 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 15(3); 2023 > Article
- Original Article Comparative assessment of nutritional characteristics of critically ill patients at admission and discharge from the neurosurgical intensive care unit in Korea: a comparison study
-
Eunjoo Bae1
 , Jinyoung Jang2, Miyeon Kim3, Seongsuk Kang3, Kumhee Son4,5, Taegon Kim2, Hyunjung Lim4,5
, Jinyoung Jang2, Miyeon Kim3, Seongsuk Kang3, Kumhee Son4,5, Taegon Kim2, Hyunjung Lim4,5 -
Annals of Clinical Nutrition and Metabolism 2023;15(3):97-108.
DOI: https://doi.org/10.15747/ACNM.2023.15.3.97
Published online: December 1, 2023
1Department of Food and Nutrition, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
2Department of Neurosurgery, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
3Department of Nursing, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
4Department of Medical Nutrition, Graduate School of East-West Medical Science, Kyung Hee University, Yongin, Korea
5Research Institute of Medical Nutrition, Kyung Hee University, Seoul, Korea
- Corresponding author: Hyunjung Lim, email: hjlim@khu.ac.kr
- Co-Corresponding author: Taegon Kim, email: tgkim@chamc.co.kr
• Received: July 13, 2023 • Revised: October 25, 2023 • Accepted: October 30, 2023
© 2023 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 5,452 Views
- 40 Download
- 4 Crossref
Abstract
-
Purpose Patients in neurosurgical (NS) intensive care units (ICUs) experience considerable energy and protein deficits associated with adverse outcomes. This study aimed to compare the nutritional status of patients at admission to (baseline) and discharge from the NS ICU.
-
Methods This was a single-center, retrospective, before and after study of patients admitted in the NS ICU of the CHA Bundang Medical Center, from January 31, 2019, to February 28, 2020. All anthropometric data, biochemical data, clinical data, and dietary data were collected during the NS ICU stay. Specifically, we investigated the cumulative caloric deficit rate, phase angle and skeletal muscle index as indicators of lean muscle mass, and nitrogen balance according to demographic and clinical characteristics.
-
Results A total of 140 NS patients were studied. Calf circumference decreased from 31.4±4.2 cm at baseline to 30.2±4.0 cm at discharge (P<0.001). Energy supply rate increased from 44.4% at baseline to 89.2% at discharge. Phase angle (PhA) patients with an modified Nutrition Risk in the Critically ill (mNUTRIC) score≤5 group had significantly lower PhA values than those with an mNUTRIC score>5 (P=0.005).
-
Conclusion Although clinical and dietary parameters of patients in the NS ICU improved from baseline to discharge, anthropometric and biochemical markers of lean muscle mass and nutritional status decreased. PhA and nitrogen balance difference values were significantly different between those with an mNUTRIC score≤5 and those with an mNUTRIC score>5. These data indicate that the nutritional risk of critically ill patients increases during hospitalization in the NS ICU.
Introduction
Patients in neurosurgical (NS) intensive care units (ICUs) have individual nutrition-related requirements related to their condition. It is challenging, however, for medical staff to assess the nutritional requirements of individuals [1]. Observational data consistently show that during the initial phase after moderate or severe traumatic brain injury, patients are substantially underfed in the ICU, similar to critically ill patients admitted with other diagnoses [2].
Confusion, delirium, fasting for repeated procedures, and swallowing difficulties are prevalent in patients after a brain injury and are risk factors for persistent energy and protein deficits [3]. In an Australian study, only 87% of the energy and 70% of the protein requirements of 37 patients admitted to the NS ICU were met over a 21-day period [4]. These energy and protein shortfalls in patients with brain injury can result in malnutrition, which is in turn associated with adverse outcomes such as a longer duration of hospital stay before admission to a rehabilitation facility and unfavorable neurological findings at 6 months [5]. Conversely, critically ill patients whose energy requirements are achieved early during ICU admission have better self-reported physical function 6 months after ICU discharge [6]. Patients who survive critical illnesses frequently develop muscle weakness, termed ICU-acquired weakness (ICU-AW). ICU-AW is associated with diminished physical function, lower health-related quality of life, increased ICU and hospital length of stay, increased healthcare costs, and mortality [7].
Critically ill NS patients are at high nutritional risk as they are in a catabolic state associated with neurological injury and because they are dependent on enteral nutrition (EN) [8]. Patients with either primary or secondary NS disorders are susceptible to nutrition risk. There is a lack of research on the provision of nutritional support for patients with a neurological injury [9]. In addition, few studies have precisely quantified the energy and protein deficits of critically ill patients [10].
The primary aim of this study was to compare patients’ nutritional status at baseline and at discharge from the NS ICU based on assessment of anthropometric, biochemical, clinical, and dietary data. The second aim was to compare changes between cumulative calorie rates, two anthropometric variables (phase angle and skeletal muscle index), and nitrogen balance according to the demographic and clinical characteristics of NS ICU patients.
Methods
The ethics committee of CHA Bundang Medical Center approved the protocol (2021-02-018). The study was registered with the Clinical Research Information Service (KCT0006244) at https://cris.nih.go.kr/. Because the study was a retrospective study, written informed consent was not obtained from patients, and the requirement for informed consent was waived by the Ethics Committee.
It is a before and after study based on the retrospective chart review. It is described according to the STROBE statement (https://www.strobe-statement.org/).
This comparison study was done in CHA Bundang Medical Center from January 31, 2019, to February 28, 2020. The comparative analysis date of ICU baseline and discharge was the third day of admission to the ICU and the day before discharge from the ICU, respectively. Total analysis period during ICU admission was from the first day of ICU admission to the day before ICU discharge.
Among patients admitted to the NS ICU in Cha Bundang Medical Center during the study period, 140 patients who met the inclusion criteria were analyzed. Inclusion criteria were age≥19 years, mechanical ventilation commenced within 48 hours of ICU admission and likely to be required >48 hours, an estimated minimum stay in the ICU of at least 3 days, and nutrition received through enteral or parenteral routes. Exclusion criteria were age<19 years, discharge or death within 2 days of admission to the ICU, no need for a mechanical ventilator, and oral intake at least once during the ICU admission period rather than EN or parenteral nutrition (PN).
Weight was determined using a bed scale (IBS-200, CASKOREA). Height was measured using a tape measure. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters (kg/m2), and patients were categorized as underweight (<18.5 kg/m2) or normal weight (18.5–22.9 kg/m2) vs. overweight (23.0–24.9 kg/m2) and obese (≥25 kg/m2) based on Asian-Pacific cutoff points [11]. A trained dietitian measured calf circumference (cm), triceps skinfold thickness (TSF, mm), mid-upper arm muscle circumference (MAMC, cm), and mid-upper arm muscle area (MAMA, cm2) as markers of lean muscle mass. Body composition was analyzed using a portable bioelectrical impedance device (InBody S10®; InBody). Bioelectric impedance analysis (BIA) was performed as early as possible after ICU admission, usually on the first day after admission to the ICU, at bare minimum within the first 48 hours, and every 7 days thereafter until ICU discharge. This device consists of eight electrodes attached to the arms, legs, and trunk with 6 different frequencies (1, 5, 50, 250, 500, and 1,000 kHz) used to measure impedance. Patients were measured in a prone position on a bed with their arms and legs abducted from the body. Source and sensor electrodes were placed on the thumb and index finger of both hands and each ankle. Before attaching the electrodes, contact areas were cleaned with alcohol. Phase angle (PhA, °) values were obtained from the resistance (R) and reactance (Xc) using the following equation: PhA (°)=arctan (Xc/R)×(180π). The sum of lean masses of the arms and legs was used to define the appendicular lean mass (ALM). Skeletal muscle index (SMI) was calculated by dividing the ALM by height squared. PhA and SMI were determined immediately after ICU admission and before ICU discharge. SMI was calculated as appendicular skeletal muscle mass/height (m2).
The following data were collected via a web-based electronic case report form: blood chemistry (serum albumin) values and 24-hour urine collection (urea nitrogen, creatinine clearance) on day three and at ICU discharge. Nitrogen balance (g/day) was calculated using the following formula: nitrogen intake (g/day)–urinary urea nitrogen (g/day)–insensible nitrogen losses (4 g/day).
Clinical data were also collected via a web-based electronic case report form: medical history related to diagnosis, including comorbidities; surgery; modified Nutrition Risk in the Critically ill (mNUTRIC) score; Acute Physiology and Chronic Health Evaluation (APACHE) II score; Sequential Organ Failure Assessment (SOFA) score; Simplified Acute Physiology Score (SAPS) III; Glasgow Coma Scale (GCS); Braden Scale score; and pressure ulcer occurrence on day three and at ICU discharge. The Braden Scale was applied daily until discharge from the ICU by a nurse researcher. mNUTRIC is a nutritional risk assessment tool validated for use in critically ill patients. An mNUTRIC score≤5 corresponds to low nutritional risk while one >5 corresponds to high nutritional risk [12]. The severity of illness was evaluated by APACHE II, SOFA, and SAPS III scores. Level of consciousness was assessed by the GCS score. Pressure ulcer risk was measured by the Braden Scale, which classifies risk for pressure ulcers as follows: 0–9 (very high risk), 10–12 (high risk), 13–14 (moderate risk), 15–18 (low risk), and 19–23 (no risk) [13]. Nutritional assessment was evaluated by the International Classification of Diseases, ninth edition, clinical modification malnutrition codes as follows: adequately nourished status, mild malnutrition, moderate malnutrition, or severe malnutrition [14].
