 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Surgical Metabolism and Nutrition > Volume 8(2); 2017 > Article
- Review Article Enteral Nutrition in Liver Disease
- Kyung Sik Kim, M.D., Ph.D.
- 간질환 환자에서의 경장영양요법
- 김경 식, M.D., Ph.D.
-
Surgical Metabolism and Nutrition 2017;8(2):28-35.
DOI: https://doi.org/10.18858/smn.2017.8.2.28
Published online: December 30, 2017
Department of Surgery, Yonsei University College of Medicine, Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Severance Hospital, Seoul, Korea
- Correspondence to: Kyung Sik Kim, Department of Surgery, Yonsei University College of Medicine, Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Severance Hospital, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea E-mail: kskim88@yuhs.ac
• Received: December 28, 2017 • Accepted: December 30, 2017
Copyright: © The Korean Society of Surgical Metabolism and Nutrition
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,910 Views
- 13 Download
Abstract
- Patients with chronic liver disease have a high risk to malnutrition. Proper nutrition should be provided through a proper nutritional assessment. Enteral nutrition is recommended as a nutritional supplement because it maintains the intestinal mucosa, reduces infectious complications, is less costly than parenteral nutrition, and is more physiological to use intestine. The purpose of this review is to define the nutritional deficiencies of patients with liver disease and to show the indications for enteral nutrition and to validate the efficacy of enteral nutrition. According to the various guidelines and researches, enteral nutrition is used as a solution to the nutritional problems caused by patients with liver disease. The optimal enteral formula will be selected on the nutritional problems. It is expected that the enteral nutrition will reduce especially postoperative complications, intraperitoneal complications, pneumonia, and wound infection. The enteral nutrition for patients with chronic liver disease should be actively implemented.
서론
최근 들어 다양한 약제의 등장으로 비교적 양호한 경과를 보이기는 하지만 아직도 많은 간질환 환자들이 만성 질환의 양상으로 만성 간염에서 30∼50년 경과 후 간경변으로 이행되어 간경변증에 의한 합병증으로 인해 사망하는 것으로 알려져 있다. 정상 사람보다 간경변 환자에서 기초 대사량과 휴식 에너지 소비량의 비율이 높아 에너지 소비가 많은 것으로 보고되고 있어 영양 불량이 발생할 위험이 매우 높다(Fig. 1).
Fig. 1
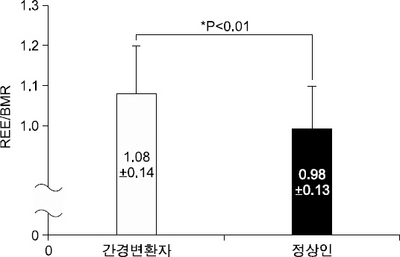
Resting energy consumption and basal energy requirement in normal and patients with liver cirrhosis.
특히 심한 간경변 환자에서는 단백질 부족과 에너지 영양 불량이 같이 있는 경우가 많아 골격근과 면역 기능이 손상될 수 있어 이에 대한 영양 공급은 필수적이다.[1]
경장 영양 요법은 장점막을 유지하여 감염성 합병증을 줄이며 정맥 영양 요법에 비해 적은 비용으로 가능하며 보다 생리적이라는 점에서 영양 공급에 있어서 우선 시행하는 것이 권장되고 있다.[2] 경장 영양 요법은 아주 오래 전부터 시행되어 온 방법으로 이집트 시대에서도 시행되었다는 보고도 있지만 1910년 날문통과 튜브(postpyloric tube) 삽입이 시도되면서 도입되기 시작되었고 1970년대부터 많은 경구용 제재가 개발되면서 활기를 띠게 되었다.[3] 최근에 발간된 중환자 관리 의학회(society of critical care medicine)과 미국 경장 영양학회(American society of parenteral and enteral nutrition)에서 제정한 영양 지원 제공과 평가에 관한 가이드라인에서 간부전을 보이는 중환자에 대해서 다음의 3가지의 주요 질문을 하고 있다.[4] 첫째, 간부전을 보이는 중환자에서 에너지 및 단백질의 공급을 간부전이 없는 경우에 동일하게 결정해야만 하나? 둘째, 간부전을 보이는 환자에서 적합한 영양 공급 경로는 무엇인가? 셋째, 간질환을 가진 중환자에서 질병 특이 경장제재가 필요한가? 전문가들의 의견 합의에 근거할 때 급성/만성 간질환을 가진 중환자에서도 경장 영양 공급이 영양 공급의 방법으로 더 선호된다.[5] 이들 환자에게 제공되는 경장제재로는 표준 경장 제재를 권장하고 있으며 간성 혼수에 빠진 경우에 장관에 작용하는 항생제와 락트로우즈(lactulose)를 투여하고 있다면 분지형 아미노산 제재(branched chain amino acid)의 공급은 더 이득이 있다는 증거는 없다고 하였다.[6]
그러므로 본 종설에서는 간질환 환자에서의 영양 부전 요인을 살펴보고 영양 지원에 관한 진료 가이드라인에서 제시한 경장영양 요법에 대한 적응증과 여러 가지 경장 제재의 효능성에 대해 알아보고자 한다.
