 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > J Clin Nutr > Volume 7(2); 2015 > Article
- Original Article Clinical Application of Bioelectrical Impedance Analysis and its Phase Angle for Nutritional Assessment of Critically III Patients
- Hyung-Sook Kim1, Eun Sook Lee1, Yeon Joo Lee2,3, Jae Ho Lee2, Choon-Taek Lee2, Young-Jae Cho2
- 중환자에서 영양상태 평가지표로서 생체전기 임피던스를 이용한 위상 각의 활용
- 김형숙1, 이은숙1, 이연주2,3, 이재호2, 이춘택2, 조영재2
-
Journal of the Korean Society for Parenteral and Enteral Nutrition 2015;7(2):54-61.
DOI: https://doi.org/10.15747/jcn.2015.7.2.54
Published online: August 31, 2015
Department of Pharmacy, Seoul National University Bundang Hospital, Seongnam, Korea
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
Interdepartment of Critical Care Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- Correspondence to Young-Jae Cho Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Bundang Hospital, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 463-707, Korea Tel: +82-31-787-7058, Fax: +82-31-787-4034, E-mail: lungdrcho@snubh.org
• Received: April 8, 2015 • Revised: July 2, 2015 • Accepted: July 6, 2015
Copyright: © Korean Society for Parenteral and Enteral Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,757 Views
- 22 Download
- 3 Crossref
Abstract
-
Purpose: Phase angle (PA) is objectively determined from resistance and reactance measured by bioelectrical impedance analysis (BIA)−a quick, noninvasive method. The aim of this study was to evaluate the clinical application of PA by BIA for nutritional assessment of critically ill patients.
-
Methods: Eighty nine adult patients admitted to a medical intensive care unit (ICU) of a tertiary academic hospital from August 2012 to September 2013 were analyzed. PA values were measured by direct segmental multi-frequency BIA. As traditional nutrition assessment tools, body mass index (BMI), serum albumin levels, total lymphocyte counts, and our hospital’s nutrition screening index (NSI) were also recorded. Correlations between the results of BIA and other traditional parameters were analyzed.
-
Results: PA showed correlation with traditional nutritional parameters, including BMI (r=0.479), serum albumin (r=0.347), and NSI score (r=0.483). Patients with PA lower than the median value (3.5°) had significantly lower nutritional status, increased duration of mechanical ventilation (P=0.039), and increased length of ICU stay (P=0.041).
-
Conclusion: PA, as a reflection of body cell mass, measured by BIA could be a potentially useful parameter for nutritional assessment in critically ill patients.
INTRODUCTION
Nutritional assessment remains an important tool in treating critically ill patients; however, it is often an overlooked aspect in critical care management. Thus far, no single best method or gold standard is available for the nutritional evaluation of critically ill patients. In the clinical setting, existing methods of nutritional evaluation may be subjective (clinical history and nutritional physical examination) or objective (food diary, anthropometry, and biochemical studies).1 Although many prediction equations to assess nutritional status have been reported, the application of the traditional tools of nutritional assessment in critically ill patients is not appropriate, given their acute phase conditions and complex clinical responses.2
Recently, bioelectrical impedance analysis (BIA) has been introduced as a fast, noninvasive, painless, relatively inexpensive, and reproducible method of evaluating body compartments.3-6 Previous studies have shown that variations in the state of hydration of the patient are the main limitation of BIA that uses two-compartment modeling techniques.7 Unlike conventional BIA equipment that often takes only partial measurements and therefore relies upon formulas to estimate whole body composition, the current BIA based by the direct segmental multi-frequency (DSM) technique measures impedance directly from each segments of the body, assuming human body divided into five-segments.8 In body-composition assessment, DSM technique uses six spectra of electrical frequencies to predict the intracellular water and extracellular water (ECW) compartments of the total body water (TBW) in five-segments. Thus, DSM-BIA is a valid tool for the assessment of total body and segmental body composition in the quantification of body cell mass (BCM).
BCM is defined as the fat free mass (FFM) without the bone mineral mass and ECW; it is a marker for the combination of visceral and somatic protein deposits, i.e., the most metabolically active compartment of the body.9 Besides BCM, the phase angle (PA) in BIA is directly determined from resistance (R) and reactance (Xc) without using equations and is known to reflect BCM.10 A smaller PA is known to be consistent with low reactance, cell death, or disruption of the cell membrane’s selective permeability, while a greater PA is compatible with high reactance and larger quantities of intact cell membranes.