Data on nutrition delivered from all routes were collected by a trained dietitian. Information regarding nutrition provided via the enteral and parenteral routes was collected from fluid balance and intravenous fluid charts completed as part of routine care by nursing staff. Amounts of total energy and protein delivered were calculated. Data on energy and protein requirements prescribed as part of the standard care and methods used to calculate requirements were recorded. The dietitian calculated the estimated energy requirements at baseline using a value of 25 kcal/kg/day. Standard care for all participants included a nutritional assessment by a dietitian within 48 hours of admission with an estimation of their nutritional requirements. Commercially available enteral and parenteral formulas were prescribed based on clinical needs as assessed by the dietitian. Daily nutritional energy delivery from EN and PN and nutritional outcome data were collected for the duration of the ICU stay. Cumulative energy deficit of each participant from artificial nutrition support was calculated daily until ICU discharge. Daily energy provision was measured for all patients receiving EN or PN, including energy from intravenous dextrose. Daily energy deficit was determined by deducting the energy delivered from the prescribed energy target determined by the dietitian. Daily energy deficit was summarized as the total cumulative energy deficit. Nutritional adequacy was assessed by dividing the daily energy delivery, including on the day of admission and discharge, by the prescribed requirements, and expressed as a percentage.
There was no selection bias reportable.
Sample size estimation was not done because all target patients were included.
Statistical analysis were performed using IBM SPSS 26 (IBM Corp.). Categorical data are presented as counts and percentages, and continuous data as mean±standard deviation, median (25th–75th percentiles), or as number (%). Continuous variables were evaluated using Student’s t-test. Multivariable generalized linear regression analysis was used to explore associations between dependent variables (cumulative caloric deficit, phase angle, skeletal muscle index, and nitrogen balance) and independent variables (age, gender, mNUTRIC score, BMI and supply percentage of energy requirements). We used a chi-squared test to assess the significance of differences in dichotomous variables between groups, and regression analysis or Wilcoxon’s test for rate and ordinal data as well as data with a non-normal distribution. Energy and protein deficits were calculated as the mean daily absolute difference between intake and estimated requirements. Energy and protein intake, deficits, and the proportion of the estimated nutritional requirements met were calculated for all nutrient sources for the overall study period. The significance of differences in energy and protein delivery, intake, and deficits in the early acute phase vs. later phase as well as EN vs. PN were assessed using independent sample t-tests. A p-value<0.05 was considered statistically significant.
Results
During the study period, a total of 686 patients were admitted to the NS ICU. We excluded 546 patients due to death and/or discharge within 3 days after NS ICU admission (n=38), indication of EN and PN withdrawal (n=267), insufficient clinical data (n=110), no mechanical ventilator care (n=102), and age<19 years (n=29) (Fig. 1). Finally, 140 patients were included in this study. Baseline demographic and clinical characteristics are shown in Table 1. Mean age of patients was 61.9±15.3 years, and 51.4% were males. Average height was 162.9±0.8 cm, and the SAPS III score was 33.6±13.0 points. Primary diagnoses were brain hemorrhage in 101 patients (72.1%), brain tumor in 25 patients (17.9%), and other in 14 patients (10.0%). There were three main reasons for leaving the ICU: 64.3% of patients (n=90) moved to the general ward, 16.4% of the patients (n=23) were transferred to a nursing facility, and 19.3% of patients (n=27) died.
Table 2 shows a comparison of anthropometric, biochemical, and clinical data at baseline and discharge. Weight at baseline (62.3±13.3 kg/m2) and discharge (60.9±12.8 kg/m2) differed significantly (P<0.001). Calf circumference decreased from 31.4±4.2 cm at baseline to 30.2±4.0 at discharge (P<0.001). MAMC decreased from 21.8±3.2 cm at baseline to 20.6±4.0 cm at discharge (P<0.001). PhA decreased from 4.0±1.4° at baseline to 3.7±1.3° at discharge; additionally, SMI also decreased from 5.7±1.1 at baseline to 5.3±1.1 at discharge (P<0.001). Extracellular water (ECW) ratio (ECW/total body water [TBW]) increased significantly from 0.401±0.015 cm at baseline to 0.405±0.014 at discharge (P<0.001). Incidence of pressure ulcers increased from 4.3% (n=6) at baseline to 23.6% (n=33) at the time of discharge (P=0.119). The 4 nutritional classifications differed significantly at baseline and discharge (P<0.001).
Nutritional targets and deficits during the NS ICU hospitalization period are shown in Table 3. The average day on which nutritional support was started after entering the ICU was 1.75±1.0 days. The number of subjects who started EN within 48 hours after ICU admission was 43.6% (n=61). Targets and deficits were examined for the entire study period. A comparison of the 3rd and last day nutrition provision is provided in Table 4. All 12 aspects of calorie and protein intake showed significant differences between the 3rd day and last day (P<0.001). Energy supply rate improved from 42.0% at ICU baseline to 95.3% at ICU discharge. Protein supply rate improved from 45.7% at ICU baseline to 83.0% at ICU discharge. The percentage of EN supply compared to the prescription increased from 0% to 92.8%, and the percentage PN supply compared to the prescribed amount decreased from 22.0% to 0%. EN% of the protein prescription was 0% at baseline, but increased to 80.0% at discharge, and PN% of the prescription was 29.4% at baseline, but decreased to 0% at discharge.
The following groupings of patients were compared: <65 years of age (n=76) vs. ≥65 years of age (n=64), female (n=68) vs. male (n=72), mNUTRIC score≤5 (n=87) vs. mNUTRIC score>5 (n=53), BMI<23 kg/m2 (n=67) vs. BMI≥23 kg/m2 (n=73), supply of 70% or more of energy requirement (n=79) vs. supply of less than 70% of energy requirement (n=61). In Fig. 2A, the cumulative caloric deficit% for ICU stay between these groups was examined. The cumulative caloric deficit% for female was 25.7±26.5% while that for male was 40.8±38.2% (P=0.007). The cumulative caloric deficit% for the BMI<23 kg/m2 group was 24.3±30.2% while that for the BMI≥23 kg/m2 group was 41.8±34.9%, a significant difference (P=0.002). The cumulative caloric deficit% of the supply group with an energy requirement of 70% was 61.3±30.3% while that of the supply group with an energy requirement of less than 70% was 11.9±15.8%. In Fig. 2B, phase angle scores at ICU baseline and discharge are shown. The phase angle score for the mNUTRIC score≤5 group was 0.51±0.99°, while that for the mNUTRIC score>5 group was 0.01±1.14°, a significant difference (P=0.005). SMI differences between ICU baseline and ICU discharge are shown in Fig. 2C. The SMI score of the mNUTRIC score≤5 group was –0.52±1.09 compared to –0.19±1.21 in the mNUTRIC score>5 group, which was not a significant difference (P=0.092). Fig. 2D shows the nitrogen balance difference between ICU baseline and discharge. The nitrogen balance was 4.0 in the mNUTRIC score≤5 group vs. 0.6 in the mNUTRIC score>5 group (P=0.023). Results of multivariable analysis are shown in Tables 5-8. Cumulative caloric deficit% had a beta value of 11.961 in the BMI≥23 kg/m2 group and –48.601 in the >70% supply of energy requirement groups (P=0.003, P<0.001, respectively; Table 5).
As shown in Tables 6 and 8, the difference in phase angle and nitrogen balance between ICU baseline and discharge groups had respectively a beta value of 0.552, and –2.552 in the group with mNUTRIC>5 (P=0.007, P=0.049, respectively).
Discussion
This study compared changes in nutritional status from NS ICU baseline to discharge. Energy supply rate improved by approximately 40% during the late ICU period compared to the early ICU period whereas anthropometric and biochemical data were poorer in the late ICU period than the early ICU period. Nutritional assessment scores differed significantly between the early and late ICU periods and PhA and nitrogen balance values were significantly different between the mNUTRIC score≤5 and mNUTRIC score>5 groups.
In this study, the EN ratio of energy prescriptions increased significantly from baseline to discharge. The ratio of protein supplied through EN also increased from baseline to discharge. Alberda et al. [15] reported that ICU patients worldwide received, on average, less than 60% of the prescribed energy and 56% of the prescribed protein. In our study, patients in the NS ICU baseline received, on average, less than 50% of the prescribed energy and protein; however, patients at ICU discharge received on average more than 80% of the prescribed energy and protein. One study found a significant association between early energy delivery of less than 60% of recommended goal calories and a greater risk of ICU mortality in patients who survived for at least 7 days [16]. In our study, early EN supply was low at less than 50%. Nasogastric tube feeding has been associated with improved clinical outcomes. Intestinal permeability is maintained and bacterial translocation from the intestinal lumen into the bloodstream, which results in septic complications, is less likely [17]. A study in the Netherlands reported that a large group of neurological patients were malnourished and at risk of malnutrition during hospital admission, and the nutritional status of most patients was observed to worsen in 10 days [18]. Therefore, EN should be provided as early as possible to patients admitted to the NS ICU to prevent malnutrition.
