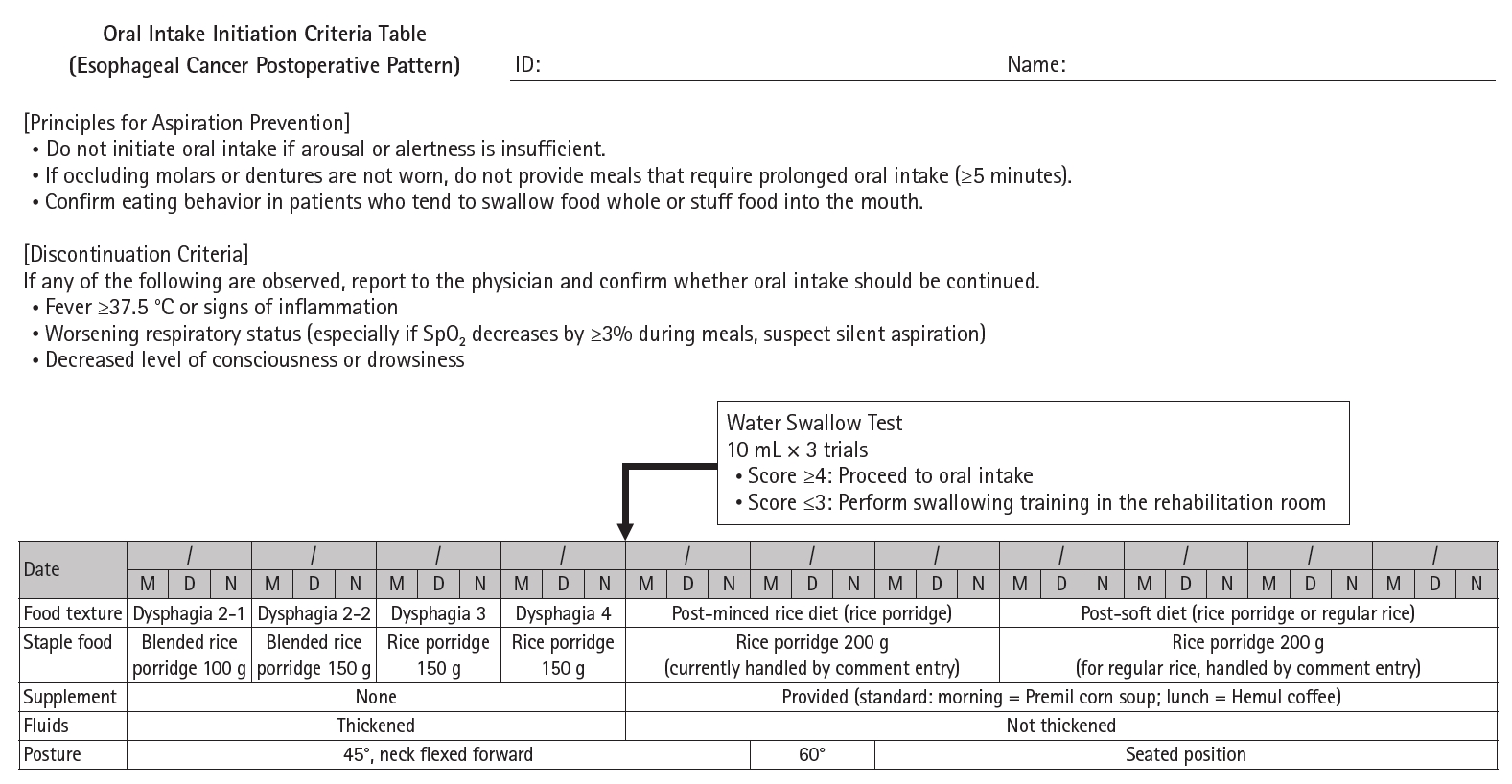
Fig. 5.