본론
만성 간질환 환자에서의 영양 부전이 일어나는 원인을 살펴보면 크게 1) 부적절한 영양 섭취, 2) 대사의 변화, 3) 흡수 장애이다(Table 1).[7] 부적절한 영양 섭취는 종양 괴사인자 알파(Tumor necrosis factor α)와 렙틴(leptin)의 증가에 의한 식욕(appetite)의 감소에 의해 생기게 된다. 또한 간경변으로 생긴 복수는 위의 팽창을 막아 조금만 먹어도 배가 부르게 되고 위배출이 저하되며 속이 더부룩한(bloating) 느낌과 복부 팽창을 야기하게 된다. 그 밖의 원인으로는 간성 혼수로 인한 구강 섭취의 저해, 알코올성 간질환에서는 알코올의 섭취, 메스꺼움과 구토, 저염식 식이 및 저단백식이, 수분제한, 아연 부족에 의한 입맛의 변화, 사회 경제적인 제약(socioeconomic constraints) 등이 있다.
Table 1
Factors contributing to malnutrition in patients with chronic liver disease
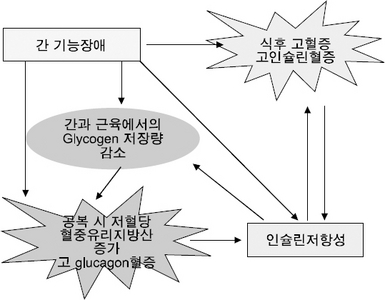
간질환 환자에서의 대사의 변화를 살펴보면 탄수화물, 지방 및 단백질 대사가 변하고 에너지 소비의 형태가 달라진다. 글리코겐의 저장 정도가 낮아지고 영양분의 저장 능력이 감소하며 인슐린 저항성이 생기게 된다는 것이다(Fig. 2).
담즙 정체성 간질환의 경우에는 담즙의 부족이 나타날 수 있고 박테리아의 과잉 증식과 문맥압의 증가로 인해 위장관장애가 일어나서 흡수장애가 생길 수 있다.
앞에서 언급한 것처럼 만성 간질환환자에서 영양 불량은 쉽게 일어날 수 있으므로 적절한 영양 공급을 시행하기 위해서 영양 평가는 반드시 필요하다. 영양 평가는 기존의 방법으로 시행할 수 있으나 프리알부민과 알부민과 같은 생화학적 지표를 사용할 경우에는 이들 지표가 간에서 형성되기 때문에 간질환의 정도에 따라 합성 능력과 염증에 의한 반응으로 정확한 검사가 어려울 수 있다. 각각의 영양 평가 방법에 따른 장점과 단점을 정리하면 아래와 같다(Table 2, 3).[8]
Table 2
Tools for assessing oral protein-energy intake in end stage liver disease
Table 3
Anthropometric assessment in end stage liver disease
1) 유럽 경정맥 경장 영양학회 가이드라인(2006) [9]
적절한 개인맞춤 영양 조언에도 불구하고 경구섭취를 통해 칼로리 필요량을 충족하지 못할 경우에는 경장영양 공급으로 보충해야 하며 정맥류가 있더라도 경구 혹은 경관 급식을 시행한다. 경피적 내시경 위창냄술(percutaneous endoscopic gastrostomy)은 합병증의 위험이 높기 때문에 권장되지는 않는다.
