 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Surgical Metabolism and Nutrition > Volume 10(2); 2019 > Article
- ORIGINAL ARTICLE Clinical Implications of the Cut-off Value of the Preoperative Prognostic Nutritional Index in Patients with Early Stage Gastric Cancer
- Ji Hye Jung, M.D.1, Ji Yeong An, M.D., Ph.D.1, You Na Kim, M.D.2, Min Gew Choi, M.D., Ph.D.1, Jun Ho Lee, M.D., Ph.D.1, Tae Sung Sohn, M.D., Ph.D.1, Jae Moon Bae, M.D., Ph.D.1, Sung Kim, M.D., Ph.D.1
-
Surgical Metabolism and Nutrition 2019;10(2):59-65.
DOI: https://doi.org/10.18858/smn.2019.10.2.59
Published online: December 30, 2019
Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine
Department of Surgery, Korea University College of Medicine, Seoul, Korea
Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine
Department of Surgery, Korea University College of Medicine, Seoul, Korea
- Correspondence to: Ji Yeong An, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-0884, Fax: +82-2-3410-6981, E-mail: jar319.an@samsung.com
• Received: September 25, 2019 • Accepted: October 28, 2019
Copyright: © The Korean Society of Surgical Metabolism and Nutrition
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,612 Views
- 4 Download
Abstract
-
Purpose: The perioperative nutritional status is a potential prognostic factor in gastric cancer patients. This study assessed the optimal cut-off value of the prognostic nutritional index (PNI) for predicting the survival of patients with early stage gastric cancer and evaluated its power for predicting the survival after gastric cancer surgery.
-
Materials and Methods: This study reviewed the data of 8,014 patients with stage T1N0~1M0 and T2~3N0M0 gastric cancer who underwent a curative gastrectomy without adjuvant chemotherapy between January 2006 and December 2015. The log-rank test on SAS was conducted to determine the preoperative PNI cut-off value that indicated the most significant difference in survival, and the clinical features and oncological outcomes were analyzed according to the cut-off value of the preoperative PNI.
-
Results: The preoperative PNI cut-off value that indicated the most significant difference in survival was 43.7. Using this cut-off value, patients were classified into high PNI and low PNI groups. The five-year overall survival rate was 96.9% and 81.5% for the high and low PNI group, respectively (P<0.001). Considering each stage (Ia, Ib, and IIa), the overall survival rates were significantly higher for the high PNI group than the low PNI group. Multivariable analysis revealed the cut-off value of the preoperative PNI to be among the independent risk factors for survival.
-
Conclusions: The cut-off value of the preoperative PNI that could be used to determine the significant differences in the survival of patients with early stage gastric cancer was identified and proven to have a significant impact on predicting survival.
INTRODUCTION
Although the incidence of gastric cancer has decreased in most parts of the world, it is still the 5th most common malignancy and the 2nd most common cause of cancer death worldwide.[1] However, owing to the development of screening programs, the diagnosis of early gastric cancer has increased and the survival outcomes are excellent,[2,3] indicating that adequate postoperative care as well as the choice of the surgical procedure are becoming increasingly important in the field of gastric cancer treatment.
The nutritional status of patients has received much attention as a potential prognostic factor in cancer treatment including gastric cancer.[4,5] Even though the prognostic impact of the nutritional status in patients with gastric cancer was not considered to be as important as the pathological tumor stage, we previously showed that various nutritional parameters were associated with the survival of patients with gastric cancer.[5] Unlike tumor stage, as the nutritional status of patients can be improved by physicians, and because most patients with gastric cancer reduce their food intake and experience weight loss and intestinal malabsorption after gastric surgery, surgeons should focus on the postoperative dietary and gastrointestinal symptoms as well as the nutritional status of patients with gastric cancer to improve the quality of life.
The significance of the prognostic nutritional index (PNI) has been widely reported and confirmed in many types of cancers. For example, in gastric cancer, a lower PNI was associated with a more aggressive tumor, higher recurrence, poor overall survival, and higher risk of postoperative complications.[6-8] Moreover, some authors have suggested the optimal cut-off value of the PNI for predicting the survival of patients with gastric cancer.[7] However, the PNI values are not widely used in clinical practice for gastric cancer because the aggressive nature of the tumor and the need for adjuvant chemotherapy followed by surgery were important factors that resulted in better survival and the association between nutritional status and tumor aggressiveness is not clear.