The present study aimed to evaluate the clinical application of PA measured by BIA in assessing nutritional status in critically ill patients.
MATERIALS AND METHODS
This study was conducted between August 2012 and September 2013 and recruited 131 patients aged 18 years and older admitted to the medical intensive care unit (ICU) of a tertiary, academic hospital. BIA was conducted for the patients except with a pacemaker or implanted cardiac defibrillator within 48 hours of ICU admission and their clinical characteristics were recorded retrospectively. The following criteria were used to exclude subjects: patients with serious errors in their BIA results, patients who stayed within 48 hours in ICU. Finally 89 patients were included in this study. The correlation between the results of traditional nutritional assessment tools and BIA parameters was analyzed; furthermore, we analyzed the relationships between BIA parameters and various clinical outcomes, including the length of ICU stay, duration of mechanical ventilation, and ICU mortality in the surviving patients.
Data regarding patient’s age, sex, body mass index (BMI), albumin, total lymphocyte count (TLC), duration of mechanical ventilation, length of ICU stay, and ICU mortality were obtained from electronic medical records. Nutritional status was evaluated using our hospital’s nutrition screening index (NSI) (Table 1).11 This index was calculated according to the following equations.
Table 1
Coding of nutrition screeing index
| Coding | Albumin (in mg/dL) | TLC (mm3) | BMI (kg/m2) | Age (y) |
|---|---|---|---|---|
| 1 | <3.5 | <900 | <18.5 | >65 |
| 2 | ≥3.5 | ≥900 | ≥18.5 | ≤65 |
These equations describe the empiric assessment of nutritional status (NSI score<8.75 indicates malnourished patients) in our hospital.11 Following NSI assessment, an enteral or parenteral nutritional regimen was started for each patient and adjusted on the basis of clinical status, nitrogen balance, and various laboratory and nutritional indices.
DSM-BIA was performed by using the InBody S10 (Biospace Co., Seoul, Korea). This device consists of the use of eight electrodes attached to the arms, legs, trunk through six different frequencies (1, 5, 50, 250, 500, and 1,000 kHz) to measure impedance. This equipment has previously been shown to have high test-pretest reliability and accuracy.12 Patients were measured in a supine position on the bed with arms and legs abducted from the body. Source and sensor electrodes were placed on the thumb and index finger of both hands and on each ankle. Before attaching the electrodes, contact areas cleaned using alcohol. The PA (θ) values were obtained from the resistance (R) and reactance (Xc) using the following equation:
As most previous studies have referred to PA values obtained at 50 kHz,13 a further analysis of PA at 50 kHz was also performed in this study. To determine whether PA and patient outcomes were improved by nutritional therapy, BIA measurements were repeated in 15 clinically stable patients before and after nutritional treatment.
Statistical analysis was carried out using the software package IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Normally distributed continuous variables were compared using paired and unpaired t-tests. Non-normally distributed variables were compared by Mann-Whitney U-test. Categorical variables were compared using the chisquare test. Pearson’s correlation was calculated to assess the relationship between variables. Repeated measures ANOVA was used to establish changes in PA and nutritional markers divided according to the ratio of nutritional support calorie and basal metabolic rate (BMR) predicted by BIA in the clinically stable patients who underwent repeated BIA. A P-value <0.05 was considered statistically significant.
The study protocol was approved by the Institutional Review Board Committee of Seoul National University Bundang Hospital (IRB No. B-1310- 224-112). Informed was waived by the IRB.
RESULTS
The demographic and nutritional parameters as well as the clinical variables of 89 patients are showed in Table 2; at the time of ICU admission, 40.4% of the patients were classified as “malnutrition status” based on the NSI score.