Nitrogen balance improved significantly from baseline to discharge. This is likely due to the negative nitrogen balance in the body during protein decomposition in the acute phase at baseline. Patients who are discharged from the ICU are most likely in the stable phase, during which anabolic actions occur. Over the past 25 years, hypermetabolism and nitrogen wasting have been documented in patients with NS with a predicted metabolic expenditure ranging from 120% to 250% [19]. The protein content for NS patients should therefore not be less than 15% of total calories. Critically ill patients may benefit from more than 2 g of amino acid/kg normal body weight per day instead of the 1.5 g of amino acid/kg normal body weight per day recommended by some guidelines [20]. Kreymann et al. [21] stated that determining nutritional requirements in the form of the energy to nitrogen (energy/nitrogen) ratio when planning nutrition provision may help optimize this balance. Therefore, protein demand on ICU admission is an important factor to consider to prevent body protein degradation. In our study, the difference in the nitrogen balance between admission and discharge was significantly higher in the mNUTRIC≤5 group than in the mNUTRIC>5 group. Even if the mNUTRIC score is low, corresponding to a good nutritional status, adequate protein provision should be considered.
The phase angles of all subjects in the present study was substantially lower than existing reference values, reflecting the fact that these patients were critically ill [22]. PhA has been reported to be a more accurate indicator of lean muscle mass than complete body composition as it reflects fat-free mass and cellular integrity [23]. Loss of lean body mass is associated with a worse prognosis in chronic diseases and in critically ill patients [23]. It is still unclear how frequently lean body mass should be evaluated, but it could be helpful to monitor fat mass, especially in chronic critically ill patients [24]. From baseline to discharge, the group with good nutritional status showed a more significant decrease in lean muscle mass than the group with poorer nutritional status. Even in multivariable analysis, the phase angle value showed significant differences according to mNUTRIC score. This indicates that a decrease in muscle mass is likely even in low nutritional risk patients (mNUTRIC≤5); therefore, adequate nutrition needs to be supplied early during a patient’s ICU stay. Identifying patients at risk of adverse events because of their nutritional status is a core competency of nutrition practitioners, recommended by clinical practice guidelines, and mandated by accreditation agencies [25]. Inherent in this discussion of nutrition risk is that the patients at high risk are more likely to benefit from nutritional therapeutic interventions than those at low risk, as demonstrated by Kondrup et al. [26]. However, our study showed that nutritional therapy intervention is also important in patients at low nutritional risk (mNUTRIC score≤5). Indicators of mNUTRIC score include age, APACHE 2 score, SOFA score, complications, and days of ICU stay, which may affect muscle mass reduction. Few studies have investigated mNUTRIC scores in NS patients, and further studies are needed in these patients. A longer follow-up duration will also help provide more insights into how nutritional interventions during an ICU stay affect muscle mass at discharge.
In this study, calf circumference, MAMC, and MAMA levels, which have been reported to be indicators of muscle mass in previous studies [27], were investigated. Due to sedation and loss of consciousness, ventilated ICU patients are unable to provide weight histories or dietary histories early in their ICU admission. They may also not have previously documented nutrition and weight histories [28]. In our study, we measured muscle circumference using a tape measure to determine nutritional status. Calf circumference, MAMC, and MAMA all showed significant decreases from ICU admission to ICU discharge, indicating that muscle mass decreased. In another study, arm muscle circumference was measured in 187 critically ill patients during hospitalization [29]. Sungurtekin et al. [30] reported a strong association between TSF, MAMC, BMI, and ICU mortality in 124 medical/surgical ICU patients. Measurement of muscle circumference using a tape measure allows for easy nutritional evaluation of critically ill patients. However, critically ill patients often have severe edema from vascular tone release or massive fluid resuscitation [31]. Therefore, edema status could be a major limitation of muscle mass assessment in ICU patients. We evaluated the ECW/TBW ratio from BIA. Patients with ECW/TBW≥0.42 have severe edema [31]; in our study, only mild edema (ECW/TBW<0.42) was present at baseline and discharge. BIA enables the determination of fat and fat-free components of the body, but fluid resuscitation complicates the determination of these components, particularly the fat free mass [24].
In this study, the incidence of pressure ulcers at baseline was 4.3%, but increased by approximately 6-fold to 23.6% at ICU discharge. However, this difference was not statistically significant. In two large, multicenter trials with thousands of patients, the incidence of pressure ulcers in ICUs was reported to be 13.5% [32] and 25.1% [33]. This is similar to the results of the present study. Another study reported that BMI and the occurrence of pressure ulcers were related in intensive care patients [34]. In a multicenter study performed in 2017 [35], the incidence of pressure ulcers was found to be related to disease, malnutrition, and hospital stay.
In this study, patients in the NS ICU had different primary diseases such as brain hemorrhage, brain tumor, and others. Acute neurologic damage results in physiological, metabolic, and functional changes [36]. Typically, nutrition risk can persist throughout hospitalization in the NS ICU. The nutrition status of patients affects their disease prognosis. An adequate assessment of nutrition risk should be a standard procedure for patients in NS ICU care, since patients at higher nutrition risk could better benefit from nutrition interventions than those at lower risk [37,38]. Because most of the physiological and metabolic changes are seen during the chronic disease stage rather than the acute stage, patients with various neurological diseases should receive a nutritional evaluation during ICU admission. This study was not a study of a specific disease population and, similar to other studies [39], included subjects with common symptoms of decreased consciousness admitted to NS ICU. However, NS diseases differ according to type of lesion or injury, life expectancy, residual mobility-functionality, and drug treatment and these factors should be considered in future studies [40]. We conducted multivariable analysis of 4 dependent variables and 5 independent variables to determine predictors of poor nutritional status. However, low correlation values were found, possibly due to the small number of subjects included in this study.
Strengths of our research are as follows. First, we compared the muscle mass of critically ill patients using various anthropometric evaluation tools. Although phase angle is an important indicator of muscle mass, it is costly and time-consuming to assess because it must be measured using BIA. Nevertheless, we evaluated nutritional status objectively using phase angle measured by BIA in NS patients and demonstrated its feasibility in clinical application. Second, we compared nutritional status of patients at the early and late stages of ICU admission, rather than performing a cross-sectional evaluation. Third, the significance of the main indicators was clarified by dividing subjects into two groups according to various criteria.
This study also had several limitations. First, our observational data were based on a single NS ICU; thus, our findings may not be generalizable to other populations. Second, this study excluded the population with oral intake because of difficulty in calculating nutritional information because of the lack of data in electronic medical records on oral nutrition provision for the study population. Third, we compared values at baseline and discharge but did not consider differences in patients’ length of stay, which is likely to impact our findings. Finally, the 5 independent variables associated with nutritional status were not significantly associated with any of the demographic or nutritional variables we evaluated. Therefore, it is necessary to conduct further study to find nutritional status markers that were not considered in the present data analysis.
Larger, well-designed randomized controlled trials exploring the role of nutrition provision on clinical outcomes are needed to confirm our findings.
Although nutrition provision increased in critically ill patients during the NS ICU period; lean muscle mass decreased. The change in PhA during the ICU period was significantly greater in the mNUTRIC score≤5 group than in the mNUTRIC score>5 group. This means that the well-nourished group has a greater decrease of lean muscle mass than the non well-nourished group. Nevertheless, if well-nourished patients remain in the hospital for an extended period of time, their nutritional status and long-term functional outcomes are likely to suffer.
Supplementary materials
None.
Acknowledgments
The authors would like to thank nutrition support team members and nurses of the intensive care unit for their critical review of the study as well as many patients who participated in this research.