전체 단백제재를 일반적으로 권장하며 간성 혼수가 있는 환자에서는 분지형 아미노산 제재가 많이 들어 있는 제재를 사용한다. 간경변이 심한 경우에는 경구용 분지형 아미노산 제재의 사용이 임상 결과를 증진할 수 있다.
2) 미국 경정맥 경장 영양학회 및 중환자 관리 의학 학회 가이드라인(2009) [10]
급성 만성 간질환을 가진 중환자에서 경장 영양 요법은 영양 치료에 있어서 선호되는 방법으로 간부전을 가진 환자에서도 단백질을 제한해서는 안되며 표준 경장 제재를 사용해야 한다. 장관에 작용하는 항생제와 락투로우즈의 표준 치료에 반응이 없는 드문 간성혼수 환자를 위해 분지형 아미노산 제재는 남겨두어야 한다.
3) 미국 간학회와 위장관 미국 대학 협회 가이드라인(2010) [11]
알코올성 간질환에 대한 미국 간학회와 위장관 미국 대학 협회 가이드라인에서는 중증도의 알코올성 간질환 즉 Maddrey 점수 32점 미만이거나, 간성 혼수가 없고 입원 첫 주 동안 Maddrey 판별 기능(discriminant function)에서 혈청 빌리루빈 수치가 호전되거나 감소되는 환자에서 영양공급과 절주 이외에 다른 내과적 치료는 도움이 되지 않고 세심한 경과 관찰을 해야 한다고 하고 있다. 특히 알코올성 간경변을 가진 환자에서는 질소 균형(nitrogen balance)을 호전 시키기 위해 저녁 스낵, 아침 급식 등의 기간급식(interval feeding)을 해야 한다.
4) 그 밖의 영양 지원 가이드라인
알코올성 간질환에 관한 NICE (2010) 가이드라인[12]과 C형 간염에 관한 SIGN (2013) 가이드라인[13]에서 모두 영양 부전을 막기 위해서 적극적인 영양 요법을 권장하고 있고 필요하다면 비위관 삽입을 통한 급식도 고려할 수 있다고 언급하고 있다.
각각의 가이드라인에서 권장하는 단백질 에너지 요구량을 살펴보면 급성 간성 혼수의 경우에는 단백질을 0.6∼0.8 g/kg/d로 제한하지만 대부분의 경우 정상인 보다 많은 양을 공급해야 하며 에너지 소모량이 많으므로 에너지 공급도 정상보다 많아야 한다고 하고 있다(Table 4). 영양 불량을 가진 간경변 환자에서는 식욕이 저하되어 있어 경장 공급이 경구 영양 공급보다 더 효과적이다. 식도정맥류의 가능성 때문에 경관급식에 대해 다소 논쟁이 있기는 하지만 위장관 출혈이 많지 않거나 간헐적인 경우에도 절대적인 금기는 아니다. 권장되는 경장영양제재는 1 ml당 1.5 Kcal의 고에너지이며 염분은 하루에 40 mmol의 저염식이로 구성한다.
Table 4
Protein-energy requirements in end stage liver disease
경관 급식에 대해 여러 가지의 시도가 보고 되고 있다.[7] 자발적인 경구 영양에 보충적으로 경장 영양을 시행할 경우 생존과 간기능의 항진 효과가 있으며 자기 의지에 의한 경구 섭취가 감소한 환자에서 유익한 효과를 대부분 볼 수 있었다. 단백질은 하루에 kg 당 1.8 g까지 주어도 정신상태 효과에 해롭지 않게 잘 적응하였다. 단백질 표준제재 및 고함유 분지형 아미노산제재를 사용한 경우에 유익한 결과를 얻었으며 특히 야식의 보충은 주간 영양 공급보다 더 효율적으로 총 채내 단백질을 향상시킨다는 것이다.