Therefore, in this study, we enrolled patients with early stage gastric cancer, that is stage Ia (T1N0M0), Ib (T2N0M0, T1N1M0), and only T3N0M0 out of stage IIa—who are free from the effects of the aggressive nature of the tumor and the need for adjuvant chemotherapy—to evaluate the prognostic impact of the nutritional status.
MATERIALS AND METHODS
Between January 2006 and December 2015, the data of 8,014 patients with stage Ia (T1N0M0), Ib (T2N0M0, T1N1M0), and only T3N0M0 out of stage IIa gastric cancer who underwent curative gastrectomy without adjuvant chemotherapy were retrospectively collected and reviewed. Tumors were staged according to the 7th American Joint Committee on Cancer Staging System.[9] Patients with a previous history of other malignancy, gastric surgery, neoadjuvant chemotherapy, or radiotherapy were excluded.
The clinical data included age, gender, preoperative body weight, body mass index (BMI), American Society of Anesthesiologists (ASA) score, resection extent (subtotal vs. total gastrectomy), approach method (open vs. minimally invasive), laboratory results indicative of the nutritional status such as the serum albumin, hemoglobin, total protein, and cholesterol levels and the prognostic nutritional index (PNI). The PNI was calculated preoperatively and 3, 6, and 12 months postoperatively by using the following equation: PNI=[10×serum albumin (g/dL)]+[0.005×total lymphocyte count]. The tumor characteristics included the tumor location (lower, middle, upper, or whole stomach), tumor size, histological type, Lauren classification, and tumor stage.
To calculate the preoperative PNI value that indicated the most significant difference in survival, we used the log-rank test of SAS. As P-values are close to zero, we used the formula “-log10 (P-value)” to obtain a negative value for ease of interpretation. When the value of the “-log10 (P-value)” is the highest, i.e., when the P-value is the smallest, the preoperative PNI at that point is considered to be the cut-off value. On the basis of the results of this analysis, the point with the smallest P-value was selected as the optimal value of the preoperative PNI. Then, patients were divided into two groups according to the cut-off value of the PNI. Several clinicopathological characteristics and long-term outcome of the two groups were compared by using the SPSS statistical software, version 24 (Chicago, IL, USA). The continuous variables between the groups were compared using the independent t-test, and the categorical data were analyzed by using the chi-squared test. The overall survival rate was estimated using Kaplan–Meier survival curves. The association between potential risk factors and outcomes and the independent effects on overall survival rate were evaluated by using Cox proportional-hazards regression analysis. The differences with P-values <0.05 were considered statistically significant.
RESULTS
Table 1 shows the baseline demographic, clinical, laboratory, perioperative, and pathologic characteristics of the 8,014 patients. Fig. 1 shows the preoperative PNI value that indicated the most significant difference in survival; the cut-off value was 43.7. Using the calculated cut-off value of the preoperative PNI, patients were divided into the high PNI group (n=7870) and the low PNI group (n=144). As shown in Table 2, the low PNI group included patients with older age, lower BMI, higher ASA score, and lower serum albumin, hemoglobin, total protein, and cholesterol levels compared to the high PNI group. In addition, the low PNI group had larger tumors, deeper depth of tumor invasion, and higher proportion of differentiated histology and intestinal type gastric cancer compared to the high PNI group.
Table 1
Baseline clinicopathological characteristics of the entire patient population (n=8014)
Fig. 1
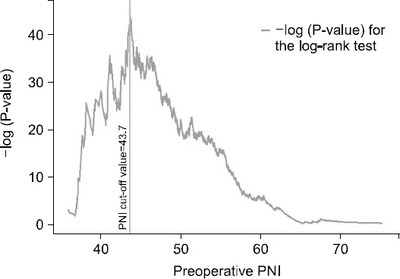
Results of the log-rank test to calculate the cut-off value of the preoperative prognostic nutritional index (PNI).