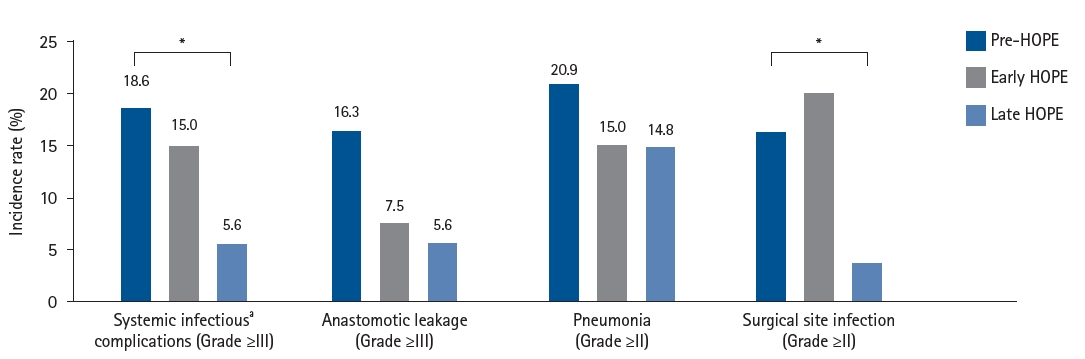
Postoperative complications. Bar graph or table showing the incidence of Clavien-Dindo grade III or higher infectious complications (anastomotic leakage, pneumonia, wound infection) before and after Hamamatsu Perioperative Care Team (HOPE) introduction. aAll complications had been evaluated by Clavien-Dindo classification. *P<0.05.
Fig. 6.
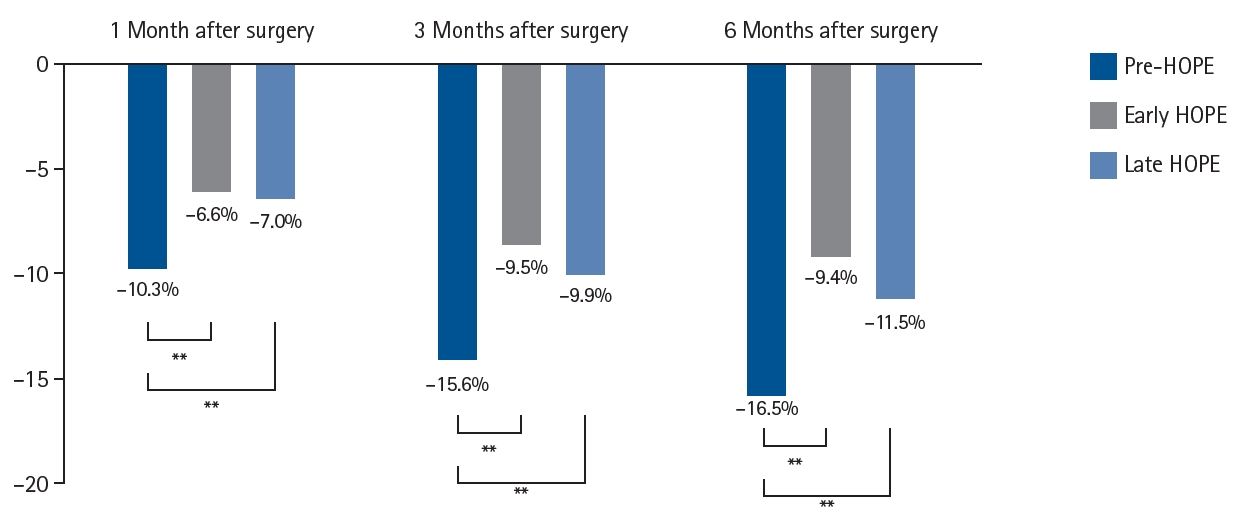
Postoperative weight changes. Line graph or table comparing the percentage of weight loss at 1, 3, and 6 months postoperatively between pre-Hamamatsu Perioperative Care Team (HOPE), early HOPE, and late HOPE groups [15]. **P<0.01.
Table 1.