Table 2
Clinical characteristics of subjects and nutritional functional variables: initially measured group (n=89)
| Characteristic | Initially measured group |
|---|---|
| Age (y) | 65.2±14.5 |
| Sex (male/female) | 63/26 |
| APACHE II score | 20.1±9.53 |
| Nutritional variables | |
| NSI score | 9.3±1.5 |
| Malnourished according to NSI score | 36 (40.4) |
| Actual body weight (kg) | 59.1±11.4 |
| Body mass index (kg/m2) | 22.1±3.6 |
| Albumin (mg/dL) | 3.3±0.7 |
| Total lymphocyte count (mm3) | 1,240.1±905.8 |
| Phase angle (o) | 3.7±1.4 |
| Fat-free mass (kg) | 48.2±9.9 |
| Body cell mass (kg) | 30.3±6.6 |
| ICU admission diagnosis | |
| Respiratory | 47 (52.8) |
| Cardiovascular | 17 (19.1) |
| Sepsis | 15 (16.9) |
| Gastrointestinal | 4 (4.5) |
| Trauma | 1 (1.1) |
| Other | 5 (5.6) |
| Clinical variables | |
| Duration of mechanical ventilation (d)a | 6.4±12.2 |
| Length of ICU stay (d)a | 9.4±13.5 |
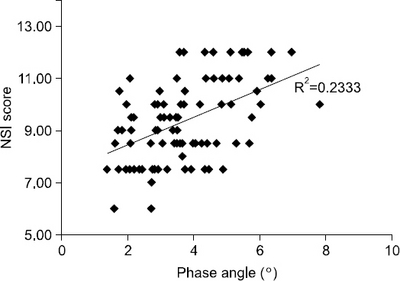
A significant correlation was observed between the markers of traditional nutritional assessment and PA or BCM (Table 3). PA showed a positive correlation with actual body weight (r=0.509, P<0.001), albumin (r=0.347, P<0.001), and TLC (r=0.225, P=0.034). Fig. 1 showed the correlation of PA with NSI scores (r=0.483, P<0.001) and BMI (r=0.479, P<0.001; not be showed in Fig. 1). Although BCM was also correlated with NSI scores (r=0.297, P= 0.005), its correlation coefficient was lower than that for PA.
Table 3
Correlations between phase angle (PA), body cell mass (BCM), and nutritional markers
The median PA was 3.5°, ranging from 1.4° to 7.8°. Overall, 44 patients (49.4%) were observed to have PA ≤3.5°. Age, NSI score, actual body weight, BMI, albumin, TLC, and FFM differed significantly between the groups with a PA value above and below the median PA. Patients with PA ≤3.5° were more malnourished than those with PA >3.5° (43.2 vs. 37.8%, P=0.669). Moreover, of the ICU survival patients (n=66), patients with PA ≤3.5° showed significantly longer duration of mechanical ventilation and ICU stay than those with PA >3.5° (Table 4).
Table 4
Nutritional, functional, and clinical variables in all patients (n=89) divided according to the median value of the phase angle (3.5×)
| PA ≤3.5× (n=44) | PA >3.5× (n=45) | P-value | |
|---|---|---|---|
| Age (y) | 70.3±3.7 | 60.2±13.7 | 0.001 |
| Sex (male/female) | 29/15 | 34/11 | 0.358 |
| APACHE II score | 22.7±10.5 | 17.5±7.8 | 0.010 |
| Nutritional variables | |||
| NSI score | 8.8±1.3 | 9.9±1.6 | <0.001 |
| Malnourished according to NSI score (%) | 19 (43.2) | 17 (37.8) | 0.669 |
| Phase angle (o) | 2.6±0.6 | 4.8±1.0 | <0.001 |
| Actual body weight (kg) | 55.0±9.8 | 63.0±11.5 | 0.001 |
| Body mass index (kg/m2) | 20.9±3.6 | 23.3±3.2 | 0.001 |
| Albumin (mg/dL) | 3.1±0.6 | 3.5±0.7 | 0.005 |
| Total lymphocyte count (mm3) | 1,076.0±743.9 | 1,400.6±1,023.1 | 0.090 |
| Fat-free mass (kg) | 44.8±8.2 | 51.6±10.3 | 0.001 |
| Clinical variables | |||
| ICU mortality (%) | 14 (31.8) | 9 (20.0) | 0.151 |
| Length of ICU stay (d)a | 9.9±9.7 | 5.9±5.6 | 0.041 |
| Duration of mechanical ventilation (d)a | 6.5±9.3 | 2.8±4.3 | 0.039 |
The patients who underwent repeated BIA with nutritional management were divided into two groups according to the ratio between nutritional caloric support and the BMR (Table 5). Of these patients, the mean PA decreased who supported the ratio of nutritional caloric support (NCS):BMR below 1 in contrast to those above 1. During the period of nutritional management, the PA decreased in 4 of 6 patients who supported the ratio of NCS:BMR below 1 (Fig. 2). The ICU survival rate among patients who supported the ratio of NCS:BMR above 1 was higher, however, this was not statistically significant. Except for PA, nearly all the nutritional markers decreased in both the groups despite nutritional management.
