 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 16(2); 2024 > Article
- Original Article Early nutritional support for inpatients reduces admission rates to intensive care units in Korea: a single-center case-control study
-
Hyun Suk Kim1
 , Jae Do Yang1,2, Se Wung Han1,2, Mi Rin Lee1,2, Da-Sol Kim1,3, Sejin Lee1,2, Seon-Hyeong Kim1, Chan-Young Kim1,2
, Jae Do Yang1,2, Se Wung Han1,2, Mi Rin Lee1,2, Da-Sol Kim1,3, Sejin Lee1,2, Seon-Hyeong Kim1, Chan-Young Kim1,2 -
Annals of Clinical Nutrition and Metabolism 2024;16(2):57-65.
DOI: https://doi.org/10.15747/ACNM.2024.16.2.57
Published online: August 1, 2024
1Nutrition Support Team, Jeonbuk National University Hospital, Jeonju, Korea
2Department of Surgery, Jeonbuk National University Hospital, Jeonju, Korea
3Department of Physical Medicine and Rehabilitation, Jeonbuk National University Hospital, Jeonju, Korea
- Corresponding author: Chan-Young Kim, email: happyhill@jbuh.co.kr
• Received: March 20, 2024 • Revised: May 4, 2024 • Accepted: May 20, 2024
© 2024 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,429 Views
- 28 Download
Abstract
-
Purpose Early nutritional support (ENS) for critically ill patients is promoted by many studies. However, there is a lack of data evaluating its necessity in general wards. This study aims to determine the impact of ENS on patients in general wards.
-
Methods Patients aged 18 and above, admitted to the Jeonbuk National University Hospital in Jeonju from January 2020 to December 2020, who were eligible for nutritional support and hospitalized for at least 7 days were included in the study. We divided the patients into two groups the ENS group, who received nutritional support within 48 hours of admission, and the control group, who received it after 48 hours.
-
Results Among 1,077 patients, 146 met the inclusion criteria. The ENS group (n=38) and the control group (n=108) were compared retrospectively. There was a significant age difference between the two groups (P=0.028). The admission ratio to the intensive care unit (ICU) in the ENS group was significantly lower than that in the control group (10.2% vs. 26.3%, P=0.019). The calorie support rate (%) and protein support rate (%) in the ENS group were significantly higher than in the control group (50.12%±23.30% vs. 38.56%±18.02%, P=0.006; 44.61%±25.07% vs. 32.07%±22.76%, P=0.002, respectively). After propensity score matching, the ENS was significantly associated with ICU low admissions (odds ratio 0.08, 95% confidence interval 0.01–0.69, P=0.022).
-
Conclusion A future multi-center study considering underlying diseases is needed to provide additional scientific evidence to support the effects of ENS.
Graphical abstract
Introduction
Monitoring the nutritional status of hospitalized patients and the implementation of appropriate dietary support are crucial for disease improvement. Malnutrition occurs when oral intake is persistently inadequate, leading to changes in physical function, weight, and body composition, and a failure to meet nutritional requirements [1]. Malnutrition is associated with complication rates in hospitalized patients, length of hospital stay, mortality, and healthcare costs [2,3]. In Western countries, the prevalence of malnutrition in hospitals has been estimated to be 30%–50% [4]. Additionally, it has been reported in 30%–55% of hospitalized patients in Korea [5], and there is a concern that this condition may worsen during hospitalization [6].
Recently, the focus of nutritional support has shifted toward objectives such as preventing oxidative damage to cells, reducing metabolic overreactions, and enhancing immune responses, as part of nutritional therapy [7]. Multiple studies have reported the necessity of early nutritional support (ENS), which involves providing enteral or intravenous nutrition to patients unable to achieve adequate oral intake within 48 hours of hospitalization [3,7-11]. However, most studies and guidelines related to ENS focus on critically ill patients, overlooking the significance of ENS for patients in general wards. Inpatients, not only those in the intensive care unit (ICU), face challenges in achieving adequate nutritional intake due to several factors, including disease-related appetite loss, medication-related side effects, nil per os (NPO) prescriptions for diagnostic tests, and gastrointestinal disorders arising from disease [12]. Böhne et al. (2022) [2] reported that patients admitted to medical facilities, including hospitals, ICUs, and nursing homes, exhibited low oral intake even after admission. Particularly noteworthy was the observation that while oral intake was not compromised before admission, a notable 27% reduction occurred following admission. In connection with this, the omission or delay in nutritional support for general ward patients may result in supplying inadequate nutrition, thereby exacerbating the progression of malnutrition during hospitalization. Additionally, malnutrition could accelerate infection rates and immune function impairment, potentially increasing the length of hospital stay, mortality rates, and healthcare costs [7].
