 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > J Clin Nutr > Volume 7(2); 2015 > Article
- Original Article The Evaluation of Preoperative Oral Carbohydrate-Rich Solution Effects on Insulin Resistance in Patients undergoing Colectomy
- Cherry Ann Sio, Kyuwhan Jung, Seong-Bum Kang, Duk-Woo Kim, Heung-Kwon Oh, Miok Yoon
- 대장절제술 환자에서 수술 전 경구용 Carbohydrate-Rich 음료 복용과 인슐린 저항성 관계
- 시오체리안, 정규환, 강성범, 김덕우, 오흥권, 윤미옥
-
Journal of the Korean Society for Parenteral and Enteral Nutrition 2015;7(2):62-67.
DOI: https://doi.org/10.15747/jcn.2015.7.2.62
Published online: August 31, 2015
Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea
- Correspondence to Kyuwhan Jung Department of Surgery, Seoul National University Bundang Hospital, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 13620, Korea Tel: +82-31-787-7099, Fax: +82-31-787-4078, E-mail: chungq@snubh.org
• Received: August 4, 2015 • Revised: August 21, 2015 • Accepted: August 22, 2015
Copyright: © Korean Society for Parenteral and Enteral Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,940 Views
- 8 Download
- 6 Crossref
Abstract
-
Purpose: Reducing preoperative fasting time showed positive effects in several studies, and current guidelines suggest use of a preoperative oral carbohydrate-rich solution before elective surgeries. For elective colectomy procedures, some surgeons favor two-day bowel preparation with diet restriction and administration of laxatives. Aside from patients experiencing the discomfort of nil per os (NPO), there are reported benefits regarding intake of liquids until at least two hours prior to surgery, including decrease in insulin resistance, without additional postoperative surgical complications. The aim of this study is to show the benefits of administration of oral rehydration solution (ORS) two hours prior to surgery for patients undergoing elective colectomy, particularly postoperative insulin resistance.
-
Methods: This is a randomized controlled trial. All patients undergoing elective colectomy were included and randomized to the control arm or treatment arm. The control arm consisted of the standard bowel preparation and one day of NPO, while the treatment arm consisted of the standard bowel preparation and allowing intake of carbohydrate-rich ORS until 2 hours before surgery. The insulin, glucose, cortisol, and triglyceride levels were determined immediately after induction, 6 hours, 24 hours, and 48 hours post-op, and compared. The homeostatic model assessment-insulin resistance, insulin, glucose, cortisol, and triglyceride levels were determined and compared between the two groups. Anxiety and postoperative complications were monitored and assessed as well.
-
Results: There was less insulin resistance in patients who received ORS 2 hours prior to surgery. Insulin, glucose, cortisol, and triglyceride levels were lower in the treatment group compared to the control group. Taking ORS 1 day prior and until 2 hours before surgery decreased anxiety and discomfort, and alleviated hunger.
-
Conclusion: Regarding complications, there was no difference in the incidence of aspiration and postoperative complications. There were fewer wound complications and incidence of paralytic ileus in the treatment group.
INTRODUCTION
Reducing preoperative fasting time showed positive effects in several studies,1-6 and current guidelines suggest using preoperative oral carbohydrate-rich solution before elective surgeries.6-10 This can reduce postoperative complications and enhance early recovery.
For elective colectomy procedures, some surgeons favor bowel preparation two days prior to the surgery. Osmotic laxatives such as CoLyte (Pendopharm Co., Canada) are administered two days prior, and nil per os (NPO) is required 1 day prior to ensure no fecal residue is left in the bowel. Though it may ensure a cleaner and safer surgery, this longer period of starvation increases insulin resistance and may increase postoperative complications and morbidity.1-4 However, there is evidence that administration of carbohydrate-rich oral rehydration solution (ORS) at least two hours prior to surgery reduces insulin resistance, without increasing postoperative complications.1-4,6
Interplay of many factors can affect the glycemic state and insulin resistance in patients, especially those undergoing major abdominal surgery. We need to optimize preoperative care and preparation to prevent complications and enhance recovery, and this is one of the many points emphasized in Enhanced Recovery after Surgery (ERAS) protocol. Preoperative preparation, as well as the surgery itself, can induce a metabolic stress response and an inflammatory ripple known to be responsible for the catabolic response, muscle wasting, hyperglycemia, insulin resistance, which leads to delayed wound healing, prolonged ileus, and other adverse outcomes.6
Preoperative oral carbohydrate-rich solutions given at least 2 hours prior to major abdominal surgery may decrease insulin resistance and its negative effects. Based on previous studies, patients should be fed with a controlled volume at specified times.6 This can cause patient discomfort and anxiety. With this background, our purpose is to evaluate the difference of insulin resistance in those who received ORS 1 day until 2 hours prior to surgery and those who did not. We want to show the benefit of freely drinking a carbohydrate-rich ORS, not limited by a specified volume or time, except until 2 hours before surgery.