Table 5
The changes in phase angle and nutritional markers divided according to the ratio of nutritional caloric support (NCS) to the basal metabolic rate (BMR) (ratio=1) in the repeated BIA group
Fig. 2
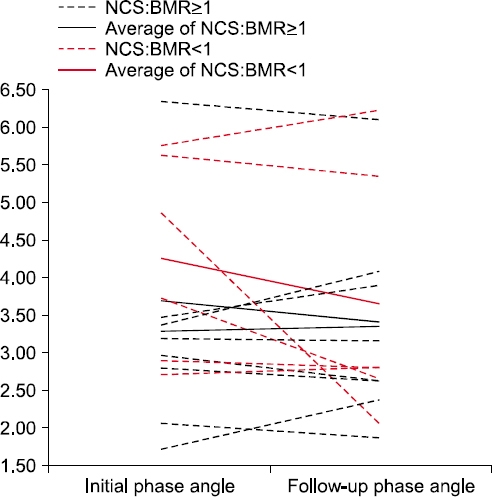
Changes in phase angle after nutritional management in the repeated bioelectrical impedance analysis (BIA) group. NCS = nutritional caloric support; BMR = basal metabolic rate.
DISCUSSION
The findings of the present study indicate that PA, as measured by DSM-BIA, may be useful in assessment of nutritional status in critically ill patients. Further, PA appears to be a valuable parameter for the nutritional assessment in such patients before and after nutritional treatment. PA, in addition to standard laboratory evaluations and clinical judgment, could provide objective information for guiding clinicians in monitoring and optimizing nutritional regimens in critically ill patients.
Available literature supports that increasing nutrient provision in the early phase of critical illness, in order to minimize protein energy deficit, may improve clinical outcomes, particularly in lean and obese patients.14 A precise nutrition assessment is needed for an efficient of nutritional support and prevent the possible problems due to inadequate feeding(infection, poor healing, prolongation of duration of mechanical ventilation etc.).15-17 Recently, BIA has been used for nutritional assessment in variable patients and PA investigated as a prognostic instrument for assessing cell membrane function under various clinical conditions.18,19 Several studies have found PA to be a strong prognostic indicator and an important tool for assessing the clinical condition and for monitoring disease progress in patients undergoing peritoneal dialysis or with human immunodeficiency virus-positive status and colon or pancreatic cancer.20-23 However, few researchers have published data on the utility of PA measured by BIA in the management of critically ill patients.24 In this study, we evaluated nutritional status objectively using PA measured by BIA, not using traditional, unreliable parameters or equations, in critically ill patients and showed the possibility of its clinical implication.
The objectivity of PA is certified by directly measuring the value of R and Xc in the body as mentioned previously in which Xc represents the cell membrane (acts as a capacitor), and R represents the TBW (acts as a conductor). The value of PA is reduced following a decrease in Xc and an increase in R.10 Therefore, PA is considered one of the best indicators of cellular health, where a higher value reflects stronger cell membranes and better cell function.25 By analyzing the changes in both body weight and PA, it is possible to distinguish whether the weight gain due to increase BCM or edema.9 For critically ill patients, it is important to distinguish between simple edema and increases in BCM. The average PA of all subjects in the present study population (3.7±1.4°) was substantially lower than existing reference values, reflecting the fact that these patients were critically ill.1,13
Our findings demonstrated PA to be positively correlated with a number of nutritional markers, such as the actual body weight, BMI, albumin, TLC, our hospital’s NSI score, and FFM. In the ICU, protein markers (albumin, prealbumin, transferrin, etc.) are used to evaluating nutritional status indicator, these values are to be changed when acute phase, therefore do not accurately reflect the alteration of the nutritional status in critically ill patients.1 Further, anthropometric measurements are also not wholly reliable in the assessment of nutrition status or the adequacy of nutrition therapy. However, our findings showed that patients with PA ≤3.5° had significantly impaired nutritional status, increased length of ICU stay, and increased duration of mechanical ventilation. The use of the 3.5° reference value could allow the identification of patients at risk who are in particular need of intensified medical and nutritional attention.
The essential goal of nutritional support is to reach the energy requirements of metabolic disorder, to support the hypermetabolism in critically ill patients, and to minimize protein catabolism.1 The adequate caloires and protein supply to reduce morbidity and mortality in critically ill patients remain controversial.15 One of the most commonly used methods for estimating caloric needs is basal energy requirements that are frequently multiplied by various activity and/or stress factors.26 In contrast, another observational study suggests that feeding fewer than the goal calories, i.e., between 33% and 66% of the estimated energy needs, lead to improved clinical outcomes as compared to outcomes in patients who receive closer to 100% of goal calories.27 Although there are only 15 patients in the repeated BIA group, our data suggests that differences exist in the changes shown by PA and traditional nutritional markers following nutritional management and PA is a possible marker of quantitative changes in body composition and is capable of discriminating between degrees of undernutrition. For long-term nutritional management, PA can be a useful parameter for evaluating the effectiveness of the nutrition regimen.