Authors’ contribution
Conceptualization: EB, HL. Data curation: TK, JJ. Investigation: MK, SK. Methodology: EB, KS. Project administration: HL, TK. Resources: JJ, SK. Software: MK, KS. Supervision: HL, TK. Validation: JJ, SK. Visualization: EB, KS. Writing – original draft: EB, TK. Writing – review & editing: all authors.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Fig. 1
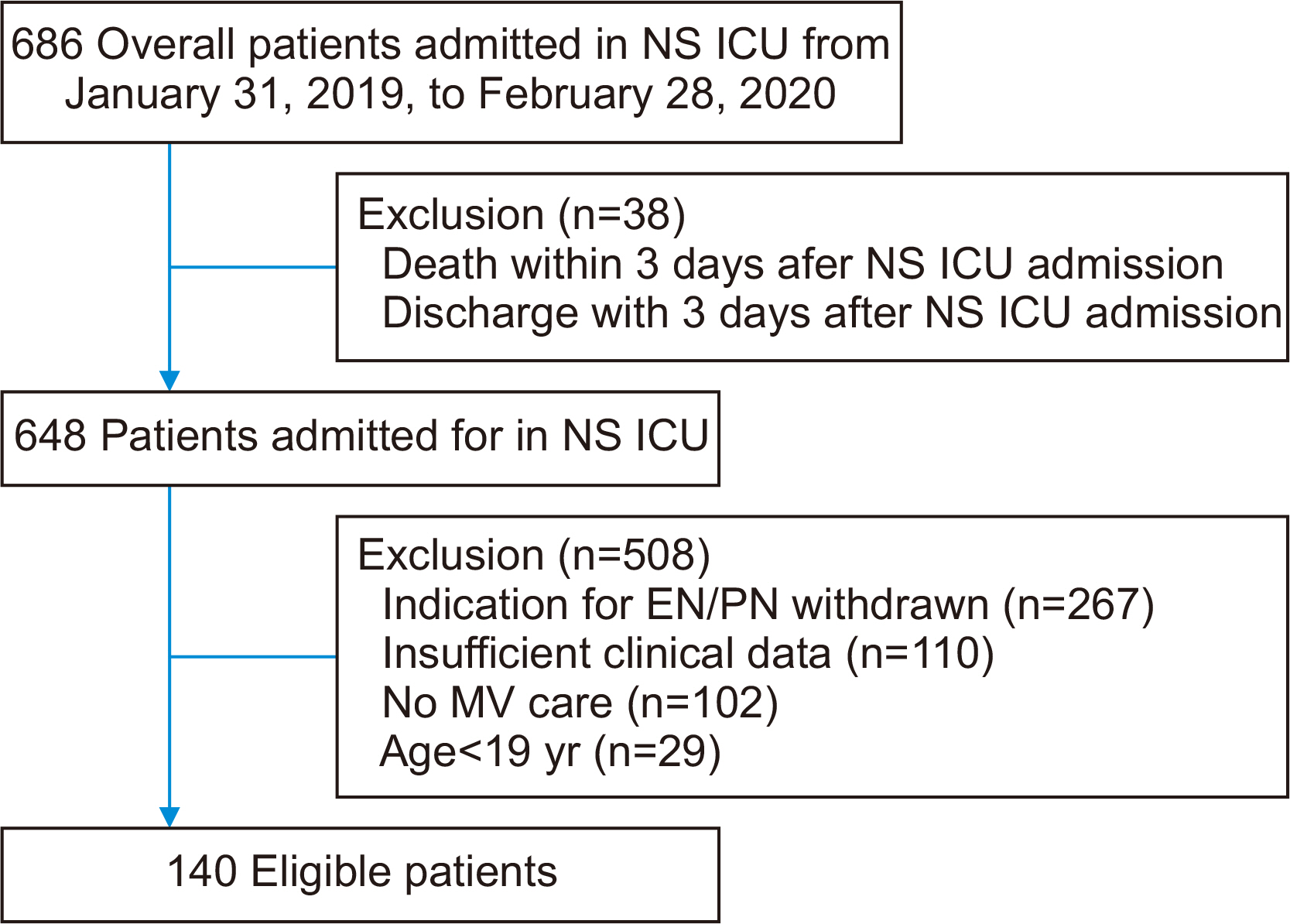
Flow diagram of patients selected for analysis. NS ICU = neurosurgical intensive care unit; EN = enteral nutrition; PN = parenteral nutrition; MV = mechanical ventilator.
Fig. 2
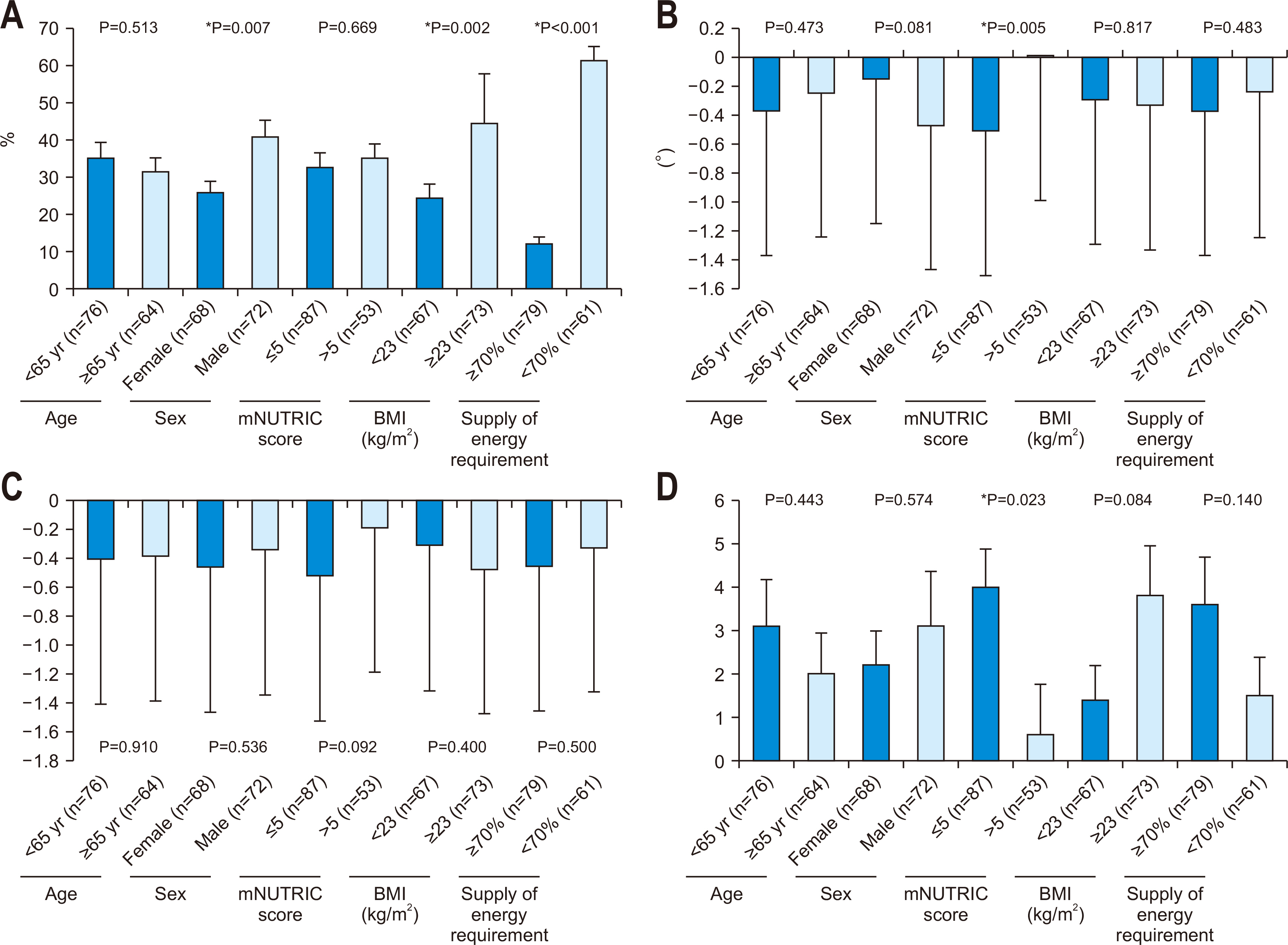
Cumulative caloric deficit, phase angle, skeletal muscle mass index, and nitrogen balance by clinical characteristics. Data shown are the mean cumulative caloric deficit, phase angle, skeletal muscle index, and nitrogen balance. Error bars are standard errors. (A) Cumulative caloric deficit% during the intensive care unit (ICU) period. (B) Change in phase angle between ICU baseline and discharge. (C) Change in skeletal muscle index between ICU baseline and ICU discharge. (D) Change in nitrogen balance between ICU baseline and discharge. mNUTRIC = modified Nutrition Risk in the Critically ill; BMI = body mass index.
Table 1
Baseline demographic and clinical characteristics
| Variable | All patients (n=140) |
|---|---|
| Age (yr) | 61.9±15.3 |
| Sex, male | 72 (51.4) |
| Height (cm) | 162.9±0.8 |
| mNUTRIC score | 5.1±1.4 |
| SAPS III score | 33.6±13.0 |
| Mechanical ventilator (day) | 9.5 (4.0–18.0) |
| Mechanical ventilator mode | |
| PCV | 80 (57.1) |
| PSIMV | 42 (30.0) |
| PSV | 13 (9.3) |
| CMV | 4 (2.9) |
| SIMV | 1 (0.7) |
| Primary diagnosis | |
| Brain hemorrhage | 101 (72.1) |
| Brain tumor | 25 (17.9) |
| Othera | 14 (10.0) |
| NS ICU LOS (day) | 21.0 (11.2–33.7) |
| Hospital LOS (day) | 39.5 (25.0–63.0) |
| NS ICU-free (day) | 14.0 (0.0–33.5) |
| Reason for NS ICU discharge | |
| Inter-hospital transfer | 90 (64.3) |
| Permanent care facility | 23 (16.4) |
| Death | 27 (19.3) |
| Surgeryb | 129 (92.1) |
| Comorbiditiesc | 106 (75.7) |
Values are presented as mean±standard deviation, number (%), or median (25th–75th percentiles).
mNUTRIC = modified Nutrition Risk in the Critically ill; SAPS = Simplified Acute Physiology Score; PCV = pressure-targeted controlled mandatory ventilation; PSIMV = pressure-targeted synchronized intermittent mandatory ventilation; PSV = pressure support ventilation; CMV = controlled mandatory ventilation; SIMV = synchronized intermittent mandatory ventilation; NS ICU = neurosurgical intensive care unit; LOS = length of stay.
aCerebral infarction, hydrocephalus meningitis, hypoxic brain damage, infective spondylopathies.
bExtraventricular drainage, craniotomy, burr hole, Guglielmi detachable coils embolization, intracerebral hemorrhage/catheter insert, craniectomy, decompression, ventriculo-other shunt, cerebral aneurysm clipping, operation of arteriovenous malformation, closed thoracostomy, tracheostomy.
cHypertension, diabetes mellitus, chronic renal failure, cancer, and others.