MATERIALS AND METHODS
The objective of this study is to determine if ORS administration for patients undergoing elective colon surgery will decrease insulin resistance.
The primary endpoint is to compare changes in homeostatic model assessment-insulin resistance (HOMA-IR) levels between the treatment and the control group.
The secondary endpoints are to compare changes in insulin levels, glucose levels, cortisol and triglyceride levels. The pain scale will be evaluated using the visual analogue scale (VAS), including stress relief from shorter NPO period. The postoperative surgical complications will be evaluated and compared as well (Fig. 1).
Fig. 1
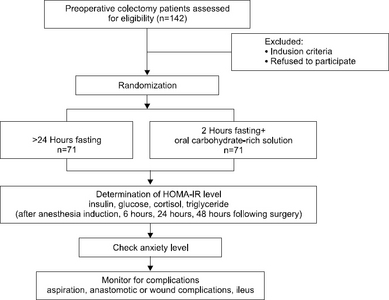
Consort diagram. This figure describes the methodology of the study. The sample size computed for this study is a minimum of 142 subjects, with 71 subjects per control and treatment arms. Outcome measures are HOMA-IR, insulin, glucose, cortisol, and triglyceride level, anxiety level, and presence of complication. HOMAIR = homeostatic model assessmentinsulin resistance.
This study has been reviewed and accepted by the Seoul National University Bundang Hospital Institutional Review Board (B-1310/224-007), Ethics Committee, and Clinicaltrial.gov Committee (NCT02062788).
The methodology of this research, the retrieval of its data and analysis are all in agreement with the fundamental spirit of Korea Good Clinical Practice and the Declaration of Helsinki. The research is conducted as according to the Korean law. The primary investigators are obligated to promptly report any approval or non-approval of the research proposal and/or its progress made by the IRB. The final report is also to be reported to the committee once the research is complete.
This is a randomized controlled trial conducted for 2 years from March 2014 to February 2016.
Based on a study by Viganò et al.6 about the effects of preoperative oral carbohydrate supplementation on postoperative metabolic stress response of patients undergoing abdominal surgery, we calculated our sample size, with a significance level of 5%, test power of 80%, and considered a dropout rate of 10%. The computed sample size is 71 subjects per arm, for a total of 142 patients.
1) Inclusion criteria
All subjects for elective colon surgery are randomized with the following inclusion criteria: adults 19-75 years of age, American Society of Anesthesiologists grade I∼II, those who can take ORS with intact swallowing mechanism, body mass index of less than 27.5, Child-Turcotte-Pugh Classification score of less than 6, patients fluent in speaking and writing Korean.
2) Exclusion criteria
The exclusion criteria are as follows: emergency colon surgery (i.e., those with perforation or obstruction), abdominal distention, patients with comorbidities (i.e., diabetes mellitus, cerebrovascular accident, chronic obstructive pulmonary disease, end-stage renal disease, myocardial infarction, transient ischemic attack), those with aspiration tendencies, with food allergies, prior gastric surgery due to limitations of evaluation of gastric residue, and those with clinical T4 or M1 disease.
3) Treatment
All subjects who will undergo elective colectomy, from March 2014 to February 2016, that fulfill the inclusion and exclusion criteria, is randomized by the Medical Research Collaborating Center. This is an independent research center that determines that both arms in the study are evenly distributed.
Elective colectomy patients are typically administered with osmotic laxatives (Colyte) 2 days prior to the surgery and are kept under NPO one day prior to the day of surgery. Nutritional support during the fasting period is administered intravenously using dextrose solution. This will be the treatment for the control group.