Table 2
Characteristics of the two groups
Fig. 2 shows the survival curves of patients according to the cut-off value of the preoperative PNI. Among all patients, the 5-year overall survival rate was 96.9% for the high PNI group and 81.5% for the low PNI group (Fig. 2A, P<0.001). In addition, the overall survival rates were significantly higher in the high PNI group than in the low PNI group considering stage Ia (Fig. 2B, 97.6% vs. 82.4%), stage Ib (Fig. 2C, 95.0% vs. 77.8%) and stage IIa (Fig. 2D, 85.2% vs. 81.0%). A significant association was identified between the preoperative PNI and overall survival rate.
Fig. 2
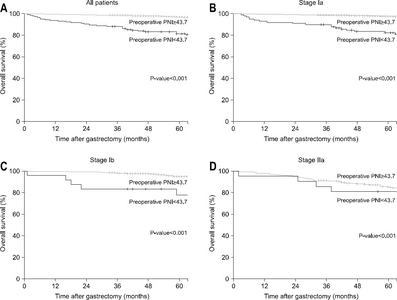
Survival curves according to the preoperative prognostic nutritional index (PNI) values. (A) in all patients with gastric cancer. (B) in patients with stage Ia gastric cancer. (C) in patients with stage Ib gastric cancer. (D) in patients with stage IIa gastric cancer.
On univariable analysis, old age, male sex, low preoperative PNI, low BMI, total gastrectomy, high ASA score, advanced stage, differentiated histology, low PNI at 3, 6, and 12 months postoperatively were significantly associated with worse prognosis, as shown in Table 3. On multivariable analysis using a Cox regression model, the low preoperative PNI (<43.7) was among the independent risk factors predicting poor survival.
Table 3
Univariable and multivariable analyses for overall survival
DISCUSSION
The perioperative nutritional status is associated with short- and long-term outcomes after surgery in patients with cancer.[10-13] Malnutrition is a risk factor for surgical site infection; it results in decreased immune function and induces alterations in the inflammatory response, thereby delaying wound healing and lengthening hospital stay.[14,15] Because most patients reduce their food intake and experience weight loss and intestinal malabsorption after gastric cancer surgery,[4] they are susceptible to being malnourished; therefore, gastric surgeons should focus on postoperative weight loss and the nutritional status to improve the quality of life of patients.
In the current study, we focused on the long-term survival of patients with early stage gastric cancer considering the nutritional status. In advanced gastric cancer, the tumor stage is the strongest predictive factor for tumor recurrence and survival, and advanced cancer is associated with gastrointestinal symptoms, weight loss, and cachexia. Moreover, adjuvant chemotherapy can also affect the nutritional status of patients with symptoms of anorexia, vomiting, abdominal pain, and diarrhea. Therefore, we included patients with early tumor stage, that is stage Ia (T1N0M0), Ib (T2N0M0, T1N1M0), and only T3N0M0 out of stage IIa, thereby omitting the effects of tumor stage and chemotherapy on the nutritional status and survival of patients.
The cut-off values of the PNI for postoperative survival of patients with gastric cancer have been calculated in previous studies by using the criteria of low 10 percentile, mean value, or multiple logistic regression analysis. [7,8,11,16-18] In the current study, we selected the cut-off value of the PNI that indicated the most significant difference in survival on the log-rank test. Even though the calculated cut-off values are different across studies, the constant result is that a low PNI is associated with worse survival compared to a high PNI. When we classified patients into two groups on the basis of the preoperative PNI cut-off value of 43.7, the low PNI group had older age, lower BMI, larger tumor size, and deeper depth of tumor invasion, indicating the presence of a more advanced tumor. In addition, the overall survival rate was significantly better in the high PNI group among all patients and considering each stage (Ia, Ib, and IIa). On multivariable analysis, the preoperative PNI was a significant prognostic factor for overall survival and the postoperative PNI was not shown to be as important as the preoperative PNI.