Table 2
Anthropometric, biochemical, and clinical data at intensive care unit baseline and discharge
| Variable | Baseline (3rd day) | Discharge (last day) | P-value |
|---|---|---|---|
| Weight (kg) | 62.3±13.3 | 60.9±12.8 | <0.001* |
| Calf circumference (cm) | 31.4±4.2 | 30.2±4.0 | <0.001* |
| TSF (mm) | 19.3±7.4 | 19.5±7.2 | 0.276 |
| MAMC (cm) | 21.8±3.2 | 20.6±4.0 | <0.001* |
| MAMA (cm2) | 38.8±11.3 | 35.2±11.5 | <0.001* |
| BIA | |||
| Phase angle (°) | 4.0±1.4 | 3.7±1.3 | <0.001* |
| SMI | 5.7±1.1 | 5.3±1.1 | <0.001* |
| ECW/TBW | 0.401±0.015 | 0.405±0.014 | <0.001* |
| TBW/FFM | 74.0±0.54 | 74.0±0.57 | 0.892 |
| Serum albumin (g/dL) | 3.7±0.6 | 3.2±0.5 | <0.001* |
| Nitrogen balance | –8.5±5.2 | –5.8±5.7 | <0.001* |
| UUN (g/day) | 12.0±13.4 | 12.2±18.9 | 0.870 |
| APACHE II score | 22.6±5.1 | 20.8±6.6 | 0.001* |
| SOFA score | 5.8±1.9 | 5.1±3.1 | 0.005* |
| Glasgow Coma Scale | 5.2±3.0 | 6.4±3.9 | 0.001* |
| Braden Scale score | 13.0±3.1 | 13.0±2.6 | 0.816 |
| Pressure ulcer | 6 (4.3) | 33 (23.6) | 0.119 |
| Nutritional assessment | <0.001* | ||
| Adequately nourished status | 96 (68.6) | 63 (45.0) | |
| Mild malnutrition | 40 (28.6) | 69 (49.3) | |
| Moderate malnutrition | 2 (1.4) | 6 (4.3) | |
| Severe malnutrition | 2 (1.4) | 2 (1.4) |
Values are presented as mean±standard deviation or number (%).
TSF = triceps skinfold thickness; MAMC = mid-upper arm muscle circumference; MAMA = mid-upper arm muscle area; BIA = bioelectrical impedance analysis; SMI = skeletal muscle index; ECW = extracellular water; TBW = total body water; FFM = fat-free mass; UUN = 24-hour urine urea nitrogen; APACHE = Acute Physiology and Chronic Health Evaluation; SOFA = Sequential Organ Failure Assessment.
*Values are significantly different between intensive care unit baseline and discharge. P<0.05.
Table 3
Nutritional targets and deficits during neurosurgical intensive care unit hospitalization
Table 4
Nutrition provision comparisons between intensive care unit baseline and discharge
Table 5
Multiple linear regression analysis of cumulative caloric deficit% during neurosurgical intensive care unit hospitalization (aP<0.001)
Table 6
Multiple linear regression analysis of phase angle difference between intensive care unit baseline and discharge (aP=0.038)
Table 7
Multiple linear regression analysis of skeletal muscle index difference between intensive care unit baseline and discharge (aP=0.507)
Table 8
Multiple linear regression analysis of nitrogen balance difference between intensive care unit baseline and discharge (aP=0.236)
- 1. Annette H, Wenström Y. Implementing clinical guidelines for nutrition in a neurosurgical intensive care unit. Nurs Health Sci 2005;7:266-72. ArticlePubMed
- 2. Chapple LA, Chapman MJ, Lange K, Deane AM, Heyland DK. Nutrition support practices in critically ill head-injured patients: a global perspective. Crit Care 2016;20:6.ArticlePubMedPMCPDF
- 3. Mackay LE, Morgan AS, Bernstein BA. Factors affecting oral feeding with severe traumatic brain injury. J Head Trauma Rehabil 1999;14:435-47. ArticlePubMed
- 4. Chapple LS, Deane AM, Heyland DK, Lange K, Kranz AJ, Williams LT, et al. Energy and protein deficits throughout hospitalization in patients admitted with a traumatic brain injury. Clin Nutr 2016;35:1315-22. ArticlePubMed
- 5. Dhandapani SS, Manju D, Sharma BS, Mahapatra AK. Clinical malnutrition in severe traumatic brain injury: factors associated and outcome at 6 months. Indian J Neurotrauma 2007;4:35-9. Article
- 6. Wei X, Day AG, Ouellette-Kuntz H, Heyland DK. The association between nutritional adequacy and long-term outcomes in critically ill patients requiring prolonged mechanical ventilation: a multicenter cohort study. Crit Care Med 2015;43:1569-79. PubMed
- 7. Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. N Engl J Med 2014;370:1626-35. ArticlePubMed
- 8. Abdelmalik PA, Dempsey S, Ziai W. Nutritional and bioenergetic considerations in critically ill patients with acute neurological injury. Neurocrit Care 2017;27:276-86. ArticlePubMedPDF
- 9. Costello LA, Lithander FE, Gruen RL, Williams LT. Nutrition therapy in the optimisation of health outcomes in adult patients with moderate to severe traumatic brain injury: findings from a scoping review. Injury 2014;45:1834-41. ArticlePubMed
- 10. Peterson SJ, Tsai AA, Scala CM, Sowa DC, Sheean PM, Braunschweig CL. Adequacy of oral intake in critically ill patients 1 week after extubation. J Am Diet Assoc 2010;110:427-33. ArticlePubMed
- 11. Pan WH, Yeh WT. How to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: an extension of Asian-Pacific recommendations. Asia Pac J Clin Nutr 2008;17:370-4. PubMed
- 12. de Vries MC, Koekkoek WK, Opdam MH, van Blokland D, van Zanten AR. Nutritional assessment of critically ill patients: validation of the modified NUTRIC score. Eur J Clin Nutr 2018;72:428-35. ArticlePubMedPDF
- 13. de Souza MFC, Zanei SSV, Whitaker IY. Risk of pressure injury in the ICU: transcultural adaptation and reliability of EVARUCI. Acta Paul Enferm 2018;31:201-8. Article
- 14. Swails WS, Samour PQ, Babineau TJ, Bistrian BR. A proposed revision of current ICD-9-CM malnutrition code definitions. J Am Diet Assoc 1996;96:370-3. ArticlePubMed
- 15. Alberda C, Gramlich L, Jones N, Jeejeebhoy K, Day AG, Dhaliwal R, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med 2009;35:1728-37. ArticlePubMedPDF
- 16. Tsai JR, Chang WT, Sheu CC, Wu YJ, Sheu YH, Liu PL, et al. Inadequate energy delivery during early critical illness correlates with increased risk of mortality in patients who survive at least seven days: a retrospective study. Clin Nutr 2011;30:209-14. ArticlePubMed