The treatment group, on the other hand, is allowed to take ORS as tolerated one day prior to the surgery until two hours prior to surgery. The rest of the treatments are the same.
All patients will be asked to fill out a questionnaire prior to surgery. Serum glucose and insulin levels are obtained for four sequential times - right after induction, 6 hours, 24 hours, and 48 hours post-op, respectively. The samples will be collected opposite the IV site on the antecubital fossa. The HOMA-IR level is derived using the equation HOMA- IR Index equation (evaluation of Insulin resistance5-7)
=Insulin (μU/mL)×blood glucose (mg/dL)/405
Serum triglyceride and cortisol levels will be obtained on two different occasions for comparison.
The gastric residual volume will be assessed after induction of anesthesia. A suction catheter is positioned in the stomach and aspirate samples are obtained using a syringe. The amount and pH levels (using pH meter) will be measured and recorded.
The patients start sips of water followed by a full liquid diet on the 2nd postoperative day. After which, a soft blended diet is allowed on the 3rd postoperative day, and a full regular diet on the same day or the day after.
4) Study endpoints
To assess the primary endpoint, HOMA-IR, the mean and standard deviation of the two groups are compared from the continuous variable glucose and insulin values. We plot the data obtained from the two groups following a Gaussian distribution, comparing its values.
The secondary endpoints, including insulin, glucose, cortisol, and triglyceride levels will be recorded and compared. The VAS and anxiety will be evaluated, including postoperative complications such as pertaining to the surgical site (i.e., anastomotic leak, anastomotic bleeding, anastomotic breakdown, abscess formation, obstruction), wound (i.e., seroma, hematoma, infection, wound dehiscence), or return to bowel function (i.e., paralytic ileus).
The difference between the two groups will be compared using an independent t-test statistical analysis.
RESULTS
Given the studies and data about preoperative carbohydrate-rich drink administration for patients undergoing elective surgery, we expect that there is less insulin resistance in these patients compared to the group who had undergone a longer fasting period.
Insulin, glucose, cortisol, and triglyceride levels are lower in the treatment arm.
Preoperative oral carbohydrate-rich solution given freely 1 day until 2 hours prior to surgery decreases anxiety, discomfort, and alleviates thirst and hunger.
For complications, there is no difference in the incidence of aspiration and other postoperative complications, including anastomotic leak or breakdown, abscess formation, obstruction on both arms. Wound complications, such as surgical site infection, are lesser in the treatment arm, as well as incidence of paralytic ileus.
DISCUSSION
ERAS was introduced in the early 2000s by Kehlet and Wilmore,11 and was applied primarily to patients receiving colectomy. As the knowledge and understanding of this concept continues to grow, we are now able to change the way we treat pre- and postoperative patients. This includes patient preparation and intervention like preoperative optimization, preoperative bowel preparation, fasting, anesthetic medications, thromboembolic prophylaxis, antibiotic use, pain control, mobilization, nutritional support and so on. In Europe, it has been proven that applying this concept to patients resulted in decreased length of post-operative hospital stay, post-op complications and overall hospital costs.8,9,12
Shortened preoperative fasting and carbohydrate-containing fluids preoperatively given 2 hours prior to surgery has been shown to be safe and beneficial to patients undergoing surgery.1-5 It has been shown to reduce patient thirst, stress and anxiety, postoperative protein and muscle loss, and insulin resistance.1-3
Insulin resistance increases in procedures such as herniorrhaphy or laparoscopic cholecystectomy.13 Administration of preoperative carbohydrates decrease post-op nausea and vomiting,1-4,14 permits early postoperative feeding, accelerates recovery, thereby shortening hospital stay and costs.
Conventional pre-op 8 hour fasting increases insulin resistance and influences increased glucose levels.1-4,15-18 Insulin resistance has various impacts on the outcome and recovery of patients especially those undergoing major surgery. Therefore, primary care physicians, surgeons, anesthesiologists, and nutritionists aim to decrease risk factors for its development to enhance recovery and decrease complications that coincide with insulin resistance.