Perioperative management teams
| Perioperative management team | Author | Preoperative | Postoperative | Outcome |
|---|---|---|---|---|
| PERiO | Shirakawa et al. (2019) [3] | Smoking cessation guidance, physical ability assessment, exercise therapy, oral care | Physical ability assessment, respiratory physiotherapy, basic movement assistance, eating/swallowing rehabilitation | Fewer days to postoperative ambulation, shortened hospital stay, reduced adverse events during preoperative chemotherapy |
| Shirakawa et al. (2021) [4] | ||||
| PeriCan | Watanabe et al. (2016) [5] | Alcohol and smoking cessation guidance, oral care | Early mobilization, rehabilitation, swallowing function assessment, dietary guidance | Reduced pneumonia |
| Perioperative Center | Ochiai (2018) [6] | Patient orientation, oral care, medication adjustment, deep vein thrombosis prevention | Postoperative pain control, oral care | Shortened average hospital stay |
| PMT | Yamamoto and Sakakibara (2023) [7] | Smoking/alcohol cessation guidance, respiratory rehabilitation, nutritional guidance, oral care, skin protection, consultation for use of economic/social resources (post-discharge life support, nursing care, etc.) | Continued postoperative nursing, discharge support, utilization of social resources | Reduced surgery postponement, optimized hospital stays, prevention of complications |
| PMT | Yokoyama (2021) [8] | Physical and social background, patient/family acceptance of surgery, swallowing function assessment, risk of postoperative nausea/vomiting, preoperative pain management plan | Treatment course, evaluation of future PMT interventions, coordination with each committee | Identification of high-risk patients for swallowing disorders |
| Tobu Hospital Patient Support Center | Ishida (2023) [9] | Assessment of dietary intake, nutritional guidance, grip strength/body measurement, calculation of nutritional indices, body composition measurement, prehabilitation (aerobic exercise, resistance exercise, stretching, respiratory training), oral care | Nutritional management, rehabilitation | Increased walking distance, improved sit-and-reach, increased skeletal muscle mass |
| HOPE | Current study (2017) | Physical fitness measurement (rehabilitation), respiratory/physical therapy, sputum discharge guidance, dietary intake assessment/nutritional guidance, lifestyle guidance, psychological care, comorbidity/medication assessment, oral care by dental department, MRSA screening, enteral nutrition (nasal feeding tube, gastrostomy, etc.) | Practice of safe minimally invasive surgery, surgery without recurrent laryngeal nerve palsy, SSI prevention, early mobilization/respiratory physiotherapy, pain control, delirium/insomnia prevention, deep vein thrombosis prevention, early enteral nutrition therapy, dietary form based on swallowing evaluation, management of diarrhea, post-discharge lifestyle guidance | Reduced incidence of atrial fibrillation, reduced pneumonia, increased skeletal muscle mass |
Table 2.
Comparison of short-term outcomes by use of WFTs
- 1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87-108. ArticlePubMedPDF
- 2. Weimann A, Braga M, Harsanyi L, Laviano A, Ljungqvist O, Soeters P, et al. Espen guidelines on enteral nutrition: surgery including organ transplantation. Clin Nutr 2006;25:224-44. ArticlePubMed
- 3. Shirakawa Y, Tanabe S, Fujiwara T. Forefront of perioperative team medicine for esophageal cancer surgery. Nihon Shokakibyo Gakkai Zasshi 2019;116:138-44. ArticlePubMed
- 4. Shirakawa Y, Noma K, Maeda N, Tanabe S, Sakurama K, Sonoyama-Hanaoka A, et al. Early intervention of the perioperative multidisciplinary team approach decreases the adverse events during neoadjuvant chemotherapy for esophageal cancer patients. Esophagus 2021;18:797-805. ArticlePubMedPDF
- 5. Watanabe M, Mine S, Nishida K, Yamada K, Shigaki H, Oya S, et al. Improvement in short-term outcomes after esophagectomy with a multidisciplinary perioperative care team. Esophagus 2016;13:337-42. ArticlePDF
- 6. Ochiai R. The case of Toho University Omori Medical Center Hospital. Jpn J Clin Anaesthesiol 2018;42:1190-8.
- 7. Yamamoto C, Sakakibara S. The evolution of preoperative outpatient care: looking back on the 10 years since its establishment and considering the future of preoperative outpatient care. J Jpn Soc Surg 2023;44:267-71.
- 8. Yokoyama K. Establishment of a perioperative management team in a regional hospital and initiatives for pre- and postoperative swallowing function assessment. J Jpn Soc Surg 2021;42:221-4.
- 9. Ishida T. Perioperative nutritional management by TOPS (Tobu Hospital Patient Support Center). J Jpn Soc Surg 2023;44:129-32.