A recent trend in the increasing severity among patients is related to the aging of the population, the rising incidence of chronic disease, and the complexity of the disease. However, due to limitations in the availability of ICU beds, most patients are admitted to general wards for treatment [13,14]. Hence, by preventing unnecessary transfers from general wards to the ICU, those critically ill patients who absolutely require ICU care have the opportunity to receive it. Moreover, ICU admission influences unnecessary healthcare expenditures, increases the total length of hospital stay, and jeopardizes patient safety [15]. In a study by Lee and Choi (2014) [13], the Sequential Organ Failure Assessment (SOFA) score, representing nutritional status, emerged as a risk factor for ICU admission among general ward patients [16-18].
We aim to investigate whether ENS affects the ICU admission rate of general ward patients.
Methods
This was a single-center retrospective study approved by the Institutional Review Board (IRB) of Jeonbuk National University Hospital (CUH 2023-12-044). Informed consent from the subjects was exempted due to the retrospective nature of the study. All procedures adhered to institutional and national ethical standards, as established by the committee overseeing human experimentation, and complied with the principles of the Helsinki Declaration of 2013.
It is a single institute case-control study. It was described according to the STOBE statement, which is available at: https://www.strobe-statement.org/
The study included 1,077 patients who were receiving prescriptions related to enteral nutrition or parenteral nutrition and were admitted to Jeonbuk National University Hospital in Jeonju, Jeollabuk-do, Korea, from January 2020 to December 2020, with hospital stays lasting more than 7 days. Exclusion criteria were as follows: patients with hospital stays of less than 7 days or exceeding one year, patients not receiving enteral or parenteral nutrition during hospitalization, those admitted to the ICU, duplicate patients, and those without accessible electronic medical records (EMRs). The final analysis involved 146 patients. In cases of repeated admissions by the same patient, only the first occurrence was considered. The ENS group included 38 patients who received enteral or parenteral nutrition during the first 48 hours after admission as followed in international guidelines [10]. The control group comprised 108 patients who received enteral or parenteral nutrition 48 hours after admission.
The primary outcome of this study is admission to the ICU, and the secondary outcomes are the amount of calories and protein supplied, length of hospital stay, and in-hospital mortality.
The characteristics of the subjects were collected via EMRs. The data, including age, sex, height, weight, admission type, smoking and alcohol consumption, and nutritional status, were collected at admission. The body mass index (BMI), calculated as weight (kg)/height (m2), ideal body weight, calculated as height (m)×height (m)×22 (male) or 21 (female), and the percentage of ideal body weight (PIBW), calculated as current body weight/ideal body weight×100, were determined using height (cm) and weight (kg). The obesity classification followed the criteria of the Korean Society for the Study of Obesity, categorizing BMI below 18.5 kg/m2 as underweight, 18.5 to 22.9 kg/m2 as normal, 23.0 to 24.9 kg/m2 as overweight, and 25.0 kg/m2 or above as obese. Nutritional status at admission was based on the Global Leadership Initiative on Malnutrition criteria [19]. Consultations for nutritional support, as well as the types of nutritional support, were confirmed through prescription during the hospitalization period. The length of NPO, the length of hospital stay, and mortality during the hospitalization period were collected via EMRs.
We calculated daily calorie requirements, applying a minimum value of 25 kcal/kg/d. Protein requirements were calculated by referencing the protein needs per weight based on the stress status of the patient. Protein requirements were calculated in the range of 1.0 to 1.5 g/kg/d, with restrictions to 0.8 g/kg/d based on renal and hepatic failure. In stress status, protein requirements were calculated as 1.2 to 1.5 g/kg for postoperative patients and 1.5 to 2.5 g/kg for patients undergoing continuous renal replacement therapy. Caloric delivery rate (%) was calculated as the supplied calories divided by the calorie requirements, multiplied by 100, whereas the protein delivery rate (%) was calculated as the supplied protein divided by the protein requirements, multiplied by 100.
Biochemical markers analyzed in this study included albumin, total lymphocyte count (TLC), hemoglobin, hematocrit, glucose, blood urea nitrogen (BUN), creatinine, alanine transaminase (ALT), aspartate transaminase (AST), sodium, potassium, chloride, calcium, phosphorus, and C-reactive protein (CRP) and these data were collected via EMRs.
There was no selection bias reportable.
Sample size estimation was not conducted because it is a retrospective study. All participants were selected based on the inclusion and exclusion criteria.