Although the current retrospective study included a large number of patients, the number of patients in the low PNI group was very small and there was a huge discrepancy in the distribution of patients between the two groups. Moreover, because our results were similar even after propensity score matching, we have not shown those results. In addition, we only evaluated the association between overall survival and the preoperative PNI and not the association between the cancer-specific survival or disease-free survival and the preoperative PNI. Accordingly, considering that comorbidities and other causes of death are important factors that influence the overall survival of patients with early stage gastric cancer, it would be better to analyze the association between the preoperative PNI and tumor recurrence and cancer-specific survival to evaluate the oncological effect of the preoperative PNI in patients with gastric cancer after surgery.
Using the PNI value is a very easy method to determine the nutritional status as well as predict patient survival and postoperative complications. Because the preoperative nutritional status can be improved via oral or parenteral supplementation, surgeons can reduce the risk of developing postoperative complications and improve the short-term and long-term outcomes of patients. Even though other factors such as age, sex, tumor stage, and histology were significant for predicting overall survival on multivariable analysis, the only modifiable factor before surgery is the nutritional status. Therefore, although the postoperative PNI values were not significant prognostic factors in our study, we should evaluate the association between the postoperative PNI and survival of patients with advanced gastric cancer who receive adjuvant chemotherapy after surgery.
In conclusion, the preoperative PNI was an independent prognostic factor in patients with stage I and IIa (only T3N0M0 out of stage IIa) gastric cancer who underwent curative gastrectomy without adjuvant chemotherapy. Surgeons should pay attention to the nutritional status of patients with gastric cancer before surgery and make an effort to improve it, especially in patients with a low PNI value (<43.7).
DISCLOSURE
The authors have no conflicts of interest, financial or otherwise.
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394-424. ArticlePubMedPDF
- 2. Jun JK, Choi KS, Lee HY, Suh M, Park B, Song SH, et al. Effectiveness of the Korean National Cancer Screening Program in reducing gastric cancer mortality. Gastroenterology 2017;152:1319-28. e7.ArticlePubMed
- 3. Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3):analysis of individual records for 37 513?025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018;391:1023-75. PubMedPMC
- 4. Rogers C. Postgastrectomy nutrition. Nutr Clin Pract 2011;26:126-36. ArticlePubMedPDF
- 5. Oh SE, Choi MG, Seo JM, An JY, Lee JH, Sohn TS, et al. Prognostic significance of perioperative nutritional parameters in patients with gastric cancer. Clin Nutr 2019;38:870-6. ArticlePubMed
- 6. Li J, Xu R, Hu DM, Zhang Y, Gong TP, Wu XL. Prognostic nutritional index predicts outcomes of patients after gastrectomy for cancer:a systematic review and meta-analysis of nonrandomized studies. Nutr Cancer 2019;71:557-68. ArticlePubMed
- 7. Sasahara M, Kanda M, Ito S, Mochizuki Y, Teramoto H, Ishigure K, et al. The preoperative prognostic nutritional index predicts short-term and long-term outcomes of patients with stage II/III gastric cancer:analysis of a multi-institution dataset. Dig Surg doi:10.1159/000497454. [In press]. ArticlePDF
- 8. Migita K, Takayama T, Saeki K, Matsumoto S, Wakatsuki K, Enomoto K, et al. The prognostic nutritional index predicts long-term outcomes of gastric cancer patients independent of tumor stage. Ann Surg Oncol 2019;2013;20:2647-54. ArticlePubMedPDF
- 9. Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. 7th ed. New York: Wiley-Blackwelly; 2011.