- 10. Takeuchi H, Ikeuchi S, Kawaguchi Y, Kitagawa Y, Isobe Y, Kubochi K, et al. Clinical significance of perioperative immunonutrition for patients with esophageal cancer. World J Surg 2007;31:2160-7. ArticlePubMedPDF
- 11. Japanese Society for Parenteral and Enteral Nutrition. Guidelines for Parenteral and Enteral Nutrition, 3rd edition [Internet]. Japanese Society for Parenteral and Enteral Nutrition; 2014. [cited 2023 Jan 1]. Available from: https://files.jspen.or.jp/2014/04/201404QR_guideline.pdf
- 12. Haneda R, Hiramatsu Y, Kawata S, Soneda W, Booka E, Murakami T, et al. Clinical impact of diarrhea during enteral feeding after esophagectomy. Int J Clin Oncol 2024;29:36-46. Article
- 13. Sato H, Miyawaki Y, Fujiwara N, Sakuramoto S, Okamoto M, Yamaguchi S, et al. Exercise therapy in esophageal surgery. Surg Metab Nutr 2018;52:289-93.ArticlePubMedPDF
- 14. Takesue T, Takeuchi H, Ogura M, Fukuda K, Nakamura R, Takahashi T, et al. A prospective randomized trial of enteral nutrition after thoracoscopic esophagectomy for esophageal cancer. Ann Surg Oncol 2015;22(Suppl 3):S802-9. ArticlePubMedPDF
- 15. Kawata S, Hiramatsu Y, Shirai Y, Watanabe K, Nagafusa T, Matsumoto T, et al. Multidisciplinary team management for prevention of pneumonia and long-term weight loss after esophagectomy: a single-center retrospective study. Esophagus 2020;17:270-8. ArticlePubMedPMCPDF