Intake of a carbohydrate-rich solution induces insulin release which is normally seen after intake of a meal. This prevents the various physiological mechanisms that occur with prolonged fasting, such as activation of gluconeogenesis, glycogenolysis, and oxidation of fatty acids.19 Liver glycogen stores are increased as much as 44% compared to those who have prolonged fasting times.20,21
Additional benefits of shorter preoperative fasting include decrease in patient discomfort from fasting state; helps stabilize postoperative glucose, triglyceride, and cortisol levels. Due to stimulation of the gut-associated lymphatic tissue through shorter preoperative fasting, this preserves intestinal barrier function, reduces bacterial translocation, which contributes to lesser postoperative infection rates.1-4,6,22-27
In monitoring intraoperative and postoperative complications, there is no difference in the incidence of aspiration. Studies have shown that gastric emptying time for clear liquids, such as carbohydrate-rich solutions, is 120 minutes. Therefore, the 2-hour fasting time preoperatively is adequate and safe for patients.28
Other postoperative complications, including anastomotic leak or breakdown, abscess formation, obstruction, will have no difference between the two groups.29 Wound healing and recovery is faster in the ORS group. This can be explained due to better glucose control and decreased insulin resistance. Insulin resistance impairs delays wound contraction, epithelialization and formation of granulation tissue essential for proper and lasting wound healing.30 Delayed wound healing and repair may also predispose patients to wound morbidity such as surgical site infections.
Overall, surgical patients will benefit with preoperative carbohydrate-rich solution as tolerated and shorter preoperative fasting periods. Giving carbohydrate-rich oral solution 2 hours preoperatively will decrease insulin resistance, have better glucose control, lower levels of insulin, cortisol, and triglycerides. Patient will experience greater comfort, lesser anxiety, hunger, and thirst; without increasing postoperative complications. It is safe as it is beneficial.
- 1. Ljungqvist O, Jonathan E. Rhoads lecture 2011: Insulin resistance and enhanced recovery after surgery. JPEN J Parenter Enteral Nutr 2012;36(4):389-98. PubMed
- 2. Ljungqvist O, Nygren J, Thorell A. Modulation of post-operative insulin resistance by pre-operative carbohydrate loading. Proc Nutr Soc 2002;61(3):329-36. ArticlePubMed
- 3. Kratzing C. Pre-operative nutrition and carbohydrate loading. Proc Nutr Soc 2011;70(3):311-5. ArticlePubMed
- 4. Yang DJ, Zhang S, He WL, Chen HY, Cai SR, Chen CQ, et al. Fast track surgery accelerates the recovery of postoperative insulin sensitivity. Chin Med J (Engl) 2012;125(18):3261-5.PubMed
- 5. Faria MS, de Aguilar-Nascimento JE, Pimenta OS, Alvarenga LC Jr, Dock-Nascimento DB, Slhessarenko N. Preoperative fasting of 2 hours minimizes insulin resistance and organic response to trauma after video-cholecystectomy: a randomized, controlled, clinical trial. World J Surg 2009;33(6):1158-64. ArticlePubMedPDF
- 6. Viganò J, Cereda E, Caccialanza R, Carini R, Cameletti B, Spampinato M, et al. Effects of preoperative oral carbohydrate supplementation on postoperative metabolic stress response of patients undergoing elective abdominal surgery. World J Surg 2012;36(8):1738-43. ArticlePubMedPDF
- 7. Soop M, Nygren J, Myrenfors P, Thorell A, Ljungqvist O. Preoperative oral carbohydrate treatment attenuates immediate postoperative insulin resistance. Am J Physiol Endocrinol Metab 2001;280(4):E576-83. ArticlePubMed