간질환을 가지고 있는 환자의 영양학적 문제가 무엇인가에 따라 특징적인 경장영양제재가 선택된다(Table 5).
Table 5
Hepatic disease specific formulas
간질환 특이 경장 제재는 우리나라에서도 정식품에서 경장 제재가 출시된 적이 있으나 2007년 단종되었고, 세계적으로도 특수의료용 식품으로 2∼3개의 제품이 있었지만 현재는 네슬레의 NutriHep만 생산되고 있다. 참고적으로 NutriHep의 함량을 살펴보면 1 ml당 1.5 Kcal로 단백질 11%, 탄수화물 77%, 지방 12%로 구성되어 있다. 단백질은 분지형아미노산이 50%이고 지방은 중쇄지방산(medium chain fatty acid)과 장쇄지방산(long chain fatty acid)으로 되어 있고 중쇄지방산과 장쇄지방산과의 비율이 70:30이다. 간질환 특이 경장 제재가 제한되어 있어 일반적인 표준 경장제재, 영양강화제재, 반성분제재(semi-elemental) 혹은 부분적 가수분해 제재, 성분 제재, 신장용 제재, 면역 항진 제재, 분지형아미노산제재 등이 사용되며 각각의 제재의 적응증은 다음과 같다(Table 6).[7]
Table 6
Enteral nutrition formula options for patients with chronic liver disease
Koretz 등[1]이 2012년 1월까지 검색된 자료를 근거로 하여 보고한 간질환을 가진 환자에서 영양 지원에 관한 Cochrane review를 살펴보면 enteral nutrition이 사망률에는 도움을 준다고 하고 있다(Fig. 3).
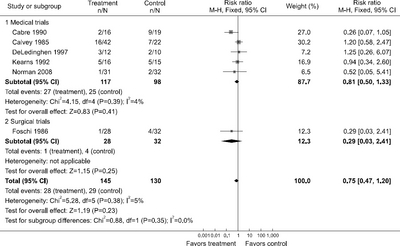
Table 7
Results of meta-analyses of trials comparing enteral nutrition to no nutritional interventions in patients with various liver diseases
Table 8
Results of meta-analyses of trials comparing supplements to no nutritional interventions in patients with various liver diseases
결론
만성 간질환을 가진 환자에서는 영양불량이 생길 가능성이 높아 합리적인 영양평가를 통하여 적절한 영양 공급은 반드시 필요하다. 경장영양요법은 장점막을 유지하여 감염성 합병증을 줄이며 정맥 영양 요법에 비해 적은 비용으로 가능하고, 보다 생리적이라는 점에서 영양 공급 방법으로 권장되고 있다. 경장 제재는 간질환을 가진 환자에서 생긴 영양학적 문제를 해결하기 위한 방안으로 선택되어야 하며 경장 영양요법을 통해 특히 수술 후 합병증과 복강내 합병증, 폐염, 상처 감염 등을 줄일 수 있을 것으로 기대되어 보다 적극적으로 시행되어야 할 것이다.