- 16. Honke J, Hiramatsu Y, Kawata S, Booka E, Matsumoto T, Morita Y, et al. Usefulness of wearable fitness tracking devices in patients undergoing esophagectomy. Esophagus 2022;19:260-8. ArticlePubMedPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
Cite- Figure
-
Effectiveness of perioperative rehabilitation and nutrition in esophageal cancer: a narrative review
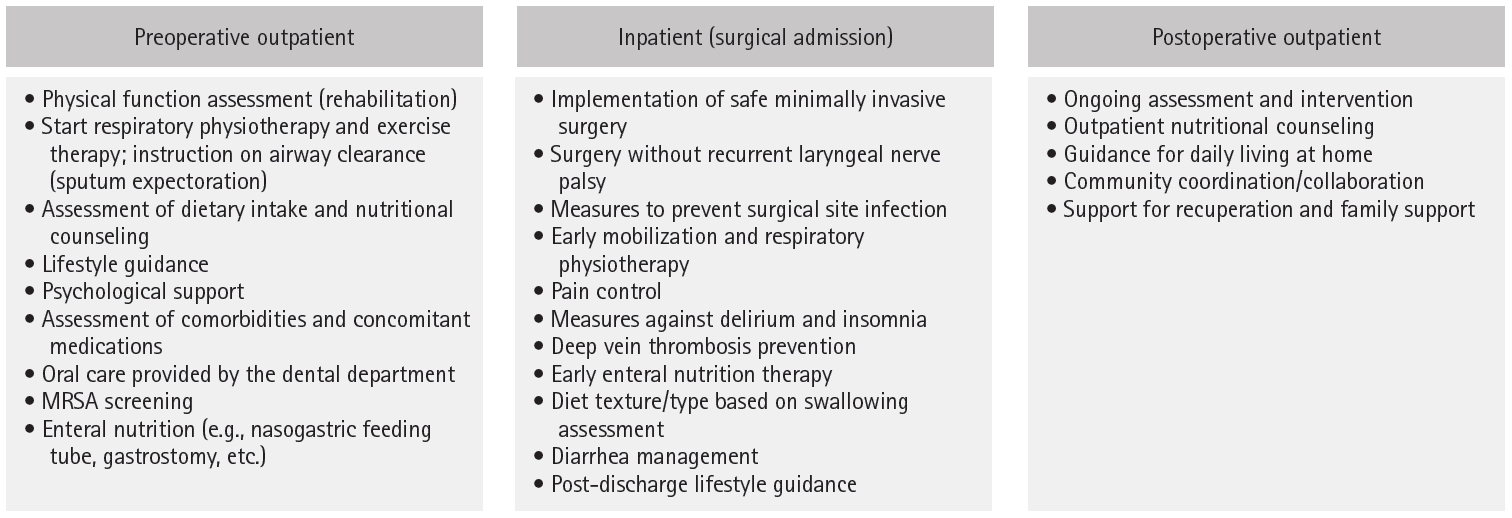
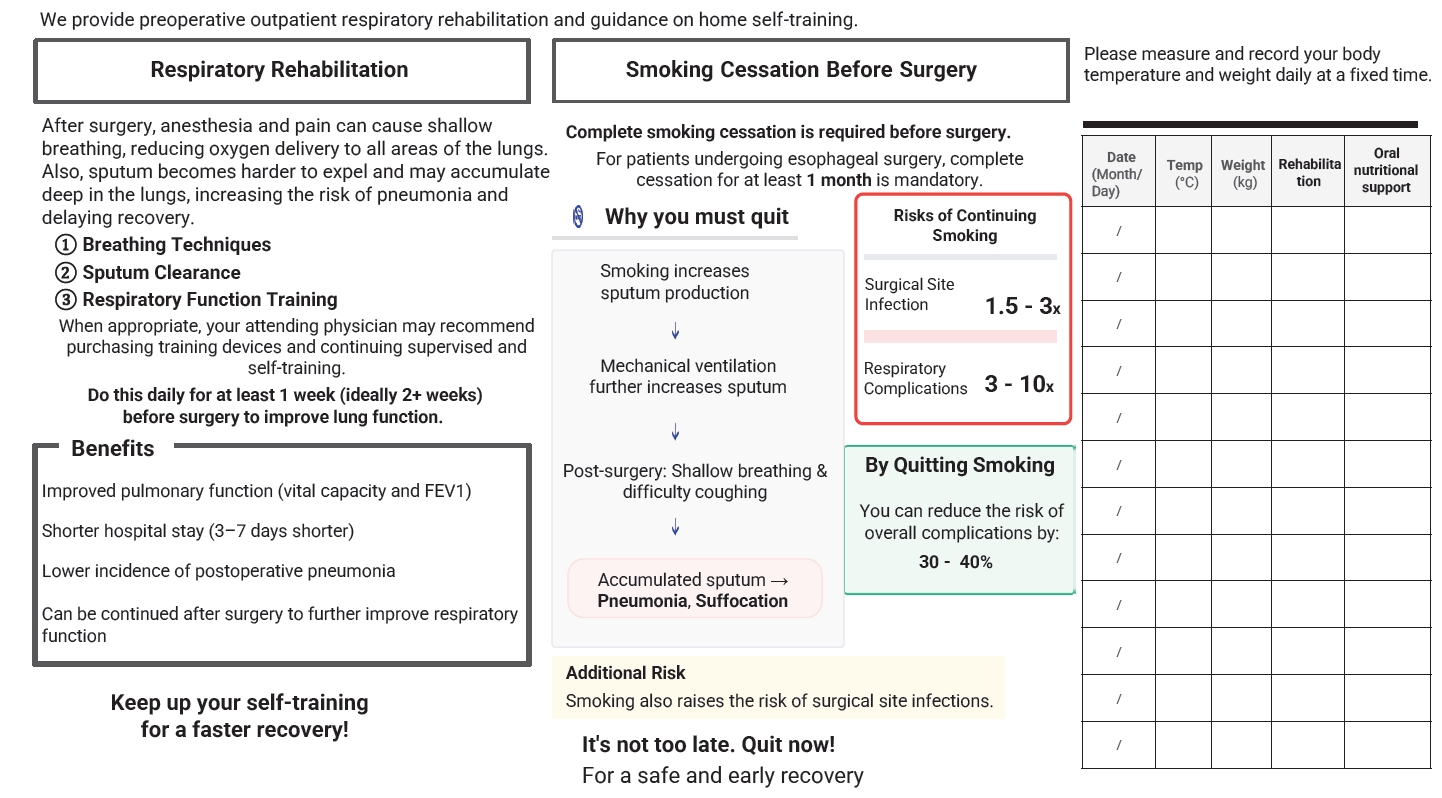
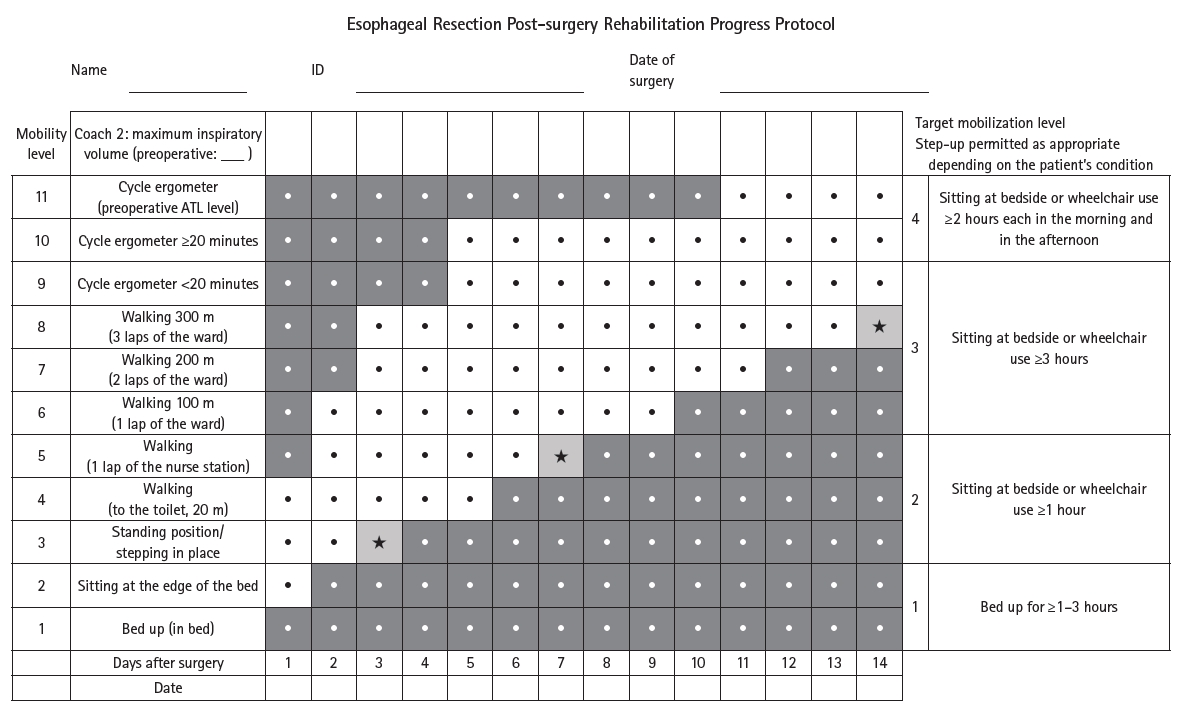
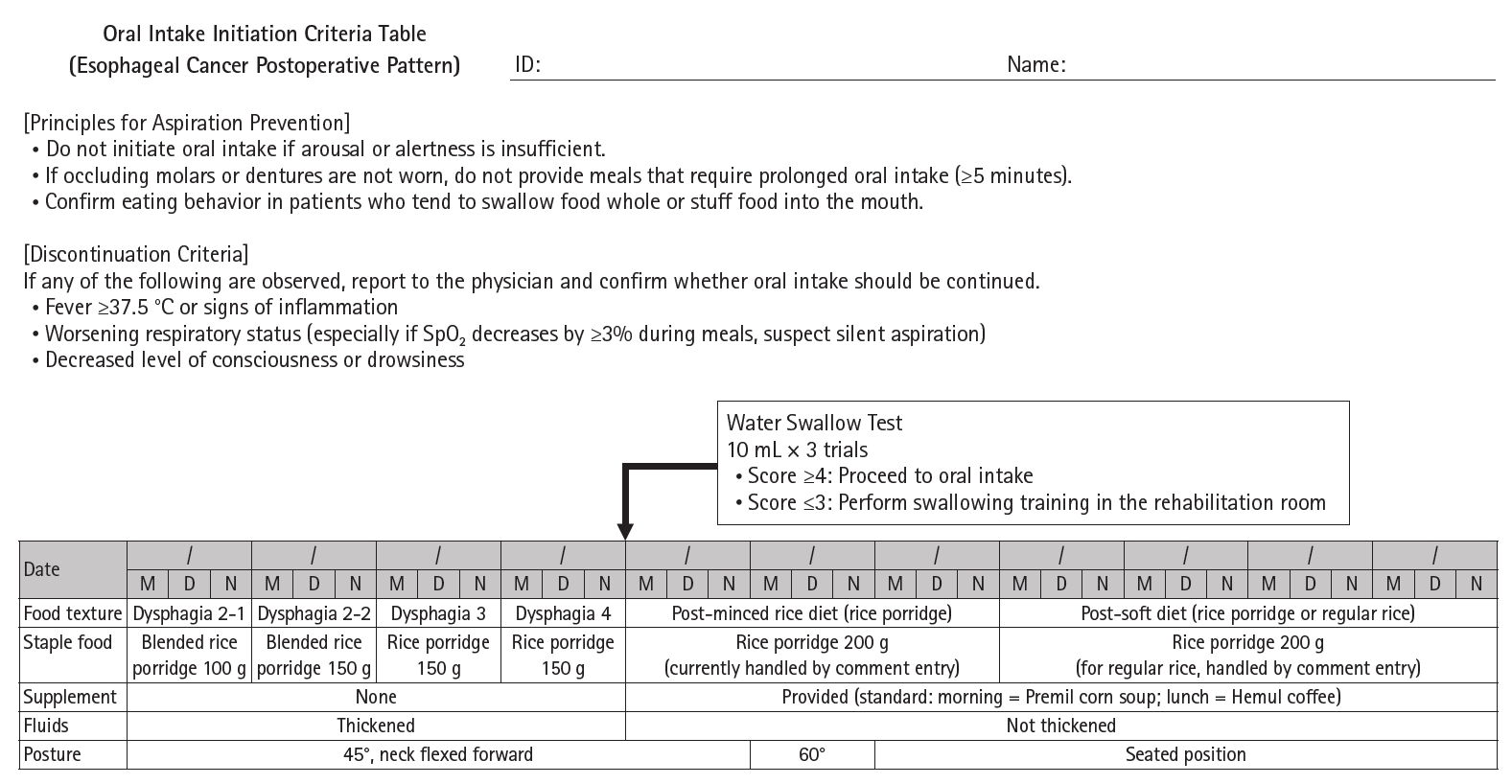
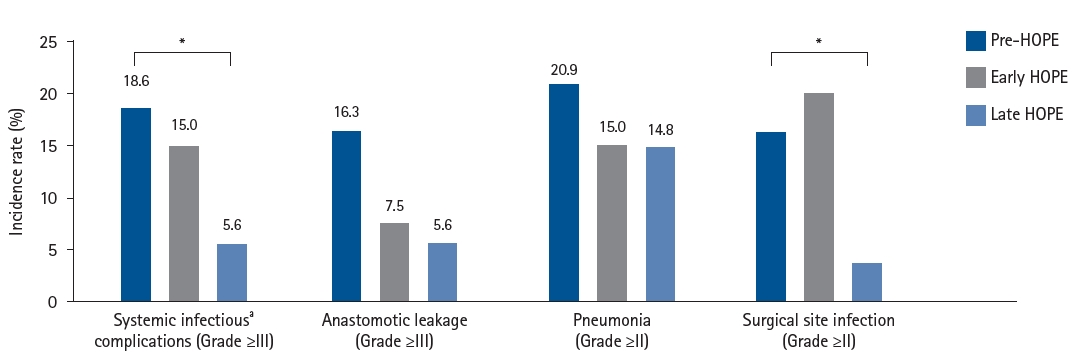