All the data collected were analyzed using IBM SPSS Statistics version 23.0 (IBM Corp.), R software (version 4.3.2., GUI 1.80 for Statistical Computing), and the R Studio interface (version 2023.09.1). Categorical variables such as sex, admission type, nutrition consultation, and ICU admission were presented as frequencies and percentages. Continuous variables such as height, weight, and BMI were expressed as means and standard deviations. For the analysis of continuous variables, either the Student’s t-test or the Mann–Whitney test was applied. The paired t-test or Wilcoxon signed-rank test was used for comparing variables at admission and discharge within each group. Categorical variables were analyzed using Pearson’s chi-square test.
To eliminate selection and confounding bias, propensity score matching (PSM) was conducted [20,21]. Covariates with P<0.1 were chosen to adjust for significant differences [22], so confounding factors included in the propensity score were age, height, admission type, nutrition support access, and nutritional status. Additionally, a univariable logistic model was used to confirm the effect of the following factors: age, height, admission type, nutrition support access, and nutritional status on ICU admission. PSM was executed using a 1:1 nearest neighbor approach with a caliper width of 0.2. Matching was conducted within the caliper values. To validate the covariate balance between the two groups, standardized differences were computed pre- and post-PSM. A balanced covariate was defined as having a standard deviation of less than 10% [20,23]. Crude odds ratios (ORs) and adjusted ORs with a 95% confidence interval (CI) were calculated. A P-value less than 0.05 was considered statistically significant.
After performing PSM, subgroup analysis was conducted for internal medicine as the surgical type was omitted in the admission type. For subgroup analysis, variables such as length of hospital stay, NPO period, ICU admission, laboratory data, calorie supply, and protein supply were analyzed, and the analysis method remains the same as above.
Results
A total of 146 subjects were included in this study (Fig. 1). The demographic characteristics of the subjects are shown in Table 1. There were no significant differences in sex between the ENS group and the control group, but age was significantly lower in the ENS group (77.56±9.79 years vs. 81.66±9.34 years, P=0.028). The admission type in the ENS group consisted of 83.3% medical type and 16.7% surgical type, whereas it was 100% medical type in the control group, indicating a significant difference between the two groups (P=0.007). Moreover, the distribution of medical departments was significantly different between the two groups (P<0.001; Supplement Table 1). Anthropometric data including height, weight, BMI, BMI range and percentage ideal body weight, smoking status, and drinking status were not significantly different between the ENS and control groups. There was a significant difference in access to nutritional support between the two groups (P=0.045). The distribution of enteral and parenteral nutrition combined was the highest in the ENS group at 58.3%, while the distribution of enteral nutrition alone was the highest in the control group at 47.4%. Nutritional status did not show a significant difference between the two groups. However, severe malnutrition was most prevalent in the ENS group at 41.7%, whereas moderate malnutrition was most prevalent in the control group at 50.0%.
The length of NPO and length of hospital stay for the subjects were significantly shorter in the ENS group compared to the control group (P<0.001 and P=0.016, respectively). Additionally, there was a significant difference in the proportion of ICU admissions during hospitalization, with 10.2% in the ENS group and 26.3% in the control group (P=0.019). Furthermore, in-hospital mortality showed a significant difference, with 9.3% in the ENS group and 23.7% in the control group (P=0.029; Table 2).
The results of the target and amount of calorie and protein supply for the subjects are shown in Table 3. The proportion of average daily calorie supply relative to the target calories was significantly higher in the ENS group compared to the control group (50.12%±23.30% vs. 38.56%±18.02%, P=0.006). Similarly, the proportion of average daily protein supply showed a significant difference between the ENS and control groups (44.61%±25.07% vs. 32.07%±22.76%, P=0.002). The proportion of calories received through enteral nutrition was significantly higher in the ENS group compared to the control group (31.46%±22.96% vs. 18.76%±15.44%, P=0.004; Supplement Table 2). However, there was no significant difference in the proportion of protein supply through enteral nutrition (Supplement Table 2). Additionally, there were no significant differences between the two groups in the proportion of calories and protein received through parenteral nutrition (Supplement Table 2).
The serum albumin levels showed no significant differences from admission to discharge in both the ENS and control groups. However, in both groups, the levels of TLC significantly increased at discharge compared to admission (both, P<0.001), with no significant differences between the two groups at admission and discharge. At discharge, serum hemoglobin and hematocrit levels were significantly higher in the ENS group compared to the control group (P=0.015 and P=0.008, respectively). However, hemoglobin levels significantly decreased at discarge compared with levels as admission in both groups (ENS, P<0.001; control, P=0.002, respectively). The levels of serum calcium showed no significant differences between the two groups at admission but were significantly higher in the ENS group compared to the control group at discharge (P=0.027). In both groups, serum CRP levels significantly decreased at discharge compared to levels at admission (both, P<0.001). Additionally, the level of CRP was significantly lower in the ENS group compared to the control group at discharge (P=0.013; Table 4).