- 10. Loan BTH, Nakahara S, Tho BA, Dang TN, Anh LN, Huy ND, et al. Nutritional status and postoperative outcomes in patients with gastrointestinal cancer in Vietnam:a retrospective cohort study. Nutrition 2018;48:117-21. ArticlePubMed
- 11. Kanda M, Mizuno A, Tanaka C, Kobayashi D, Fujiwara M, Iwata N, et al. Nutritional predictors for postoperative short-term and long-term outcomes of patients with gastric cancer. Medicine (Baltimore) 2016;95:e3781.ArticlePubMedPMC
- 12. Lee H, Cho YS, Jung S, Kim H. Effect of nutritional risk at admission on the length of hospital stay and mortality in gastrointestinal cancer patients. Clin Nutr Res 2013;2:12-8. ArticlePubMedPMC
- 13. van Stijn MF, Korkic-Halilovic I, Bakker MS, van der Ploeg T, van Leeuwen PA, Houdijk AP. Preoperative nutrition status and postoperative outcome in elderly general surgery patients:a systematic review. JPEN J Parenter Enteral Nutr 2013;37:37-43. PubMed
- 14. Fukuda Y, Yamamoto K, Hirao M, Nishikawa K, Maeda S, Haraguchi N, et al. Prevalence of malnutrition among gastric cancer patients undergoing gastrectomy and optimal preoperative nutritional support for preventing surgical site infections. Ann Surg Oncol 2015;22(Suppl 3):S778-85. ArticlePubMedPDF
- 15. Cheng Y, Zhang J, Zhang L, Wu J, Zhan Z. Enteral immunonutrition versus enteral nutrition for gastric cancer patients undergoing a total gastrectomy:a systematic review and meta-analysis. BMC Gastroenterol 2018;18:11.ArticlePubMedPMCPDF
- 16. Hirahara N, Tajima Y, Fujii Y, Kaji S, Yamamoto T, Hyakudomi R, et al. Prognostic nutritional index as a predictor of survival in resectable gastric cancer patients with normal preoperative serum carcinoembryonic antigen levels:a propensity score matching analysis. BMC Cancer 2018;18:285.ArticlePubMedPMCPDF
- 17. Lee JY, Kim HI, Kim YN, Hong JH, Alshomimi S, An JY, et al. Clinical significance of the prognostic nutritional index for predicting short- and long-term surgical outcomes after gastrectomy:a retrospective analysis of 7781 gastric cancer patients. Medicine (Baltimore) 2016;95:e3539.PubMedPMC
- 18. Song S, Liu H, Xue Y. [Clinical significance of prognostic nutritional index in patients with advanced gastric cancer]. Zhonghua Wei Chang Wai Ke Za Zhi 2018;21:180-4; Chinese. PubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteClinical Implications of the Cut-off Value of the Preoperative Prognostic Nutritional Index in Patients with Early Stage Gastric Cancer
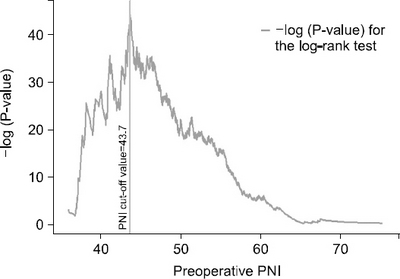
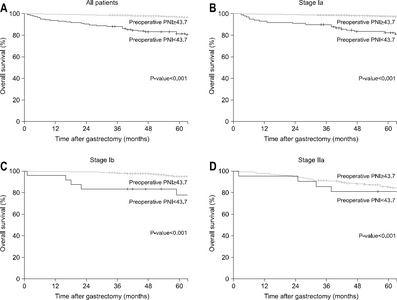
Fig. 1
Results of the log-rank test to calculate the cut-off value of the preoperative prognostic nutritional index (PNI).
Fig. 2
Survival curves according to the preoperative prognostic nutritional index (PNI) values. (A) in all patients with gastric cancer. (B) in patients with stage Ia gastric cancer. (C) in patients with stage Ib gastric cancer. (D) in patients with stage IIa gastric cancer.