- 17. Peter JV, Moran JL, Phillips-Hughes J. A metaanalysis of treatment outcomes of early enteral versus early parenteral nutrition in hospitalized patients. Crit Care Med 2005;33:213-20. discussion 260-1. ArticlePubMed
- 18. Hafsteinsdóttir TB, Mosselman M, Schoneveld C, Riedstra YD, Kruitwagen CL. Malnutrition in hospitalised neurological patients approximately doubles in 10 days of hospitalisation. J Clin Nurs 2010;19:639-48. ArticlePubMed
- 19. Deutschman CS, Konstantinides FN, Raup S, Thienprasit P, Cerra FB. Physiological and metabolic response to isolated closed-head injury. Part 1: basal metabolic state: correlations of metabolic and physiological parameters with fasting and stressed controls. J Neurosurg 1986;64:89-98. PubMed
- 20. Hoffer LJ. Protein and energy provision in critical illness. Am J Clin Nutr 2003;78:906-11. ArticlePubMed
- 21. Kreymann G, DeLegge MH, Luft G, Hise ME, Zaloga GP. The ratio of energy expenditure to nitrogen loss in diverse patient groups--a systematic review. Clin Nutr 2012;31:168-75. ArticlePubMed
- 22. Wirth R, Volkert D, Rösler A, Sieber CC, Bauer JM. Bioelectric impedance phase angle is associated with hospital mortality of geriatric patients. Arch Gerontol Geriatr 2010;51:290-4. ArticlePubMed
- 23. Thibault R, Makhlouf AM, Mulliez A, Cristina Gonzalez M, Kekstas G, Kozjek NR, et al. Phase Angle Project Investigators. Fat-free mass at admission predicts 28-day mortality in intensive care unit patients: the international prospective observational study Phase Angle Project. Intensive Care Med 2016;42:1445-53. ArticlePubMedPDF
- 24. Berger MM, Reintam-Blaser A, Calder PC, Casaer M, Hiesmayr MJ, Mayer K, et al. Monitoring nutrition in the ICU. Clin Nutr 2019;38:584-93. ArticlePubMed
- 25. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M. ESPEN guidelines for nutrition screening 2002. Clin Nutr 2003;22:415-21. ArticlePubMed
- 26. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z. Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr 2003;22:321-36. ArticlePubMed
- 27. Simpson F, Doig GS. Early PN Trial Investigators Group. Physical assessment and anthropometric measures for use in clinical research conducted in critically ill patient populations: an analytic observational study. JPEN J Parenter Enteral Nutr 2015;39:313-21. PubMed
- 28. Sheean PM, Peterson SJ, Gurka DP, Braunschweig CA. Nutrition assessment: the reproducibility of subjective global assessment in patients requiring mechanical ventilation. Eur J Clin Nutr 2010;64:1358-64. ArticlePubMedPMCPDF
- 29. Miyajima I, Yatabe T, Kuroiwa H, Tamura T, Yokoyama M. Influence of nutrition support therapy on readmission among patients with acute heart failure in the intensive care unit: a single-center observational study. Clin Nutr 2020;39:174-9. ArticlePubMed
- 30. Sungurtekin H, Sungurtekin U, Oner O, Okke D. Nutrition assessment in critically ill patients. Nutr Clin Pract 2008;23:635-41. ArticlePubMedPDF
- 31. Kim D, Sun JS, Lee YH, Lee JH, Hong J, Lee JM. Comparative assessment of skeletal muscle mass using computerized tomography and bioelectrical impedance analysis in critically ill patients. Clin Nutr 2019;38:2747-55. ArticlePubMed
- 32. Rogenski NM, Santos VL. [Incidence of pressure ulcers at a university hospital]. Rev Lat Am Enfermagem 2005;13:474-80; Portuguese. PubMed
- 33. Blanes L, Duarte IS, Calil JA, Ferriera LM. Clinical and epidemiological assessment of pressure ulcers in patients admitted to Sao Paulo Hospital. Rev Assoc Méd Bras 2004;50:182-7. PubMed
- 34. Hyun S, Li X, Vermillion B, Newton C, Fall M, Kaewprag P, et al. Body mass index and pressure ulcers: improved predictability of pressure ulcers in intensive care patients. Am J Crit Care 2014;23:494-500. quiz 501.ArticlePubMedPMC
- 35. Becker D, Tozo TC, Batista SS, Mattos AL, Silva MCB, Rigon S, et al. Pressure ulcers in ICU patients: incidence and clinical and epidemiological features: a multicenter study in southern Brazil. Intensive Crit Care Nurs 2017;42:55-61. ArticlePubMed
- 36. Kaya H, Turan N, Özdemir Aydın G. Stan odżywienia pacjentów neurochirurgicznego oddziału intensywnej opieki medycznej. J Neurol Neurosurg Nurs 2017;6:33-8; Polish. ArticlePDF
- 37. Heyland DK, Dhaliwal R, Jiang X, Day AG. Identifying critically ill patients who benefit the most from nutrition therapy: the development and initial validation of a novel risk assessment tool. Crit Care 2011;15:R268.ArticlePubMedPMCPDF
- 38. Mukhopadhyay A, Henry J, Ong V, Leong CS, Teh AL, van Dam RM, et al. Association of modified NUTRIC score with 28-day mortality in critically ill patients. Clin Nutr 2017;36:1143-8. ArticlePubMed
- 39. Ardehali SH, Dehghan S, Baghestani AR, Velayati A, Vahdat Shariatpanahi Z. Association of admission serum levels of vitamin D, calcium, Phosphate, magnesium and parathormone with clinical outcomes in neurosurgical ICU patients. Sci Rep 2018;8:2965.ArticlePubMedPMCPDF
- 40. Dionyssiotis Y, Papachristos A, Petropoulou K, Papathanasiou J, Papagelopoulos P. Nutritional alterations associated with neurological and neurosurgical diseases. Open Neurol J 2016;10:32-41. ArticlePubMedPMCPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Association between the Modified NUTRIC Score (mNUTRIC) and Clinical Outcomes in a Mixed Intensive Care Unit: A Retrospective Cohort Study
Thanh Luan Nguyen, Quang Dai Le, Trang Nguyen Hoai Dinh, Van Hoang Nam Ho, Cong Dang Tran, Van Phieu Duong, Hoang Ngoc Thao Duong, Phuc Tuong Pham, Thi Phuong Thao Le, Tuyet Phuong Bui