- 1. Koretz RL, Avenell A, Lipman TO. Nutritional support for liver disease. Cochrane Database Syst Rev 2012;5:CD008344.Article
- 2. Kim ER. Enteral nutritional support in gastrointestinal and liver diseases. Korean J Gastroenterol 2015;65:354-60. ArticlePubMed
- 3. Harkness L. The history of enteral nutrition therapy: from raw eggs and nasal tubes to purified amino acids and early postoperative jejunal delivery. J Am Diet Assoc 2002;102:399-404. PubMed
- 4. McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2016;40:159-211. PubMed
- 5. Xu ZW, Li YS. Pathogenesis and treatment of parenteral nutrition-associated liver disease. Hepatobiliary Pancreat Dis Int 2012;11:586-93. ArticlePubMed
- 6. Holecek M. Branched-chain amino acids and ammonia metabolism in liver disease: therapeutic implications. Nutrition 2013;29:1186-91. ArticlePubMed
- 7. Hasse JM, DiCecco SR. Enteral nutrition in chronic liver disease: translating evidence into practice. Nutr Clin Pract 2015;30:474-87. PubMed
- 8. Johnson TM, Overgard EB, Cohen AE, DiBaise JK. Nutrition assessment and management in advanced liver disease. Nutr Clin Pract 2013;28:15-29. ArticlePubMedPDF
- 9. Plauth M, Cabré E, Riggio O, Assis-Camilo M, Pirlich M, Kondrup J; DGEM (German Society for Nutritional Medicine), Ferenci P, Holm E, Vom Dahl S, Müller MJ, Nolte W; ESPEN (European Society for Parenteral and Enteral Nutrition). ESPEN guidelines on enteral nutrition: liver disease. Clin Nutr 2006;25:285-94. ArticlePubMed
- 10. McClave SA, Martindale RG, Vanek VW, McCarthy M, Roberts P, Taylor B, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2009;33:277-316. PubMed
- 11. O'Shea RS, Dasarathy S, McCullough AJ. Practice Guideline Committee of the American Association for the Study of Liver Diseases;Practice Parameters Committee of the American College of Gastroenterology. Alcoholic liver disease. Hepatology 2010;51:307-28. PubMed
- 12. Swain S, Krause T, Laramee P, Stewart S; Guideline Development Group. Diagnosis and clinical management of alcohol related physical complications: summary of NICE guidance. BMJ 2010;340:c2942.ArticlePubMed
- 13. SIGN. Mangement of hepatitis C. Edinburgh: Scottish Intercollegiate Guidelines Network; 2013. p. 133.
- 14. Koretz RL. The evidence for the use of nutritional support in liver disease. Curr Opin Gastroenterol 2014;30:208-14. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteEnteral Nutrition in Liver Disease
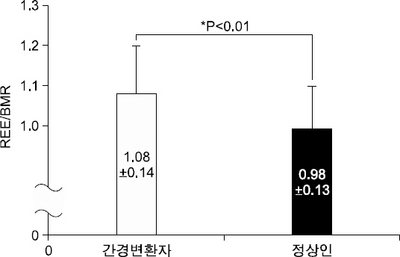
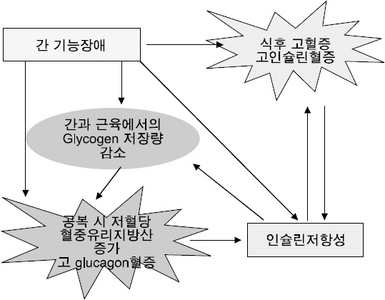
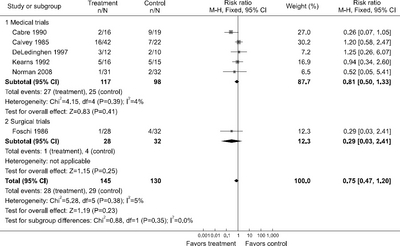
Fig. 1
Resting energy consumption and basal energy requirement in normal and patients with liver cirrhosis.
Fig. 2
Interaction between hepatic function insufficiency and insulin resistance.
Fig. 3
Mortality comparing enteral nutrition to control.