Fig. 1
Fig. 2
Clinical Implications of the Cut-off Value of the Preoperative Prognostic Nutritional Index in Patients with Early Stage Gastric Cancer
Baseline clinicopathological characteristics of the entire patient population (n=8014)
| Mean±SD | |
|---|---|
| Age (years) | 57.2±11.6 |
| Sex | |
| Male | 5118 (63.9) |
| Female | 2896 (36.1) |
| Preoperative body weight (kg) | 64.4±10.6 |
| BMI (kg/m2) | 24.1±3.0 |
| ASA score | |
| 1 | 3713 (46.3) |
| 2 | 4125 (51.5) |
| 3 | 176 (2.2) |
| Preoperative albumin level (g/dL) | 4.4±0.4 |
| Preoperative hemoglobin level (g/dL) | 13.9±1.7 |
| Preoperative total protein level (g/dL) | 7.0±0.5 |
| Preoperative cholesterol level (mg/dL) | 185.4±36.1 |
| Preoperative PNI | 54.9±5.1 |
| Resection extent | |
| Subtotal gastrectomy | 6668 (83.2) |
| Total gastrectomy | 1346 (16.8) |
| Surgical approach | |
| Open | 6208 (77.5) |
| Minimally invasive | 1806 (22.5) |
| Tumor location in the stomach | |
| Lower | 4594 (57.3) |
| Middle | 2454 (30.6) |
| Upper | 960 (12.0) |
| Whole | 6 (0.1) |
| Tumor size (cm) | 3.0±1.9 |
| T stage | |
| T1 | 7126 (88.9) |
| T2 | 698 (8.7) |
| T3 | 190 (2.4) |
| N stage | |
| N0 | 7707 (96.2) |
| N1 | 269 (3.3) |
| N2 | 38 (0.5) |
| WHO classification | |
| Differentiated | 3449 (43.0) |
| Undifferentiated | 4565 (57.0) |
| Lauren classification | |
| Intestinal | 3676 (45.9) |
| Diffuse | 3434 (42.8) |
| Mixed | 904 (11.3) |
BMI = body mass index; ASA = American Society of Anesthesiologists; PNI = prognostic nutritional index; WHO = World Health Organization.
Characteristics of the two groups
| Pre-op PNI<43.7 (n=144) | Pre-op PNI≥43.7 (n=7870) | P-value | |
|---|---|---|---|
| Age (years) | 65.9±11.1 | 57.0±11.6 | <0.001 |
| Sex | 0.856 | ||
| Male | 93 (64.6) | 5025 (63.9) | |
| Female | 51 (35.4) | 2845 (36.1) | |
| Preoperative body weight (kg) | 59.9±9.9 | 64.5±10.6 | <0.001 |
| BMI (kg/m2) | 23.3±3.2 | 24.1±3.0 | <0.001 |
| ASA score | <0.001 | ||
| 1 | 29 (20.1) | 3684 (46.8) | |
| 2 | 90 (62.5) | 4035 (51.3) | |
| 3 | 25 (17.4) | 151 (1.9) | |
| Preoperative albumin level (g/dL) | 3.4±0.3 | 4.4±0.3 | <0.001 |
| Preoperative hemoglobin level (g/dL) | 11.5±2.0 | 14.0±1.6 | <0.001 |
| Preoperative total protein level (g/dL) | 6.1±0.7 | 7.0±0.5 | <0.001 |
| Preoperative cholesterol level (mg/dL) | 152.0±34.8 | 186.0±35.9 | <0.001 |
| Preoperative PNI | 40.7±2.8 | 55.1±4.8 | NA |
| Resection extent | 0.683 | ||
| Subtotal gastrectomy | 118 (81.9) | 6550 (83.2) | |
| Total gastrectomy | 26 (18.1) | 1320 (16.8) | |
| Surgical approach | <0.001 | ||
| Open | 139 (96.5) | 6069 (77.1) | |
| Minimally invasive | 5 (3.5) | 1801 (22.9) | |
| Tumor location in the stomach | 0.830 | ||
| Lower | 86 (59.7) | 4508 (57.3) | |
| Middle | 44 (30.6) | 2410 (30.6) | |
| Upper | 14 (9.7) | 946 (12.0) | |
| Whole | 0 (0.0) | 6 (0.1) | |
| Tumor size (cm) | 4.2±2.8 | 3.0±1.9 | <0.001 |
| T stage | <0.001 | ||
| T1 | 103 (71.5) | 7023 (89.2) | |
| T2 | 24 (16.7) | 674 (8.6) | |
| T3 | 17 (11.8) | 173 (2.2) | |
| N stage | 0.797 | ||
| N0 | 137 (95.1) | 7570 (96.2) | |
| N1 | 6 (4.2) | 263 (3.3) | |
| N2 | 1 (0.7) | 37 (0.5) | |
| WHO classification | <0.001 | ||
| Differentiated | 98 (68.1) | 3351 (42.6) | |
| Undifferentiated | 46 (31.9) | 4519 (57.4) | |
| Lauren classification | <0.001 | ||
| Intestinal | 99 (68.8) | 3577 (45.5) | |
| Diffuse | 33 (22.9) | 3401 (43.2) | |
| Mixed | 12 (8.3) | 892 (11.3) |
Pre-op = preoperative; PNI = prognostic nutritional index; BMI = body mass index; ASA = American Society of Anesthesiologists; WHO = World Health Organization.