SN Comprehensive Clinical Medicine.2026;[Epub] CrossRef - Barriers to nutrition following neurosurgery: A descriptive cohort study
Dale Palmer, Melissa Zhou, Suzie Ferrie
Journal of Parenteral and Enteral Nutrition.2026; 50(4): 565. CrossRef - A Review on the Effects of Multiple Nutritional Scores on Wound Healing after Neurosurgery.
Jingqian Ye, Bo Ning , Jianwen Zhi
International Journal of Biology and Life Sciences.2025; 9(2): 82. CrossRef - Transition from Enteral to Oral Nutrition in Intensive Care and Post Intensive Care Patients: A Scoping Review
Gioia Vinci, Nataliia Yakovenko, Elisabeth De Waele, Reto Stocker
Nutrients.2025; 17(11): 1780. CrossRef
 Cite
Cite- Figure
-
Comparative assessment of nutritional characteristics of critically ill patients at admission and discharge from the neurosurgical intensive care unit in Korea: a comparison study
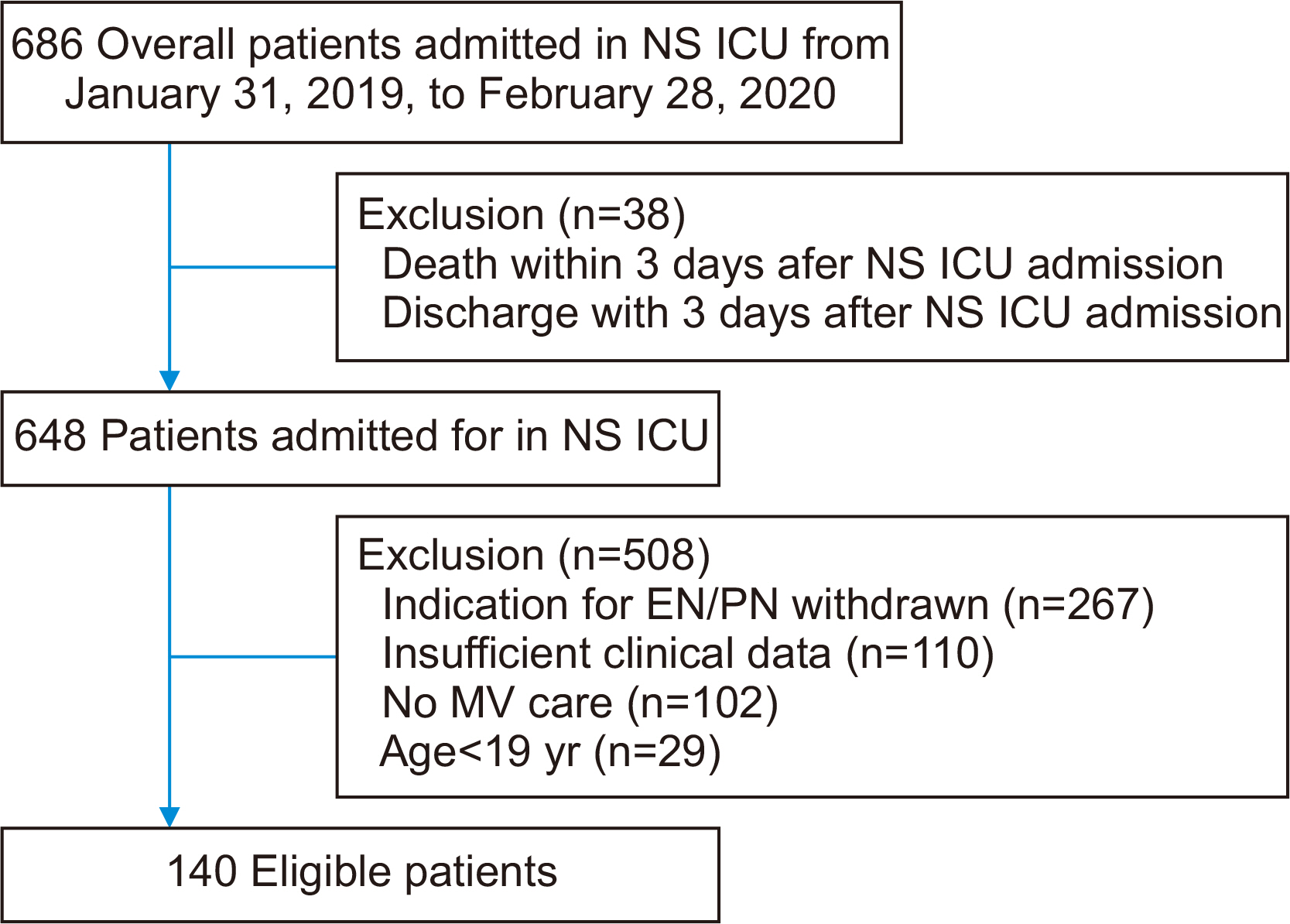
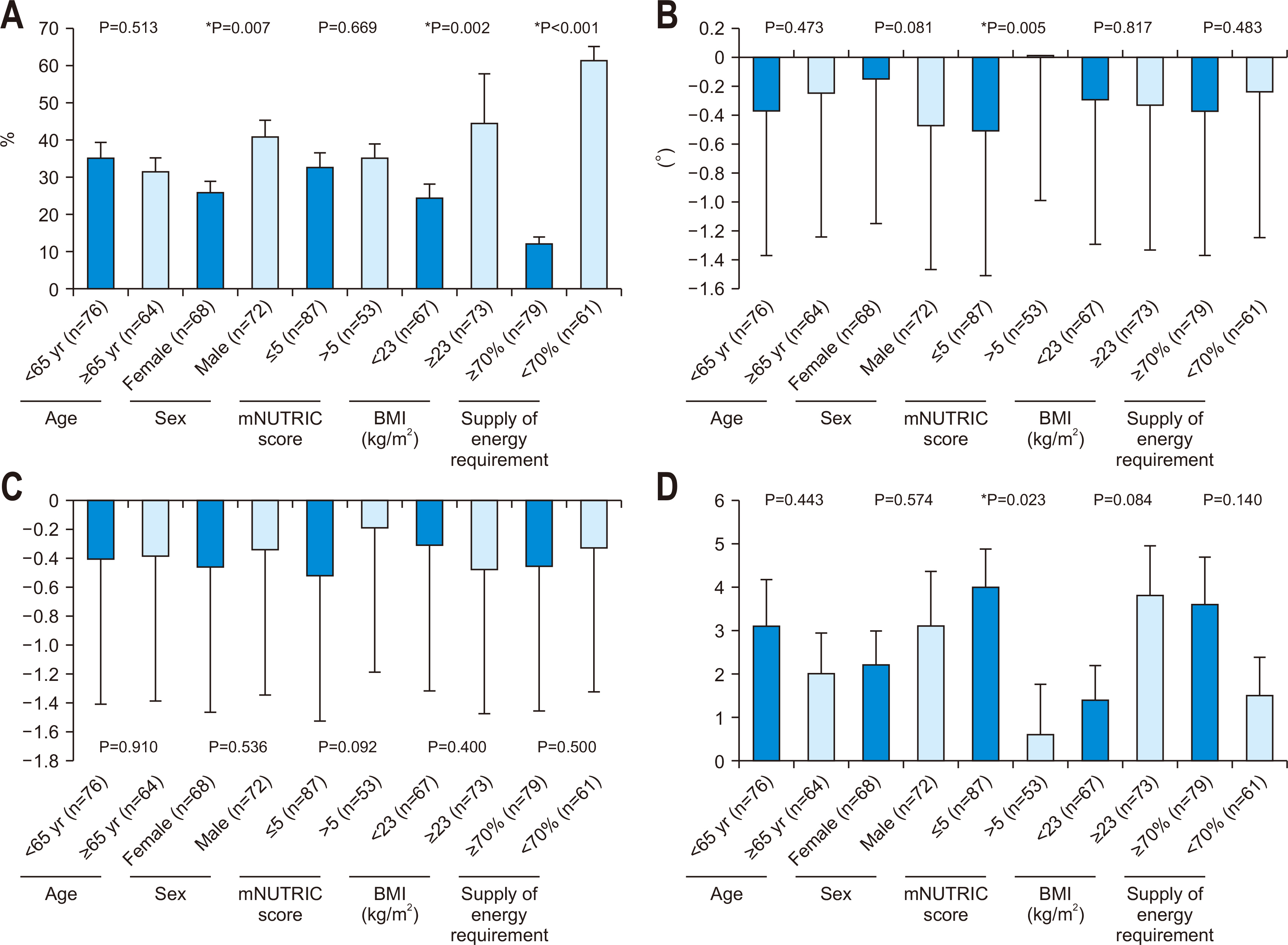
Fig. 1
Flow diagram of patients selected for analysis. NS ICU = neurosurgical intensive care unit; EN = enteral nutrition; PN = parenteral nutrition; MV = mechanical ventilator.
Fig. 2
Cumulative caloric deficit, phase angle, skeletal muscle mass index, and nitrogen balance by clinical characteristics. Data shown are the mean cumulative caloric deficit, phase angle, skeletal muscle index, and nitrogen balance. Error bars are standard errors. (A) Cumulative caloric deficit% during the intensive care unit (ICU) period. (B) Change in phase angle between ICU baseline and discharge. (C) Change in skeletal muscle index between ICU baseline and ICU discharge. (D) Change in nitrogen balance between ICU baseline and discharge. mNUTRIC = modified Nutrition Risk in the Critically ill; BMI = body mass index.
Fig. 1
Fig. 2
Comparative assessment of nutritional characteristics of critically ill patients at admission and discharge from the neurosurgical intensive care unit in Korea: a comparison study
Baseline demographic and clinical characteristics
| Variable | All patients (n=140) |
|---|---|
| Age (yr) | 61.9±15.3 |
| Sex, male | 72 (51.4) |
| Height (cm) | 162.9±0.8 |
| mNUTRIC score | 5.1±1.4 |
| SAPS III score | 33.6±13.0 |
| Mechanical ventilator (day) | 9.5 (4.0–18.0) |
| Mechanical ventilator mode | |
| PCV | 80 (57.1) |
| PSIMV | 42 (30.0) |
| PSV | 13 (9.3) |
| CMV | 4 (2.9) |
| SIMV | 1 (0.7) |
| Primary diagnosis | |
| Brain hemorrhage | 101 (72.1) |
| Brain tumor | 25 (17.9) |
| Other |
14 (10.0) |
| NS ICU LOS (day) | 21.0 (11.2–33.7) |
| Hospital LOS (day) | 39.5 (25.0–63.0) |
| NS ICU-free (day) | 14.0 (0.0–33.5) |
| Reason for NS ICU discharge | |
| Inter-hospital transfer | 90 (64.3) |
| Permanent care facility | 23 (16.4) |
| Death | 27 (19.3) |
| Surgery |
129 (92.1) |
| Comorbidities |
106 (75.7) |
Values are presented as mean±standard deviation, number (%), or median (25th–75th percentiles).
mNUTRIC = modified Nutrition Risk in the Critically ill; SAPS = Simplified Acute Physiology Score; PCV = pressure-targeted controlled mandatory ventilation; PSIMV = pressure-targeted synchronized intermittent mandatory ventilation; PSV = pressure support ventilation; CMV = controlled mandatory ventilation; SIMV = synchronized intermittent mandatory ventilation; NS ICU = neurosurgical intensive care unit; LOS = length of stay.
aCerebral infarction, hydrocephalus meningitis, hypoxic brain damage, infective spondylopathies.
bExtraventricular drainage, craniotomy, burr hole, Guglielmi detachable coils embolization, intracerebral hemorrhage/catheter insert, craniectomy, decompression, ventriculo-other shunt, cerebral aneurysm clipping, operation of arteriovenous malformation, closed thoracostomy, tracheostomy.
cHypertension, diabetes mellitus, chronic renal failure, cancer, and others.
Anthropometric, biochemical, and clinical data at intensive care unit baseline and discharge
| Variable | Baseline (3rd day) | Discharge (last day) | P-value |
|---|---|---|---|
| Weight (kg) | 62.3±13.3 | 60.9±12.8 | <0.001 |
| Calf circumference (cm) | 31.4±4.2 | 30.2±4.0 | <0.001 |
| TSF (mm) | 19.3±7.4 | 19.5±7.2 | 0.276 |
| MAMC (cm) | 21.8±3.2 | 20.6±4.0 | <0.001 |
| MAMA (cm2) | 38.8±11.3 | 35.2±11.5 | <0.001 |
| BIA | |||
| Phase angle (°) | 4.0±1.4 | 3.7±1.3 | <0.001 |
| SMI | 5.7±1.1 | 5.3±1.1 | <0.001 |
| ECW/TBW | 0.401±0.015 | 0.405±0.014 | <0.001 |
| TBW/FFM | 74.0±0.54 | 74.0±0.57 | 0.892 |
| Serum albumin (g/dL) | 3.7±0.6 | 3.2±0.5 | <0.001 |
| Nitrogen balance | –8.5±5.2 | –5.8±5.7 | <0.001 |
| UUN (g/day) | 12.0±13.4 | 12.2±18.9 | 0.870 |
| APACHE II score | 22.6±5.1 | 20.8±6.6 | 0.001 |
| SOFA score | 5.8±1.9 | 5.1±3.1 | 0.005 |
| Glasgow Coma Scale | 5.2±3.0 | 6.4±3.9 | 0.001 |
| Braden Scale score | 13.0±3.1 | 13.0±2.6 | 0.816 |
| Pressure ulcer | 6 (4.3) | 33 (23.6) | 0.119 |
| Nutritional assessment | <0.001 |
||
| Adequately nourished status | 96 (68.6) | 63 (45.0) | |
| Mild malnutrition | 40 (28.6) | 69 (49.3) | |
| Moderate malnutrition | 2 (1.4) | 6 (4.3) | |
| Severe malnutrition | 2 (1.4) | 2 (1.4) |
Values are presented as mean±standard deviation or number (%).
TSF = triceps skinfold thickness; MAMC = mid-upper arm muscle circumference; MAMA = mid-upper arm muscle area; BIA = bioelectrical impedance analysis; SMI = skeletal muscle index; ECW = extracellular water; TBW = total body water; FFM = fat-free mass; UUN = 24-hour urine urea nitrogen; APACHE = Acute Physiology and Chronic Health Evaluation; SOFA = Sequential Organ Failure Assessment.