Details on the factors influencing ICU admission are shown in Table 5, Supplement Tables 3, 4. Before PSM, ENS and admission type were significantly associated with ICU admission (OR 0.32, 95% CI 0.21–0.82, P=0.018; OR 5.18, 95% CI 1.73–15.54, P=0.003, respectively). Moreover, ENS significantly influenced ICU admission after adjusting for age, admission type, and nutrition support access (aOR 0.14, 95% CI 0.04–0.53, P=0.004). Furthermore, ENS was significantly associated with ICU admission after PSM (OR 0.08, 95% CI 0.01–0.69, P=0.022).
Discussion
This study was conducted to determine whether ENS impacted the ICU admission of general ward patients. The rates of energy and protein supply in the ENS group were significantly higher than those in the control group. Furthermore, providing ENS to patients in the general wards can prevent ICU admissions.
Patients with poor oral intake or undergoing NPO often find it challenging to meet nutritional requirements through diet alone. Therefore, it is advisable to provide supplemental enteral or intravenous nutrition concurrently. However, patients face barriers to receiving sufficient nutritional support due to various factors [12]. Inadequate nutritional support may lead to malnutrition and is reported to affect almost half of hospitalized patients by previous studies [4,5]. Nutritional support aims to prevent negative outcomes such as increased infection rates, muscle loss, and delayed wound healing due to nutritional deficiencies [2]. The guidelines for nutritional support in critically ill patients strongly recommend initiating ENS within 48 hours of admission to prevent complications [24]. Nutritional support is essential not only for critically ill patients but also for all hospitalized patients when considering factors such as restricted activity, sensory loss (taste, smell), and surgery, which can contribute to nutritional deficiencies [25]. Therefore, we determined the impact of ENS within 48 hours of admission for general ward patients undergoing fasting or insufficient oral intake.
In this study, the average amounts of calories and protein supplied compared to nutritional goals were analyzed to determine whether ENS achieves the nutritional requirements for general ward patients. The rates of the calories and protein supplied were significantly higher in the ENS group compared to the delayed nutritional support group. Similarly, in a study by Koga et al. (2018) [8], a significant difference was observed in the amounts of calories and protein supplied between the group receiving early enteral nutrition within 48 hours of admission and the group receiving delayed enteral nutrition. The early enteral nutrition group had significantly higher amounts than the delayed enteral nutrition group. Furthermore, Pardo et al. (2023) [10] reported that the ENS group reached the target calories faster than the delayed nutritional support group, and the amount of calories supplied was also higher. Based on both this study and prior studies, ENS has a positive effect on achieving the nutritional goals for general ward patients.
Proper nutritional supply is related to biomarkers reflecting nutritional status. In a systematic review and meta-analysis by Zhang et al. (2017) [26], serum albumin, prealbumin, hemoglobin, total cholesterol, and total protein were found to be useful biomarkers to access malnutrition in adults. Unfortunately, albumin level was not significantly different between the ENS group and the control group. Albumin is influenced not only by the nutritional status of the patient but also by hepatic diseases, acute inflammatory conditions, and dehydration [27,28]. Particularly, serum albumin decreases sharply in inflammatory stress status, and guidelines suggest that recovery through active nutritional support may be unattainable [27]. For these reasons, we concluded that ENS had an insufficient effect on albumin in this study.
Hemoglobin is also a biomarker that reflects malnutrition [26]. In this study, hemoglobin levels, which are known to decrease in cases of malnutrition, improved significantly at discharge in the ENS group [27]. The components of hemoglobin require amino acids, vitamins, including vitamin B6, and iron [29,30]. This means that an inadequate nutrient supply can decrease the synthesis of hemoglobin. Therefore, we suggest that ENS improves hemoglobin and nutritional status by providing necessary nutrients.
In this study, the levels of AST, BUN, creatinine, and CRP in the control group were significantly higher compared to the ENS group at admission. These biomarkers are indicators that reflect impaired liver function, renal dysfunction, and inflammation [27]. Therefore, abnormalities associated with these biomarkers might be one reason to delay nutritional support in this study. However, an absolute contraindication of nutritional support is hemodynamic instability, requiring fluid resuscitation, septic shock, mean arterial pressure below 60 mmHg, or an escalating demand for vasoactive support [31], and not the abnormality of biomarkers. Moreover, as the hemodynamic stability of general ward patients tends to be constant, ENS may be administered. This demonstrates the importance of clinicians acquiring specialized knowledge regarding the indications and contraindications of nutritional support. Additionally, according to recent studies, inadequate medical staff education, along with factors such as excessive workload and personnel shortages, was identified as causes for inadequate nutritional support for patients [3,32,33]. Therefore, it is believed that the causes of delayed nutritional support in this study may also be related to these factors. Hence, it is deemed necessary to establish systems at the hospital and national levels to address this issue, including the education of medical staff.