- 8. Søreide E, Eriksson LI, Hirlekar G, Eriksson H, Henneberg SW, Sandin R, et al. (Task Force on Scandinavian Pre-operative Fasting Guidelines, Clinical Practice Committee Scandinavian Society of Anaesthesiology and Intensive Care Medicine). Pre- operative fasting guidelines: an update. Acta Anaesthesiol Scand 2005;49(8):1041-7. ArticlePubMed
- 9. Hausel J, Nygren J, Lagerkranser M, Hellström PM, Hammarqvist F, Almström C, et al. A carbohydrate-rich drink reduces preoperative discomfort in elective surgery patients. Anesth Analg 2001;93(5):1344-50. ArticlePubMed
- 10. Braga M, Ljungqvist O, Soeters P, Fearon K, Weimann A, Bozzetti F. ESPEN. ESPEN Guidelines on Parenteral Nutrition: surgery. Clin Nutr 2009;28(4):378-86. PubMed
- 11. Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002;183(6):630-41. ArticlePubMed
- 12. Brady M, Kinn S, Stuart P. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst Rev 2003;4:CD004423. Article
- 13. Nygren J. The metabolic effects of fasting and surgery. Best Pract Res Clin Anaesthesiol 2006;20(3):429-38. ArticlePubMed
- 14. Hausel J, Nygren J, Thorell A, Lagerkranser M, Ljungqvist O. Randomized clinical trial of the effects of oral preoperative carbohydrates on postoperative nausea and vomiting after laparoscopic cholecystectomy. Br J Surg 2005;92(4):415-21. ArticlePubMedPDF
- 15. Ljungqvist O, Nygren J, Soop M, Thorell A. Metabolic perioperative management: novel concepts. Curr Opin Crit Care 2005;11(4):295-9. ArticlePubMed
- 16. van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in critically ill patients. N Engl J Med 2001;345(19):1359-67. ArticlePubMed
- 17. Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc 2004;79(8):992-1000. ArticlePubMed
- 18. Svanfeldt M, Thorell A, Hausel J, Soop M, Nygren J, Ljungqvist O. Effect of “preoperative” oral carbohydrate treatment on insulin action--a randomised cross-over unblinded study in healthy subjects. Clin Nutr 2005;24(5):815-21. ArticlePubMed
- 19. Pimenta GP, de Aguilar-Nascimento JE. Prolonged preoperative fasting in elective surgical patients: why should we reduce it? Nutr Clin Pract 2014;29(1):22-8. PubMed
- 20. Gjessing PF, Constantin-Teodosiu D, Hagve M, Lobo DN, Revhaug A, Irtun Ø. Preoperative carbohydrate supplementation attenuates post-surgery insulin resistance via reduced inflammatory inhibition of the insulin-mediated restraint on muscle pyruvate dehydrogenase kinase 4 expression. Clin Nutr 2014;doi:10.1016/j.clnu.2014.12.004. [Epub ahead of print]. Article
- 21. Awad S, Constantin-Teodosiu D, Constantin D, Rowlands BJ, Fearon KC, Macdonald IA, et al. Cellular mechanisms underlying the protective effects of preoperative feeding: a randomized study investigating muscle and liver glycogen content, mitochondrial function, gene and protein expression. Ann Surg 2010;252(2):247-53. PubMed
- 22. Engelhardt T, Wilson G, Horne L, Weiss M, Schmitz A. Are you hungry? Are you thirsty?--fasting times in elective outpatient pediatric patients. Paediatr Anaesth 2011;21(9):964-8. ArticlePubMed
- 23. Hendry PO, Balfour A, Potter MA, Mander BJ, Bartolo DC, Anderson DN, et al. Preoperative conditioning with oral carbohydrate loading and oral nutritional supplements can be combined with mechanical bowel preparation prior to elective colorectal resection. Colorectal Dis 2008;10(9):907-10. ArticlePubMed
- 24. Brady M, Kinn S, Ness V, O’ Rourke K, Randhawa N, Stuart P. Preoperative fasting for preventing perioperative complications in children. Cochrane Database Syst Rev 2009;4:CD005285. Article
- 25. Kasama K, Mui W, Lee WJ, Lakdawala M, Naitoh T, Seki Y, et al. IFSO-APC consensus statements 2011. Obes Surg 2012;22(5):677-84. ArticlePubMedPDF
- 26. Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, et al. Enhanced Recovery After Surgery Society. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Clin Nutr 2012;31(6):783-800. PubMed