Univariable and multivariable analyses for overall survival
| Risk factor | Univariable analysis | Multivariable analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | |||
| Age | 1.100 | 1.088 | 1.112 | <0.001 | 1.084 | 1.071 | 1.097 | <0.001 |
| Sex | ||||||||
| Male | ref. | ref. | ||||||
| Female | 0.411 | 0.318 | 0.531 | <0.001 | 0.428 | 0.331 | 0.555 | <0.001 |
| Preoperative PNI | ||||||||
| <43.7 | 7.109 | 5.175 | 9.766 | <0.001 | 2.925 | 2.103 | 4.067 | <0.001 |
| ≥43.7 | ref. | ref. | ||||||
| BMI | 0.924 | 0.892 | 0.957 | <0.001 | 0.940 | 0.906 | 0.976 | 0.001 |
| Resection extent | ||||||||
| Subtotal | ref. | ref. | ||||||
| Total | 1.338 | 1.044 | 1.714 | 0.021 | 1.134 | 0.882 | 1.457 | 0.327 |
| ASA score | ||||||||
| 1 | ref. | ref. | ||||||
| 2 | 2.541 | 2.003 | 3.222 | <0.001 | 1.160 | 0.899 | 1.497 | 0.254 |
| 3 | 10.151 | 7.011 | 14.698 | <0.001 | 2.572 | 1.738 | 3.807 | <0.001 |
| Stage | ||||||||
| Ia | ref. | ref. | ||||||
| Ib | 2.044 | 1.550 | 2.696 | <0.001 | 1.404 | 1.061 | 1.857 | 0.018 |
| IIa | 5.050 | 3.792 | 6.725 | <0.001 | 2.455 | 1.826 | 3.302 | <0.001 |
| WHO classification | ||||||||
| Differentiated | ref. | ref. | ||||||
| Undifferentiated | 0.477 | 0.388 | 0.587 | <0.001 | 1.200 | 0.869 | 1.657 | 0.267 |
| Lauren classification | ||||||||
| Intestinal | ref. | ref. | ||||||
| Diffuse | 0.363 | 0.285 | 0.463 | <0.001 | 0.690 | 0.477 | 0.998 | 0.049 |
| Mixed | 0.617 | 0.432 | 0.883 | 0.008 | 0.765 | 0.506 | 1.157 | 0.205 |
| Postoperative PNI | ||||||||
| 3 months | 0.887 | 0.869 | 0.906 | <0.001 | ||||
| 6 months | 0.883 | 0.861 | 0.907 | <0.001 | ||||
| 12 months | 0.897 | 0.872 | 0.923 | <0.001 | ||||
HR = hazard ratio; CI = confidence interval; PNI = prognostic nutritional index; BMI = body mass index; ASA = American Society of Anesthesiologists; WHO = World Health Organization.
Table 1 Baseline clinicopathological characteristics of the entire patient population (n=8014)
BMI = body mass index; ASA = American Society of Anesthesiologists; PNI = prognostic nutritional index; WHO = World Health Organization.
Table 2 Characteristics of the two groups
Pre-op = preoperative; PNI = prognostic nutritional index; BMI = body mass index; ASA = American Society of Anesthesiologists; WHO = World Health Organization.
Table 3 Univariable and multivariable analyses for overall survival
HR = hazard ratio; CI = confidence interval; PNI = prognostic nutritional index; BMI = body mass index; ASA = American Society of Anesthesiologists; WHO = World Health Organization.