In this study, the prevalence of patients with medical conditions was significantly higher in the control group than in the ENS group. Additionally, the biomarkers indicating renal and liver functions, as previously mentioned, were higher in the control group. This suggests that patients with chronic illnesses or complex underlying diseases might be considered for transfer to the ICU [34]. However, both of the groups exhibited elevated levels of BUN, creatinine, ALT, AST, and CRP at admission, surpassing the normal range. Given that BUN with a threshold of 20 mg/dL is a predictive factor for ICU admission, both the control and ENS groups indicate a high risk of ICU admission [35]. Therefore, the significantly lower ICU admission rate in the ENS group compared to the control group indicates the importance of ENS for general ward patients.
The transfer of patients from general wards to the ICU demonstrates higher severity and mortality rates compared to transfers that occur through alternative routes such as emergency or operating rooms [13]. Preventing transfers from general wards to the ICU is considered to reduce patient mortality and have a positive impact on prognosis. One risk factor influencing the decision to transfer patients from the general ward to the ICU is the SOFA score [13,16-18]. According to prior studies, the SOFA score was reported as indicative of a patient’s nutritional status [36,37], and ENS can improve a patient’s nutritional status [3,7-11].
There are several limitations in this study. Firstly, we did not include the data of patients with underlying disease and clinical status, such as operation, trauma, and others. Secondly, the study did not conduct various blood biomarkers related to malnutrition (prealbumin, total protein). Thirdly, the significant differences between the two groups in indicators related to renal and liver function at admission suggest that they may act as factors attenuating the positive effects of ENS. Lastly, we could not compare the nutritional status of patients at admission and discharge due to insufficient data for nutritional status assessment at the time of discharge.
We suggest conducting a multi-center prospective study on ENS in the future. This would address the limitations of this single-center retrospective study and further confirm the im- pact of ENS.
Improving nutritional status through ENS is reflected in the improvement of the SOFA score, which can decrease the risk factor for ICU admission. The significantly lower ICU admission in the ENS group compared to the control group of this study also supports the evidence shown in previous studies.
This study contributes to the limited studies on ENS for general ward patients and provides scientific evidence to substantiate the necessity of ENS for general ward patients. Furthermore, it is strengthened by its focus on the domestic population.
Authors’ contribution
Conceptualization: CYK, DSK. Data curation: HSK, MRL. Formal analysis: SL, SWH. Investigation: MRL, DSK, HSK. Methodology: CYK, SWH, SHK. Project administration: SHK, HSK, CYK. Resources: CYK, JDY, SWH, MRL, DSK, SL, SHK, HSK. Supervision: CYK. Validation: JDY, SWH, SHK. Visualization: MRL, DSK, HSK. Writing – original draft: HSK, SL. Writing – review and editing: JDY, SWH, MRL.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
None.
Supplementary materials
Supplementary materials can be found via https://doi.org/10.15747/ACNM.2024.16.2.57
Supplement Table 1. Distribution of medical departments.
Supplement Table 2. Daily required and delivered nutritional amount in the two groups.
Supplement Table 3. Logistic regression analysis of general characteristics and ENS on ICU admission.
Supplement Table 4. Standardized mean difference before and after PSM.