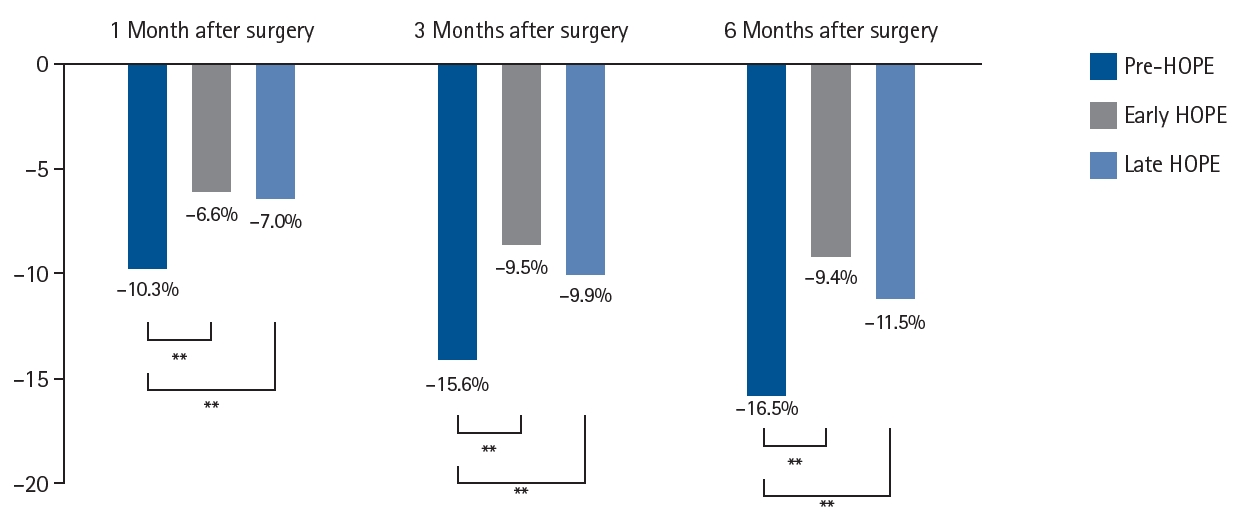
Fig. 1. Hamamatsu Perioperative Care Team esophageal cancer perioperative management bundle. MRSA, methicillin-resistant Staphylococcus aureus [12].
Fig. 2. Treatment diary example.
Fig. 3. Rehabilitation protocol after esophagectomy.
Fig. 4. Hamamatsu Perioperative Care Team oral intake protocol.
Fig. 5. Postoperative complications. Bar graph or table showing the incidence of Clavien-Dindo grade III or higher infectious complications (anastomotic leakage, pneumonia, wound infection) before and after Hamamatsu Perioperative Care Team (HOPE) introduction. aAll complications had been evaluated by Clavien-Dindo classification. *P<0.05.