The limitations of this study include the time points of BIA to measure PA and the retrospective study design. BIA was not performed at certain time points as recommended which may have led to inaccuracies in the data. Rather, BIA was performed during routine clinical ICU admission and these real time measurements are more reflective of its reliability. The cut-off value of PA in this study was generated to divide the patient population into 2 equal and mutually exclusive groups, which does not agree with those reported by other researchers in the field; however, PA reference values for the Korean population are still lacking.17,28-30 Therefore, there is a clear need to define thresholds for PA as a nutritional assessment tool by using receiver operating characteristic analysis based on large, prospective studies in various ethnic groups.24,30 Longitudinal, prospective studies investigating the association between these nutritional markers and clinical outcomes such as hospitalization and mortality should be conducted to clarify such issues.
CONCLUSION
PA, as a reflection of BCM, measured by BIA could be a potentially useful parameter for nutritional assessment in critically ill patients.
- 1. McClave SA, Martindale RG, Vanek VW, McCarthy M, Roberts P, Taylor B, et al. A.S.P.E.N. Board of Directors; American College of Critical Care Medicine; Society of Critical Care Medicine. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2009;33(3):277-316. PubMed
- 2. Jacobs DO. Use of bioelectrical impedance analysis measurements in the clinical management of critical illness. Am J Clin Nutr 1996;64(3 Suppl):498S-502S. ArticlePubMed
- 3. Kyle UG, Unger P, Dupertuis YM, Karsegard VL, Genton L, Pichard C. Body composition in 995 acutely ill or chronically ill patients at hospital admission: a controlled population study. J Am Diet Assoc 2002;102(7):944-55. PubMed
- 4. Thibault R, Pichard C. The evaluation of body composition: a useful tool for clinical practice. Ann Nutr Metab 2012;60(1):6-16. ArticlePubMedPDF
- 5. Thibault R, Genton L, Pichard C. Body composition: why, when and for who? Clin Nutr 2012;31(4):435-47. ArticlePubMed
- 6. Kyle UG, Piccoli A, Pichard C. Body composition measurements: interpretation finally made easy for clinical use. Curr Opin Clin Nutr Metab Care 2003;6(4):387-93. ArticlePubMed
- 7. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Manuel Gómez J, et al. ESPEN. Bioelectrical impedance analysis-part II: utilization in clinical practice. Clin Nutr 2004;23(6):1430-53. PubMed
- 8. Ling CH, de Craen AJ, Slagboom PE, Gunn DA, Stokkel MP, Westendorp RG, et al. Accuracy of direct segmental multifrequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin Nutr 2011;30(5):610-5. ArticlePubMed
- 9. Oliveira CM, Kubrusly M, Mota RS, Silva CA, Choukroun G, Oliveira VN. The phase angle and mass body cell as markers of nutritional status in hemodialysis patients. J Ren Nutr 2010;20(5):314-20. ArticlePubMed
- 10. Gunn SM, Halbert JA, Giles LC, Stepien JM, Miller MD, Crotty M. Bioelectrical phase angle values in a clinical sample of ambulatory rehabilitation patients. Dyn Med 2008;7:14.ArticlePubMedPMCPDF
- 11. Kim S, Kim S, Sohn C. Development of nutrition screening index for hospitalized patients. Korean J Community Nutr 2006;11(6):779-84.