Fig. 1
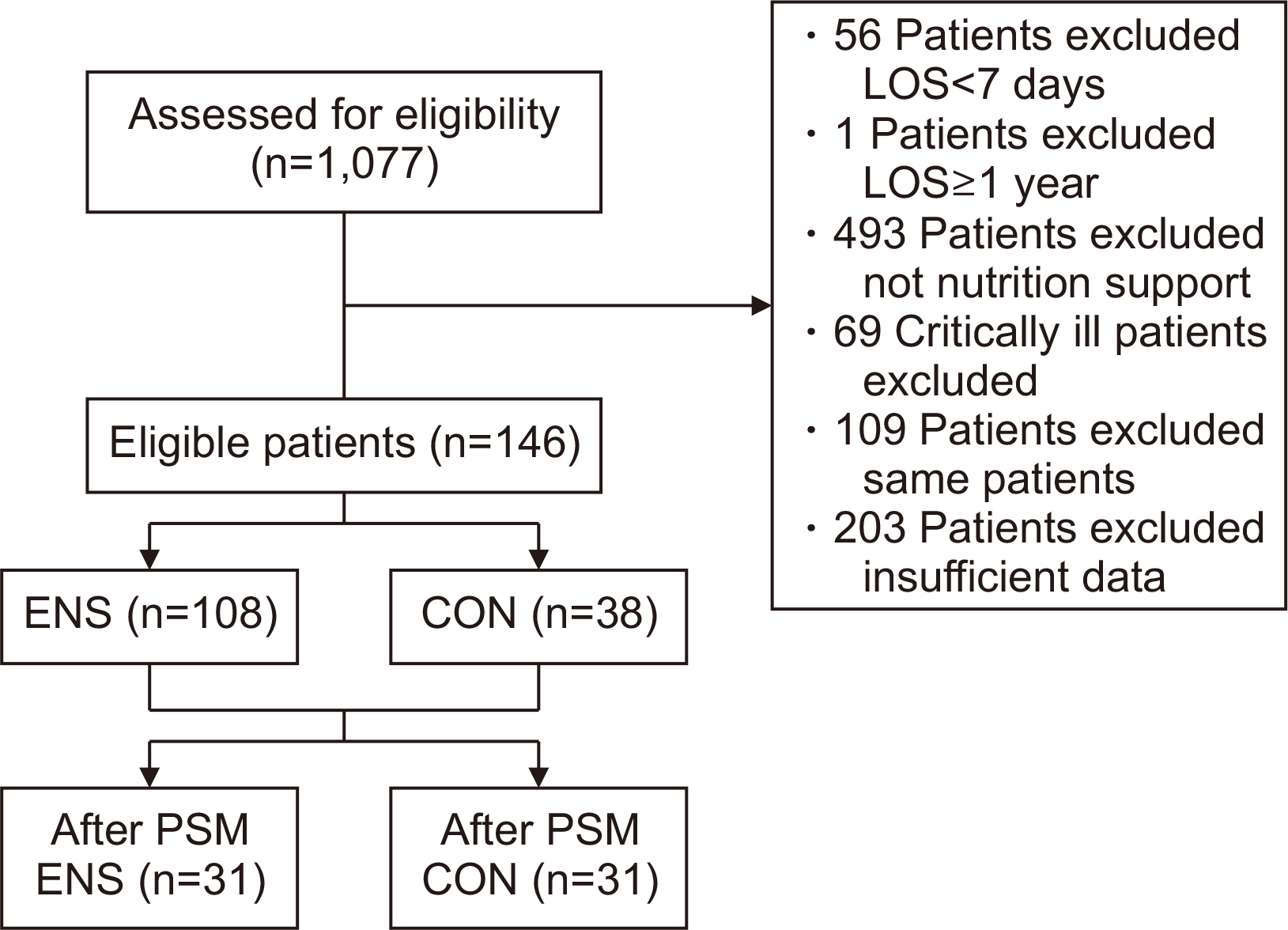
low chart of this study. LOS = length of stay; ENS = patients who received enteral or parenteral nutrition 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; PSM = propensity score matching.
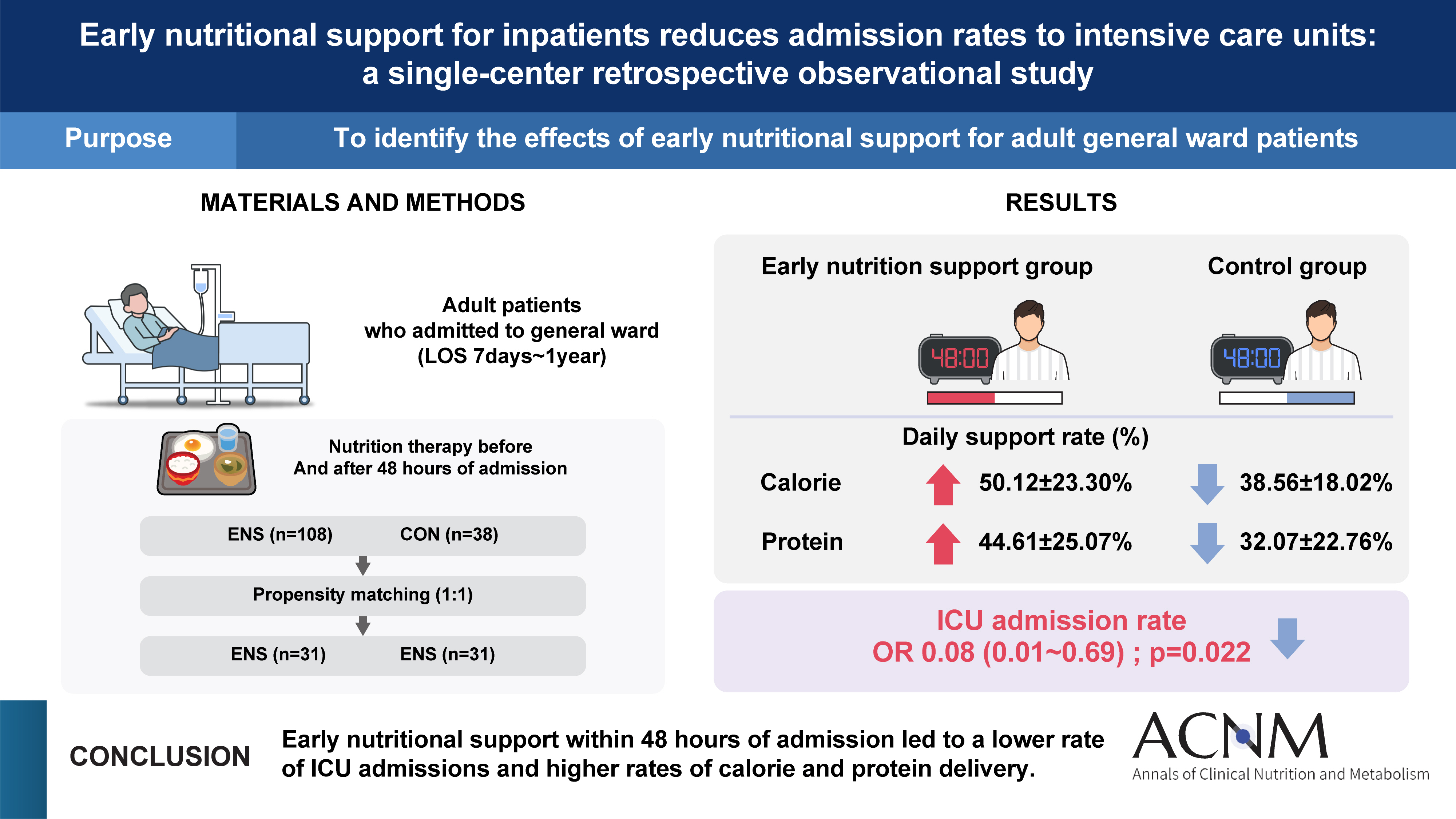
Table 1
Baseline characteristics of the two groups
| Variable | ENS (n=108) | CON (n=38) | P-value |
|---|---|---|---|
| Sex | |||
| Male | 64 (59.3) | 21 (55.3) | 0.705b |
| Female | 44 (40.7) | 17 (44.7) | |
| Age (yr) | 77.56±9.79 | 81.66±9.34 | 0.028c |
| Admission type | |||
| Medical | 90 (83.3) | 38 (100) | 0.007b |
| Surgical | 18 (16.7) | 0 (0) | |
| Height (cm) | 160.50±8.90 | 163.18±10.27 | 0.061c |
| Weight (kg) | 50.15±10.47 | 53.00±12.67 | 0.233c |
| BMI (kg/m2) | 19.41±3.56 | 19.86±4.54 | 0.703c |
| BMI range (kg/m2) | |||
| <18.5 (underweight) | 51 (47.2) | 17 (44.7) | 0.677b |
| 18.5–22.9 (normal) | 39 (36.1) | 14 (36.8) | |
| 23.0–24.9 (overweight) | 10 (9.3) | 2 (5.3) | |
| ≥25.0 (obese) | 8 (7.4) | 5 (13.2) | |
| PIBW (%) | 89.57±16.87 | 91.71±21.51 | 0.703c |
| Smoking status | |||