Fig. 6. Postoperative weight changes. Line graph or table comparing the percentage of weight loss at 1, 3, and 6 months postoperatively between pre-Hamamatsu Perioperative Care Team (HOPE), early HOPE, and late HOPE groups [15]. **P<0.01.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Effectiveness of perioperative rehabilitation and nutrition in esophageal cancer: a narrative review
| Perioperative management team | Author | Preoperative | Postoperative | Outcome |
|---|---|---|---|---|
| PERiO | Shirakawa et al. (2019) [3] | Smoking cessation guidance, physical ability assessment, exercise therapy, oral care | Physical ability assessment, respiratory physiotherapy, basic movement assistance, eating/swallowing rehabilitation | Fewer days to postoperative ambulation, shortened hospital stay, reduced adverse events during preoperative chemotherapy |
| Shirakawa et al. (2021) [4] | ||||
| PeriCan | Watanabe et al. (2016) [5] | Alcohol and smoking cessation guidance, oral care | Early mobilization, rehabilitation, swallowing function assessment, dietary guidance | Reduced pneumonia |
| Perioperative Center | Ochiai (2018) [6] | Patient orientation, oral care, medication adjustment, deep vein thrombosis prevention | Postoperative pain control, oral care | Shortened average hospital stay |
| PMT | Yamamoto and Sakakibara (2023) [7] | Smoking/alcohol cessation guidance, respiratory rehabilitation, nutritional guidance, oral care, skin protection, consultation for use of economic/social resources (post-discharge life support, nursing care, etc.) | Continued postoperative nursing, discharge support, utilization of social resources | Reduced surgery postponement, optimized hospital stays, prevention of complications |
| PMT | Yokoyama (2021) [8] | Physical and social background, patient/family acceptance of surgery, swallowing function assessment, risk of postoperative nausea/vomiting, preoperative pain management plan | Treatment course, evaluation of future PMT interventions, coordination with each committee | Identification of high-risk patients for swallowing disorders |
| Tobu Hospital Patient Support Center | Ishida (2023) [9] | Assessment of dietary intake, nutritional guidance, grip strength/body measurement, calculation of nutritional indices, body composition measurement, prehabilitation (aerobic exercise, resistance exercise, stretching, respiratory training), oral care | Nutritional management, rehabilitation | Increased walking distance, improved sit-and-reach, increased skeletal muscle mass |
| HOPE | Current study (2017) | Physical fitness measurement (rehabilitation), respiratory/physical therapy, sputum discharge guidance, dietary intake assessment/nutritional guidance, lifestyle guidance, psychological care, comorbidity/medication assessment, oral care by dental department, MRSA screening, enteral nutrition (nasal feeding tube, gastrostomy, etc.) | Practice of safe minimally invasive surgery, surgery without recurrent laryngeal nerve palsy, SSI prevention, early mobilization/respiratory physiotherapy, pain control, delirium/insomnia prevention, deep vein thrombosis prevention, early enteral nutrition therapy, dietary form based on swallowing evaluation, management of diarrhea, post-discharge lifestyle guidance | Reduced incidence of atrial fibrillation, reduced pneumonia, increased skeletal muscle mass |
| WFT use (n=31) | No WFT use (n=31) | P-value | |
|---|---|---|---|
| All complications, No. (%) | |||
| C-D grade II or higher | 5 (16.1) | 12 (38.7) | 0.043 |
| Anastomotic leakage | 3 (9.7) | 2 (6.5) | 0.500 |
| Pneumonia | 0 | 7 (22.6) | 0.005 |
| Postoperative hospital stay (day), median (range) | 22 (20–29) | 29 (24–36) | 0.012 |
| Blood test results at 1 month after surgery, median (range) | |||
| Prognostic nutritional index | 46.2 (40.8–49.7) | 42.6 (37.8–45.9) | 0.034 |
| Albumin (g/dL) | 3.9 (3.6–4.1) | 3.6 (3.2–3.9) | 0.013 |
| Transthyretin (mg/dL) | 24.4 (21.5–26.0) | 19.4 (15.0–22.9) | 0.001 |
| CRP (mg/dL) | 0.14 (0.09–0.31) | 0.35 (0.15–1.60) | 0.018 |
Table 1. Perioperative management teams
PERiO, Perioperative Management Center; PeriCan, Perioperative Team at the Cancer Institute Hospital; PMT, Perioperative Management Team; MRSA, methicillin-resistant
Table 2. Comparison of short-term outcomes by use of WFTs
WFTs, wearable fitness tracking devices; C-D, Clavien-Dindo classification; CRP, C-reactive protein.