Fig. 1
Fig. 2
Fig. 3
Enteral Nutrition in Liver Disease
Factors contributing to malnutrition in patients with chronic liver disease
| Factor | Mechanisms |
|---|---|
| Inadequate nutrient intake | ↑Levels of tumor necrosis factor-α and leptin → loss of appetite Ascites → impaired gastric expansion → early satiety, delayed gastric emptying, bloating, abdominal distention Hepatic encephalopathy → altered consciousness with decreased oral intake Alcohol intake replaces nutrition Nausea and vomiting Restrictive diets (low-sodium, low-protein, fluid restriction) Altered taste perception (zinc deficiency) Socioeconomic constraints |
| Metabolic alterations | Altered glucose, lipid, and protein metabolism Altered pattern of energy consumption Decreased glycogen levels and reduced ability to store nutrients Insulin resistance |
| Malabsorption | Bile salt deficiency in cholestatic liver disease and cholestasis Small bowel bacterial overgrowth Portal hypertensive enteropathy |
Tools for assessing oral protein-energy intake in end stage liver disease
| Assessment Tool | Method | Strengths | Limitations |
|---|---|---|---|
| 24-Hour recall | • Participant recalls all foods and beverages consumed over the previous 24 hours • Used to estimate protein-calorie intake |
• Low cost • Quick • No equipment required |
• May be inaccurate in those with poor memory or encephalopathy • Underreporting of portions and food items consumed may occur in women, those with body issues, or those who are overweight |
| Food frequency questionnaire | • Participant is given a list of foods/beverages and indicates how frequently these foods are consumed | • Low cost • Quick |
• May not represent foods typically consumed • High level of participant literacy required • Does not provide data on portion sizes or actual protein-energy intake |
| Calorie count | • A healthcare professional calculates protein-energy intake based on foods consumed | • Does not rely on patient’s recall • Low cost • No equipment required |
• Subjective • Portion sizes may not be standard or well documented • Often relies on nursing staff to complete |
| Food diary | • Patient or caregiver records foods eaten • Protein-energy intake is then calculated by a healthcare professional |
• Low cost • Does not require special equipment • Can be very accurate |
• Requires instruction by provider • Requires a higher level of literacy • Subjectivity may lead to inaccuracies • Typically underestimates energy intake • Time-consuming for provider to analyze intake |
Anthropometric assessment in end stage liver disease
| Tool | Method | Strengths | Limitations |
|---|---|---|---|
| Body mass index (BMI) | • Weight (kg)/height (m2) | • Easy to perform • No equipment required • Cost free |
• Inaccurate in patients with ascites or edema unless dry weight is available |
| Waist circumference | • Measures abdominal visceral adiposity | • Easily accessible • Low cost • Component involved in diagnosing metabolic syndrome |
• Not accurate in patients with ascites |
| Mid-arm circumference (MAC) | • Mid-arm is measured to assess muscle mass | • Low cost • Quick • Requires minimal equipment • Useful for assessing changes in muscle mass over time |
• Not a strong predictor of malnutrition |
| Skin fold | • Skin folds are measured using a caliper at various points of the body • Used to assess body fat |
• Low cost • Requires minimal equipment • Number of sites tested improves accuracy |
• Requires training for proper use • Conflicting reports of accuracy in predicting malnutrition in cirrhosis |
| Hand grip strength (HGS) | • A hand dynamometer is used to assess grip strength • Decreased grip strength is associated with malnutrition |
• Low cost • Requires a hand-grip dynamometer • Found to better predict complications of cirrhosis over the Subjective Global Assessment, BMI, skin fold, MAC, and BIA |
• Was not found to correlate with Child-Pugh score |