- 12. Gibson AL, Holmes JC, Desautels RL, Edmonds LB, Nuudi L. Ability of new octapolar bioimpedance spectroscopy analyzers to predict 4-component-model percentage body fat in Hispanic, black, and white adults. Am J Clin Nutr 2008;87(2):332-8. ArticlePubMed
- 13. Wirth R, Volkert D, Rösler A, Sieber CC, Bauer JM. Bioelectric impedance phase angle is associated with hospital mortality of geriatric patients. Arch Gerontol Geriatr 2010;51(3):290-4. ArticlePubMed
- 14. Alberda C, Gramlich L, Jones N, Jeejeebhoy K, Day AG, Dhaliwal R, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med 2009;35(10):1728-37. ArticlePubMedPDF
- 15. Villet S, Chiolero RL, Bollmann MD, Revelly JP, Cayeux R N MC, Delarue J, et al. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin Nutr 2005;24(4):502-9. ArticlePubMed
- 16. Rubinson L, Diette GB, Song X, Brower RG, Krishnan JA. Low caloric intake is associated with nosocomial bloodstream infections in patients in the medical intensive care unit. Crit Care Med 2004;32(2):350-7. ArticlePubMed
- 17. Petros S, Engelmann L. Enteral nutrition delivery and energy expenditure in medical intensive care patients. Clin Nutr 2006;25(1):51-9. ArticlePubMed
- 18. Norman K, Stobäus N, Pirlich M, Bosy-Westphal A. Bioelectrical phase angle and impedance vector analysis--clinical relevance and applicability of impedance parameters. Clin Nutr 2012;31(6):854-61. ArticlePubMed
- 19. Kyle UG, Genton L, Pichard C. Low phase angle determined by bioelectrical impedance analysis is associated with malnutrition and nutritional risk at hospital admission. Clin Nutr 2013;32(2):294-9. ArticlePubMed
- 20. Schwenk A, Beisenherz A, Römer K, Kremer G, Salzberger B, Elia M. Phase angle from bioelectrical impedance analysis remains an independent predictive marker in HIV-infected patients in the era of highly active antiretroviral treatment. Am J Clin Nutr 2000;72(2):496-501. ArticlePubMed
- 21. Paiva SI, Borges LR, Halpern-Silveira D, Assunção MC, Barros AJ, Gonzalez MC. Standardized phase angle from bioelectrical impedance analysis as prognostic factor for survival in patients with cancer. Support Care Cancer 2010;19(2):187-92. ArticlePubMedPDF
- 22. Gupta D, Lis CG, Dahlk SL, Vashi PG, Grutsch JF, Lammersfeld CA. Bioelectrical impedance phase angle as a prognostic indicator in advanced pancreatic cancer. Br J Nutr 2004;92(6):957-62. ArticlePubMed
- 23. Gupta D, Lis CG, Dahlk SL, King J, Vashi PG, Grutsch JF, et al. The relationship between bioelectrical impedance phase angle and subjective global assessment in advanced colorectal cancer. Nutr J 2008;7:19.ArticlePubMedPMCPDF
- 24. Berbigier MC, Pasinato VF, Rubin Bde A, Moraes RB, Perry ID. Bioelectrical impedance phase angle in septic patients admitted to intensive care units. Rev Bras Ter Intensiva 2013;25(1):25-31. ArticlePubMedPMC
- 25. Zdolsek HJ, Lindahl OA, Sjöberg F. Non-invasive assessment of fluid volume status in the interstitium after haemodialysis. Physiol Meas 2000;21(2):211-20. ArticlePubMed
- 26. Foster GD, Knox LS, Dempsey DT, Mullen JL. Caloric requirements in total parenteral nutrition. J Am Coll Nutr 1987;6(3):231-53. ArticlePubMed
- 27. Krishnan JA, Parce PB, Martinez A, Diette GB, Brower RG. Caloric intake in medical ICU patients: consistency of care with guidelines and relationship to clinical outcomes. Chest 2003;124(1):297-305. ArticlePubMed