*Values are significantly different between intensive care unit baseline and discharge. P<0.05.
Nutritional targets and deficits during neurosurgical intensive care unit hospitalization
| Variable | All patients (n=140) |
|---|---|
| Days from NS ICU admission to initiating nutrition support | 1.75±1.0 |
| Patients who started EN within 48 hours from NS ICU admission | 61 (43.6) |
| Days receiving EN | 20.2±17.2 |
| Targets | |
| Calories prescribed (kcal/day) | 1,600 (1,300–1,700) |
| Calories prescribed (kcal/kg) | 24.6 (24.1–25.7) |
| Total energy requirements during NS ICU period (kcal) | 31,500 (15,400–54,150) |
| Proteins prescribed (g/day) | 80 (70–90) |
| Proteins prescribed (g/kg) | 1.26 (1.23–1.30) |
| Total protein requirements during NS ICU period (g) | 1,617 (785–2,730) |
| Deficits | |
| Cumulative caloric deficit (kcal) | 8,571 (3,232–14,362) |
| % Cumulative caloric deficit | 27.9 (13.3–48.0) |
| Cumulative protein deficit (g) | 516.9 (210.3–840.6) |
| % Cumulative protein deficit | 33.2 (16.0–51.8) |
Values are presented as mean±standard deviation, number (%), or median (25th–75th percentiles).
NS ICU = neurosurgical intensive care unit; EN = enteral nutrition.
Nutrition provision comparisons between intensive care unit baseline and discharge
| Variable | Baseline (3rd day) | Discharge (last day) |
|---|---|---|
| Calorie intake | ||
| Calories received (kcal/day) | 659.0 (421–861) | 1,354.6 (1,119–1,546) |
| Calories received (kcal/kg) | 10.1 (7.1–14.1) | 23.5 (18.2–25.9) |
| % Calories received of prescribed | 42.0 (28.4–57.1) | 95.3 (74.0–106.6) |
| % Enteral nutrition of calories prescribed | 0 (0–37.5) | 92.8 (69.4–100) |
| % Parenteral nutrition of calories prescribed | 22.0 (9.5–35.5) | 0 (0–0.5) |
| Daily caloric deficit (kcal/day) | 840.3 (608.7–1,183.1) | 77.0 (–100.0 to 400.0) |
| Protein intake | ||
| Protein received (g/day) | 35.1 (23.5–46.5) | 60.9 (50.0–72.0) |
| Protein received (g/kg) | 0.5 (0.3–0.7) | 1.0 (0.8–1.2) |
| % Protein received of prescribed | 45.7 (29.4–59.6) | 83.0 (68.0–101.6) |
| % Enteral nutrition of protein prescribed | 0 (0–34.1) | 80.0 (60.0–96.2) |
| % Parenteral nutrition of protein prescribed | 29.4 (15.7–45.7) | 0 (0–0) |
| Daily protein deficit (g/day) | 42.7 (29.0–58.9) | 12.0 (–1.0 to 26.0) |
Values are presented as median (25th–75th percentiles).
P-values of all data by paired t-test were <0.001.
Multiple linear regression analysis of cumulative caloric deficit% during neurosurgical intensive care unit hospitalization (
| Independent variable | β (standardized) | SE | t-value | P-value |
|---|---|---|---|---|
| Constant | 50.736 | 5.035 | 10.078 | <0.001 |
| Age≥65 yr | 7.509 (0.111) | 4.260 | 1.763 | 0.080 |
| Sex, male | 6.004 (0.089) | 3.966 | 1.514 | 0.132 |
| mNUTRIC>5 | –6.748 (–0.097) | 4.256 | –1.585 | 0.115 |
| Body mass index≥23 kg/m2 | 11.961 (0.177) | 3.890 | 3.075 | 0.003 |
| Supply of energy requirement≥70% | –48.601 (–0.715) | 3.990 | –12.180 | <0.001 |
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill.
aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Multiple linear regression analysis of phase angle difference between intensive care unit baseline and discharge (
| Independent variable | β (standardized) | SE | t-value | P-value |
|---|---|---|---|---|
| Constant | –0.210 | 0.236 | –0.890 | 0.375 |
| Age≥65 yr | –0.134 (–0.062) | 0.200 | –0.672 | 0.503 |
| Sex, male | –0.364 (–0.169) | 0.186 | –1.953 | 0.053 |
| mNUTRIC>5 | 0.552 (0.249) | 0.200 | 2.761 | 0.007 |
| Body mass index≥23 kg/m2 | –0.008 (–0.003) | 0.183 | –0.041 | 0.967 |
| Supply of energy requirement≥70% | –0.107 (–0.049) | 0.187 | –0.571 | 0.569 |
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill.
aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Multiple linear regression analysis of skeletal muscle index difference between intensive care unit baseline and discharge (
| Independent variable | β (standardized) | SE | t-value | P-value |
|---|---|---|---|---|
| Constant | –0.407 | 0.259 | –1.574 | 0.118 |
| Age≥65 yr | –0.099 (–0.043) | 0.219 | –0.451 | 0.653 |
| Sex, male | 0.111 (0.049) | 0.204 | 0.546 | 0.586 |
| mNUTRIC>5 | 0.353 (0.150) | 0.219 | 1.615 | 0.109 |
| Body mass index≥23 kg/m2 | –0.189 (–0.082) | 0.200 | –0.945 | 0.347 |
| Supply of energy requirement≥70% | –0.073 (–0.032) | 0.205 | –0.356 | 0.723 |
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill.
aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Multiple linear regression analysis of nitrogen balance difference between intensive care unit baseline and discharge (
| Independent variable | β (standardized) | SE | t-value | P-value |
|---|---|---|---|---|
| Constant | 2.276 | 1.518 | 1.500 | 0.136 |
| Age≥65 yr | 0.542 (0.040) | 1.284 | 0.422 | 0.674 |
| Sex, male | 0.644 (0.047) | 1.196 | 0.539 | 0.591 |
| mNUTRIC>5 | –2.552 (–0.183) | 1.283 | –1.989 | 0.049 |
| Body mass index≥23 kg/m2 | 1.689 (0.124) | 1.172 | 1.440 | 0.152 |
| Supply of energy requirement≥70% | –0.324 (–0.024) | 1.203 | –0.269 | 0.788 |
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill.
aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Table 1
Baseline demographic and clinical characteristics
Values are presented as mean±standard deviation, number (%), or median (25th–75th percentiles). mNUTRIC = modified Nutrition Risk in the Critically ill; SAPS = Simplified Acute Physiology Score; PCV = pressure-targeted controlled mandatory ventilation; PSIMV = pressure-targeted synchronized intermittent mandatory ventilation; PSV = pressure support ventilation; CMV = controlled mandatory ventilation; SIMV = synchronized intermittent mandatory ventilation; NS ICU = neurosurgical intensive care unit; LOS = length of stay. aCerebral infarction, hydrocephalus meningitis, hypoxic brain damage, infective spondylopathies. bExtraventricular drainage, craniotomy, burr hole, Guglielmi detachable coils embolization, intracerebral hemorrhage/catheter insert, craniectomy, decompression, ventriculo-other shunt, cerebral aneurysm clipping, operation of arteriovenous malformation, closed thoracostomy, tracheostomy. cHypertension, diabetes mellitus, chronic renal failure, cancer, and others.
Table 2
Anthropometric, biochemical, and clinical data at intensive care unit baseline and discharge
Values are presented as mean±standard deviation or number (%). TSF = triceps skinfold thickness; MAMC = mid-upper arm muscle circumference; MAMA = mid-upper arm muscle area; BIA = bioelectrical impedance analysis; SMI = skeletal muscle index; ECW = extracellular water; TBW = total body water; FFM = fat-free mass; UUN = 24-hour urine urea nitrogen; APACHE = Acute Physiology and Chronic Health Evaluation; SOFA = Sequential Organ Failure Assessment. *Values are significantly different between intensive care unit baseline and discharge. P<0.05.
Table 3
Nutritional targets and deficits during neurosurgical intensive care unit hospitalization
Values are presented as mean±standard deviation, number (%), or median (25th–75th percentiles). NS ICU = neurosurgical intensive care unit; EN = enteral nutrition.
Table 4
Nutrition provision comparisons between intensive care unit baseline and discharge
Values are presented as median (25th–75th percentiles). P-values of all data by paired t-test were <0.001.
Table 5
Multiple linear regression analysis of cumulative caloric deficit% during neurosurgical intensive care unit hospitalization (aP<0.001)
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill. aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Table 6
Multiple linear regression analysis of phase angle difference between intensive care unit baseline and discharge (aP=0.038)
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill. aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Table 7
Multiple linear regression analysis of skeletal muscle index difference between intensive care unit baseline and discharge (aP=0.507)
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill. aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.
Table 8
Multiple linear regression analysis of nitrogen balance difference between intensive care unit baseline and discharge (aP=0.236)
SE = standard error; mNUTRIC = modified Nutrition Risk in the Critically ill. aThe suitability of the regression model for the 5 independent variables was confirmed through the P-value of the ANOVA result table.