| Body cell mass (BCM) | • Validated marker used to assess body composition in the cirrhotic patient | • Very accurate even in the fluid-overloaded patient | • Expensive • Not readily available for clinical use and is typically used as a validation tool when analyzing other anthropometric assessments |
| Dual-energy X-ray absorptiometry (DEXA) | • Assesses body composition through a low-dose X-ray | • Gold-standard test | • Expensive • Not readily available |
| Bioelectrical impedance analysis (BIA) | • Measures body composition via an electrical current that estimates total body water, fat-free mass, and body fat | • Easily accessible • Correlates well with Child-Pugh score • Accurate in patients without ascites |
• Not accurate in patients with ascites |
| Air plethysmography | • Measures whole body density and subsequent calculation of body composition | • Noninvasive • Quick, convenient • Requires minimum compliance • Reliable • No water submersion |
• Varies among men and women • Limited availability |
Protein-energy requirements in end stage liver disease
| A.S.P.E.N./ESPEN | |
| Energy requirement based on dry weight or determined ideal body weight if ascites is present | 25∼40 kcal/kg/d |
| A.S.P.E.N. | |
| Stable and malnourished | REE×1.2∼1.4 |
| Without encephalopathy | REE×1.2∼1.4 1.0∼1.5 g/kg/d protein |
| Acute encephalopathy | REE×1.2∼1.4 0.6∼0.8 g/kg/d protein |
| ESPEN | |
| All stable cirrhosis patients | 35∼40 kcal/kg/d 1.0∼1.5 g/kg/d protein |
| Critically Ill | |
| ICU malnourished patients at risk for refeeding | 15∼20 kcal/kg/d 1.2 g/kg/d protein |
| ICU for maintenance caloric support | 25∼30 kcal/kg/d 1.5 g/kg/d protein |
| Catabolic | 35∼50 kcal/kg/d |
| Critically ill obese (body mass index <30) | Mifflin–St Jeor equation Indirect calorimetry for comorbidities 1.5∼2.0 g/kg/d protein ideal body weight |
Hepatic disease specific formulas
| Nutritional problems | Formula characteristics |
|---|---|
| Malnutrition | Calorically dense |
| Altered protein/carbohydrate metabolism | High branched-chain: aromatic amino acid ratio |
| Impaired urea synthesis | |
| Fat malabsorption | Fat system with MCT oil |
| Micronutrient deficiencies | Modified micronutrient profile |
| Fluid/sodium retention | Calorically dense, low sodium |
Enteral nutrition formula options for patients with chronic liver disease
| Enteral nutrition formula category | Indications and comments | Relative cost |
|---|---|---|
| Standard intact protein formulas | • Require normal digestion • Available in a variety of protein and calorie concentrations |
$ |
| Nutrient-dense formulas | • Require normal digestion • Generally available as 1.5∼2 kcal/ml concentrations • Useful in patients in whom fluid restriction is needed (eg, hypervolemic hyponatremia, fluid retention, reduced urine output, early satiety, high nutrition requirements) |
$ |
| Semi-elemental or partially hydrolyzed formulas | • Useful for patients who have impaired digestion • Available in a variety of protein and calorie concentrations • Often contain peptides and/or medium-chain triglycerides |
$$ |
| Elemental formulas | • Useful when digestion is impaired or a very-low-fat formula is preferred • Contain amino acids and dextrose (vs whole proteins and starches) • Usually high in carbohydrate, which could contribute to hyperglycemia in patients with insulin impairment • Usually hypertonic, which can reduce tolerance |
$$$ |
| Renal formulas | • Require normal digestion • Useful for patients with renal dysfunction and hyperkalemia or hyperphosphatemia • Usually fluid-restricted with reduced amounts of potassium and phosphorus |
$$ |
| Immune-enhancing formulas | • Require normal digestion • Have not been shown to be beneficial in patients with liver disease • Usually contain immune-enhancing nutrients such as fish oil, arginine, RNA • May affect insulin sensitivity and satiety • May temporarily increase serum ammonia levels but do not worsen symptoms of hepatic encephalopathy |
$$$ |
| BCAA formulas | • Controversial as to benefit, but American and European guidelines suggest consideration of BCAA formulas in patients with encephalopathy refractory to other treatments or with a protein intolerance • Contain higher proportion of BCAAs and reduced amounts of aromatic amino acids and methionine • Usually have reduced electrolyte content |