- 28. Schwenk A, Ward LC, Elia M, Scott GM. Bioelectrical impedance analysis predicts outcome in patients with suspected bacteremia. Infection 1998;26(5):277-82. ArticlePubMedPDF
- 29. Norman K, Stobäus N, Zocher D, Bosy-Westphal A, Szramek A, Scheufele R, et al. Cutoff percentiles of bioelectrical phase angle predict functionality, quality of life, and mortality in patients with cancer. Am J Clin Nutr 2010;92(3):612-9. ArticlePubMed
- 30. Bosy-Westphal A, Danielzik S, Dörhöfer RP, Later W, Wiese S, Müller MJ. Phase angle from bioelectrical impedance analysis: population reference values by age, sex, and body mass index. JPEN J Parenter Enteral Nutr 2006;30(4):309-16. ArticlePubMedPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Optimal Enteral Nutrition Support Preserved Muscle Mass in Critically Ill Children
Kantisa Sirianansopa, Chavisa Rassameehirun, Sirinuch Chomtho, Orapa Suteerojntrakool, Lalida Kongkiattikul, Eric Gumpricht
Journal of Nutrition and Metabolism.2022; 2022: 1. CrossRef - Prognostic value of phase angle and bioelectrical impedance vector in critically ill patients: A systematic review and meta-analysis of observational studies
Júlia Lima, Igor Eckert, Maria Cristina Gonzalez, Flávia Moraes Silva
Clinical Nutrition.2022; 41(12): 2801. CrossRef - Bioelectrical Impedance Analysis for Prediction of Early Complications after Gastrectomy in Elderly Patients with Gastric Cancer: the Phase Angle Measured Using Bioelectrical Impedance Analysis
Byunghyuk Yu, Ki Bum Park, Ji Yeon Park, Seung Soo Lee, Oh Kyoung Kwon, Ho Young Chung
Journal of Gastric Cancer.2019; 19(3): 278. CrossRef
 Cite
CiteClinical Application of Bioelectrical Impedance Analysis and its Phase Angle for Nutritional Assessment of Critically III Patients
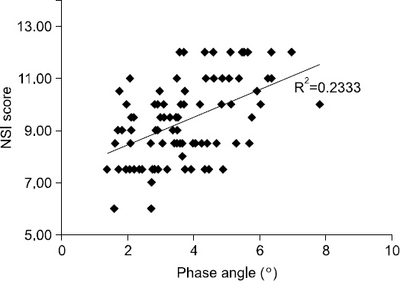
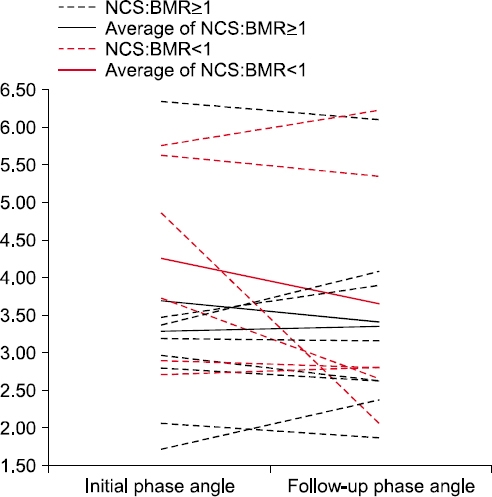
Fig. 1
The relationships between nutrition screening index (NSI) score, and phase angle.
Fig. 2
Changes in phase angle after nutritional management in the repeated bioelectrical impedance analysis (BIA) group. NCS = nutritional caloric support; BMR = basal metabolic rate.
Fig. 1
Fig. 2
Clinical Application of Bioelectrical Impedance Analysis and its Phase Angle for Nutritional Assessment of Critically III Patients
Coding of nutrition screeing index
| Coding | Albumin (in mg/dL) | TLC (mm3) | BMI (kg/m2) | Age (y) |
|---|---|---|---|---|
| 1 | <3.5 | <900 | <18.5 | >65 |
| 2 | ≥3.5 | ≥900 | ≥18.5 | ≤65 |
Clinical characteristics of subjects and nutritional functional variables: initially measured group (n=89)
| Characteristic | Initially measured group |
|---|---|
| Age (y) | 65.2±14.5 |
| Sex (male/female) | 63/26 |
| APACHE II score | 20.1±9.53 |
| Nutritional variables | |
| NSI score | 9.3±1.5 |
| Malnourished according to NSI score | 36 (40.4) |
| Actual body weight (kg) | 59.1±11.4 |
| Body mass index (kg/m2) | 22.1±3.6 |
| Albumin (mg/dL) | 3.3±0.7 |
| Total lymphocyte count (mm3) | 1,240.1±905.8 |
| Phase angle (o) | 3.7±1.4 |
| Fat-free mass (kg) | 48.2±9.9 |
| Body cell mass (kg) | 30.3±6.6 |
| ICU admission diagnosis | |
| Respiratory | 47 (52.8) |
| Cardiovascular | 17 (19.1) |
| Sepsis | 15 (16.9) |
| Gastrointestinal | 4 (4.5) |
| Trauma | 1 (1.1) |
| Other | 5 (5.6) |
| Clinical variables | |
| Duration of mechanical ventilation (d) |
6.4±12.2 |
| Length of ICU stay (d) |
9.4±13.5 |
aICU survival subgroup, n=66.