| Former smoker | 25 (23.1) | 9 (23.7) | >0.999b |
| Nonsmoker | 79 (73.1) | 28 (73.7) | |
| Current smoker | 4 (3.7) | 1 (2.6) | |
| Drinking status | |||
| Former | 22 (20.4) | 12 (31.6) | 0.252b |
| None | 78 (72.2) | 22 (57.9) | |
| Current | 8 (7.4) | 4 (10.5) | |
| Nutrition consultationa | |||
| Yes | 26 (24.1) | 6 (15.8) | 0.365b |
| No | 82 (75.9) | 32 (84.2) | |
| Nutrition support access | |||
| EN only | 28 (25.9) | 18 (47.4) | 0.045b |
| PN only | 17 (15.7) | 3 (7.9) | |
| EN & PN | 63 (58.3) | 17 (44.7) | |
| Nutritional status | |||
| No malnutrition | 30 (27.8) | 5 (13.2) | 0.057b |
| Moderate malnutrition | 33 (30.6) | 19 (50.0) | |
| Severe malnutrition | 45 (41.7) | 14 (36.8) |
Values are presented as number (%) or mean±standard deviation.
aConsultation for nutrition support.
bStatistical analysis by χ2-test, cstatistical analysis by Mann–Whitney U-test.
ENS = patients who received enteral or parenteral nutrition within 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; BMI = body mass index; PIBW = percentage ideal body weight; EN = enteral nutrition; PN = parenteral nutrition.