$$$ |
Results of meta-analyses of trials comparing enteral nutrition to no nutritional interventions in patients with various liver diseases
| Outcome | Cirrhosis | Alcoholic hepatitis | Liver transplantation | Obstructive jaundice |
|---|---|---|---|---|
| Mortality | 0.85 (0.54, 1.33); 4 (219) | 1.10 (0.61, 1.99); 2 (95) | No data | 0.29 (0.03, 2.41); 1 (60) |
| Appearance ascites | No data | No data | No data | No data |
| Resolution ascites | 0.86 (0.46, 1.62); 1 (29) | No data | No data | No data |
| Gastrointestinal bleeding | 1.17 (0.59, 2.34); 4 (215) | 2.88 (0.70, 11.87); 1 (64) | No data | No data |
| Appearance encephalopathy | 3.13 (0.64, 15.34); 2 (121) | 1.03 (0.26, 4.12); 2 (48) | 1.71 (0.46, 6.44); 1 (32) | No data |
| Resolution encephalopathy | No data | 1.57 (0.59, 4.13); 2 (47) | No data | No data |
| Infections | 0.91 (0.65, 1.29); 4 (211) | 0.96 (0.41, 2.25); 1/64 | 0.46 (0.15, 1.40); 1 (31) | 0.51 (0.18, 1.47); 1 (60) |
| Serum bilirubin | 0.37 (0.40, 1.15); 2 (162) | 5.90 (17.54, 5.74); 1 (31) | No data | No data |
| Duration of hospitalization | 1.08 (2.65, 4.80); 2/57 | No data | 9.80 (27.66, 8.06); 1 (31) | No data |
| Total postoperative complications | N/A | N/A | No data | 0.35 (0.16, 0.91); 1 (60) |
| Intra-abdominal postoperative complications | N/A | N/A | No data | 0.46 (0.10, 2.17); 1 (60) |
| Postoperative pneumonia | N/A | N/A | No data | 0.38 (0.02, 8.95); 1 (60) |
| Postoperative wound infections | N/A | N/A | No data | 0.46 (0.10, 2.17); 1 (60) |
Results of meta-analyses of trials comparing supplements to no nutritional interventions in patients with various liver diseases
| Outcomes | Cirrhosis | Hepatocellular carcinoma | Liver transplantation | Surgery | Hepatitis C treatment |
|---|---|---|---|---|---|
| Mortality | 0.53 (0.24, 1.15); 5 (205) | 1.18 (0.95,1.47); 4 (505) | 0.27 (0.06, 1.23); 1 (82) | 1.50 (0.37, 5.98); 3 (136) | 3.11 (0.13, 73.08); 1 (53) |
| Appearance ascites | 0.72 (0.36, 1.46); 2 (62) | 0.53 (0.30, 0.87); 2 (286) | No data | No data | No data |
| Resolution ascites | 4.16 (0.87, 19.84); 2 (29) | No data | No data | No data | No data |
| Gastrointestinal bleeding | 0.87 (0.45, 1.69); 3 (118) | 1.50 (0.53, 4.26); 2 (305) | No data | 1.10 (0.07, 16.43); 1 (44) | No data |
| Appearance encephalopathy | 0.87 (0.67, 1.14); 9 (332) | 0.75 (0.38, 1.48); 2 (305) | 0.43 (0.14, 1.32); 1 (29) | Not estimable (no events in 68 patients in 2 trials) | No data |
| Resolution encephalopathy | 3.75 (1.15, 12.18) 2 (53) | No data | No data | No data | No data |
| Infections | 0.50 (0.24, 1.03); 3 (184) | 0.35 (0.01, 8.34); 1 (84) | No data | 0.86 (0.44, 1.67); 3 (94) | No data |
| Serum bilirubin | 0.24 (−2.00, 2.51); 2 (87) | No data | No data | No data | No data |
| Duration of hospitalization | −8.00 (−17.54, 1.54); 1 (36) | See text | No data | See text | No data |
| Total postoperative complications | N/A | N/A | No data | 0.85 (0.66, 1.10); 4 (162) | N/A |
| Intra-abdominal postoperative complications | N/A | N/A | No data | 0.30 (0.05, 1.74); 2 (68) | N/A |
| Postoperative pneumonia | N/A | N/A | No data | 0.55 (0.26, 2.29); 2 (68) | N/A |
| Postoperative wound infections | N/A | N/A | No data | 0.77 (0.26, 2.29); 2 (68) | N/A |
Table 1 Factors contributing to malnutrition in patients with chronic liver disease
Table 2 Tools for assessing oral protein-energy intake in end stage liver disease
Table 3 Anthropometric assessment in end stage liver disease
Table 4 Protein-energy requirements in end stage liver disease
Table 5 Hepatic disease specific formulas
Table 6 Enteral nutrition formula options for patients with chronic liver disease
Table 7 Results of meta-analyses of trials comparing enteral nutrition to no nutritional interventions in patients with various liver diseases
Table 8 Results of meta-analyses of trials comparing supplements to no nutritional interventions in patients with various liver diseases