Correlations between phase angle (PA), body cell mass (BCM), and nutritional markers
| Nutritional marker | PA | BCM | ||
|---|---|---|---|---|
| r | P | r | P | |
| Actual body weight | 0.509 | <0.001 | 0.837 | <0.001 |
| Body mass index | 0.479 | <0.001 | 0.505 | <0.001 |
| Albumin | 0.347 | 0.001 | 0.023 | 0.830 |
| Total lymphocyte count | 0.225 | 0.034 | 0.157 | 0.143 |
| Nutrition screening index score | 0.483 | <0.001 | 0.297 | 0.005 |
Nutritional, functional, and clinical variables in all patients (n=89) divided according to the median value of the phase angle (3.5×)
| PA ≤3.5× (n=44) | PA >3.5× (n=45) | P-value | |
|---|---|---|---|
| Age (y) | 70.3±3.7 | 60.2±13.7 | 0.001 |
| Sex (male/female) | 29/15 | 34/11 | 0.358 |
| APACHE II score | 22.7±10.5 | 17.5±7.8 | 0.010 |
| Nutritional variables | |||
| NSI score | 8.8±1.3 | 9.9±1.6 | <0.001 |
| Malnourished according to NSI score (%) | 19 (43.2) | 17 (37.8) | 0.669 |
| Phase angle (o) | 2.6±0.6 | 4.8±1.0 | <0.001 |
| Actual body weight (kg) | 55.0±9.8 | 63.0±11.5 | 0.001 |
| Body mass index (kg/m2) | 20.9±3.6 | 23.3±3.2 | 0.001 |
| Albumin (mg/dL) | 3.1±0.6 | 3.5±0.7 | 0.005 |
| Total lymphocyte count (mm3) | 1,076.0±743.9 | 1,400.6±1,023.1 | 0.090 |
| Fat-free mass (kg) | 44.8±8.2 | 51.6±10.3 | 0.001 |
| Clinical variables | |||
| ICU mortality (%) | 14 (31.8) | 9 (20.0) | 0.151 |
| Length of ICU stay (d) |
9.9±9.7 | 5.9±5.6 | 0.041 |
| Duration of mechanical ventilation (d) |
6.5±9.3 | 2.8±4.3 | 0.039 |
aICU survival subgroup: PA ≤3.5, n=30; PA >3.5, n=36.
The changes in phase angle and nutritional markers divided according to the ratio of nutritional caloric support (NCS) to the basal metabolic rate (BMR) (ratio=1) in the repeated BIA group
| NCS:BMR ≥1 (n=9) | NCS:BMR <1 (n=6) | P-value | |||
|---|---|---|---|---|---|
| Initial | Post | Initial | Post | ||
| Age (y) | 69.2±12.6 | 60.0±15.6 | 0.228 | ||
| Sex (male/female) | 5/4 | 4/2 | 1.000 | ||
| APACHE II score | 25.0±10.5 | 21.5±8.4 | 0.506 | ||
| DM/liver disease | 3 | 1/2 | 0.758 | ||
| Basal metabolic rate | 1,316.3±165.3 | 1,427.8±227.5 | 0.290 | ||
| Nutritional markers | |||||
| Phase angle (°) | 3.3±1.3 | 3.4±1.3 | 4.2±1.3 | 3.7±1.7 | 0.139 |
| Malnourished according to NSI coding | 2 (22.2) | 5 (55.6) | 2 (33.3) | 3 (50.0) | 1.000 |
| Actual body weight (kg) | 55.1±12.6 | 54.7±12.1 | 61.6±11.9 | 60.8±11.2 | 0.669 |
| Body mass index (kg/m2) | 21.7±5.1 | 21.5±4.9 | 21.9±3.4 | 21.7±3.3 | 0.857 |
| Albumin (mg/dL) | 3.1±0.9 | 2.9±0.4 | 3.5±0.6 | 3.3±0.7 | 0.918 |
| Total lymphocyte count (mm3) | 1,675.3±1,100.9 | 1,488.2±882.8 | 1,265.9±1,252.5 | 1,032.9±806.7 | 0.945 |
| NSI score | 9.3±1.2 | 8.1±1.5 | 9.6±2.0 | 8.8±1.4 | 0.713 |
| Clinical variables | |||||
| ICU survival | 8 (88.9) | 4 (66.7) | 0.525 | ||
Table 1 Coding of nutrition screeing index
Table 2 Clinical characteristics of subjects and nutritional functional variables: initially measured group (n=89)
ICU survival subgroup, n=66.
Table 3 Correlations between phase angle (PA), body cell mass (BCM), and nutritional markers
Table 4 Nutritional, functional, and clinical variables in all patients (n=89) divided according to the median value of the phase angle (3.5×)
ICU survival subgroup: PA ≤3.5, n=30; PA >3.5, n=36.
Table 5 The changes in phase angle and nutritional markers divided according to the ratio of nutritional caloric support (NCS) to the basal metabolic rate (BMR) (ratio=1) in the repeated BIA group