- 27. Luttikhold J, Oosting A, van den Braak CC, van Norren K, Rijna H, van Leeuwen PA, et al. Preservation of the gut by preoperative carbohydrate loading improves postoperative food intake. Clin Nutr 2013;32(4):556-61. ArticlePubMed
- 28. Lobo DN, Hendry PO, Rodrigues G, Marciani L, Totman JJ, Wright JW, et al. Gastric emptying of three liquid oral preoperative metabolic preconditioning regimens measured by magnetic resonance imaging in healthy adult volunteers: a randomised double-blind, crossover study. Clin Nutr 2009;28(6):636-41. ArticlePubMed
- 29. Zhuang CL, Ye XZ, Zhang CJ, Dong QT, Chen BC, Yu Z. Early versus traditional postoperative oral feeding in patients undergoing elective colorectal surgery: a meta-analysis of randomized clinical trials. Dig Surg 2013;30(3):225-32. ArticlePubMedPDF
- 30. Al-Niaimi AN, Ahmed M, Burish N, Chackmakchy SA, Seo S, Rose S, et al. Intensive postoperative glucose control reduces the surgical site infection rates in gynecologic oncology patients. Gynecol Oncol 2015;136(1):71-6. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Preoperative carbohydrate loading reduces length of stay after major elective, non-cardiac surgery when compared to fasting: a systematic review and meta-analysis
Anna Réka Sebestyén, Caner Turan, Ambrus Szemere, Marcell Virág, Klementina Ocskay, Fanni Dembrovszky, László Szabó, Péter Hegyi, Marie Anne Engh, Zsolt Molnár
Scientific Reports.2025;[Epub] CrossRef - Oral high-carbohydrate solution as an alternative dietary modality in patients with acute pancreatitis
See Young Lee, Jaein Lee, Jae Hee Cho, Dong Ki Lee, Yeseul Seong, Sung Ill Jang
Pancreatology.2024; 24(7): 1003. CrossRef - Effect of preoperative oral carbohydrate loading on postoperative insulin resistance, patient-perceived well-being, and surgical outcomes in elective colorectal surgery: a randomized controlled trial
Shanmugam Mannoj Kumar, Amaranathan Anandhi, Sathasivam Sureshkumar, Andi Rajendharan Keerthi, Kalayarasan Raja, Ajay Kumar Jha, Zachariah Bobby, Vikram Kate
Journal of Gastrointestinal Surgery.2024; 28(10): 1654. CrossRef - Effects of Preoperative Oral Carbohydrate Loading on Neutrophil/Lymphocyte Ratio and Postoperative Complications following Colorectal Cancer Surgery: A Randomized Controlled Study
Nermina Rizvanović, Višnja Nesek Adam, Merlina Kalajdžija, Senada Čaušević, Senad Dervišević, Jasmina Smajić
European Surgical Research.2023; 64(2): 278. CrossRef - Effects of preoperative oral carbohydrate on postoperative discomfort in patients undergoing elective surgery: a meta-analysis of randomized controlled trials
Po-Lung Cheng, El-Wui Loh, Jui-Tai Chen, Ka-Wai Tam
Langenbeck's Archives of Surgery.2021; 406(4): 993. CrossRef - A randomised controlled study of preoperative oral carbohydrate loading versus fasting in patients undergoing colorectal surgery
Nermina Rizvanović, Višnja Nesek Adam, Senada Čaušević, Senad Dervišević, Samir Delibegović
International Journal of Colorectal Disease.2019; 34(9): 1551. CrossRef
 Cite
CiteThe Evaluation of Preoperative Oral Carbohydrate-Rich Solution Effects on Insulin Resistance in Patients undergoing Colectomy
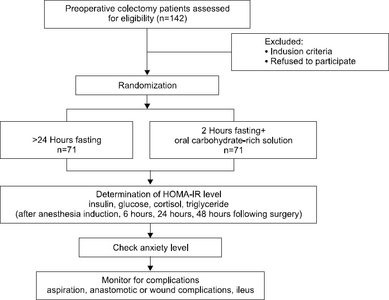
Fig. 1
Consort diagram. This figure describes the methodology of the study. The sample size computed for this study is a minimum of 142 subjects, with 71 subjects per control and treatment arms. Outcome measures are HOMA-IR, insulin, glucose, cortisol, and triglyceride level, anxiety level, and presence of complication. HOMAIR = homeostatic model assessmentinsulin resistance.
Fig. 1
The Evaluation of Preoperative Oral Carbohydrate-Rich Solution Effects on Insulin Resistance in Patients undergoing Colectomy