Table 2
Outcomes of patients in the two groups
| Variable | ENS (n=108) | CON (n=38) | P-value |
|---|---|---|---|
| Length of NPO (day) | 4.23±6.45 | 6.32±5.69 | <0.001a |
| Length of stay (day) | 22.83±14.89 | 27.42±13.83 | 0.016a,c |
| ICU admission | |||
| Yes | 11 (10.2) | 10 (26.3) | 0.019b,c |
| No | 97 (89.8) | 28 (73.7) | |
| In-hospital mortality | |||
| Yes | 10 (9.3) | 9 (23.7) | 0.029b |
| No | 98 (90.7) | 29 (76.3) |
Values are presented as mean±standard deviation or number (%).
ENS = patients who received enteral or parenteral nutrition within 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; NPO = nil per os; ICU = intensive care unit.
aStatistical analysis by Mann–Whitney U-test; bstatistical analysis by χ2-test; cP<0.05 by χ2-test in internal medicine patients of sub-group.
Table 3
Daily required and delivered nutrition amount in the two groups
| Variable | ENS (n=108) | CON (n=38) | P-valuea |
|---|---|---|---|
| Energy (kcal) | |||
| Requirement | 1,388.23±181.52 | 1,434.87±203.64 | 0.113 |
| Order (delivered) | 678.02±294.79 | 546.18±260.58 | 0.016b |
| Total ordered/required calorie ratio (%) | 50.12±23.30 | 38.56±18.02 | 0.006b,c |
| Protein (g) | |||
| Requirement | 59.99±13.43 | 52.00±12.83 | 0.002 |
| Order (delivered) | 25.24±12.39 | 16.74±12.54 | <0.001d |
| Total ordered/required protein ratio (%) | 44.61±25.07 | 32.07±22.76 | 0.002c |
Values are presented as mean±standard deviation.
ENS = patients who received enteral or parenteral nutrition within 48 hours of admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission.
aStatistical analysis by Mann–Whitney U-test; bstatistical analysis by independent t-test; cP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group; dP<0.05 by independent t-test in internal medicine patients of sub-group.
Table 4
Laboratory data in the two groups
| Variable | ENS (n=108) | CON (n=38) | P-valueb | P-valuec | |||||
|---|---|---|---|---|---|---|---|---|---|
| Admission | Discharge | P-valuea | Admission | Discharge | P-valuea | ||||
| Albumin (g/dL) | 3.21±0.66 | 3.10±0.47 | 0.061 | 2.97±0.51 | 2.95±0.42 | 0.879 | 0.098 | 0.093 | |
| TLC (cell/mm3) | 856.18±650.48 | 1,191.21±586.11 | <0.001g | 920.16±670.09 | 1,309.48±828.75 | <0.001g | 0.641 | 0.882 | |
| Hb (g/dL) | 10.71±2.50 | 9.85±1.58 | <0.001g | 10.89±2.83 | 9.15±1.27 | 0.002d,g | 0.717e | 0.015f,h | |
| Hct (%) | 32.19±8.23 | 32.15±21.27 | 0.985d,g | 33.34±8.36 | 28.51±3.91 | 0.003d,g | 0.418e | 0.008h | |
| Glucose (mg/L) | 156.92±77.00 | 152.82±71.55 | 0.258 | 191.82±100.62 | 136.25±42.89 | 0.007g | 0.114 | 0.117f | |
| BUN (mg/dL) | 33.23±32.42 | 29.14±29.55 | 0.172 | 64.61±48.74 | 28.47±22.11 | <0.001g | <0.001h | 0.503 | |
| Creatinine (mg/dL) | 1.63±2.50 | 1.19±1.47 | <0.001g | 2.71±3.42 | 1.18±0.07 | <0.001g | <0.001h | 0.478 | |
| AST (IU/L) | 43.06±40.42 | 57.94±125.30 | 0.537 | 165.82±507.39 | 36.97±25.59 | 0.004g | 0.012h | 0.635 | |
| ALT (IU/L) | 26.80±29.87 | 28.36±40.84 | 0.490 | 64.84±145.14 | 27.75±24.22 | 0.295 | 0.077 | 0.720 | |
| Na (mmol/L) | 136.47±7.68 | 137.52±7.07 | 0.268 | 140.34±11.53 | 137.71±5.11 | 0.359 | 0.118 | 0.878f | |
| K (mmol/L) | 4.07±1.02 | 4.05±0.79 | 0.867 | 4.22±1.03 | 3.87±0.65 | 0.064 | 0.172 | 0.175 | |
| Cl (mmol/L) | 107.73±28.77 | 103.60±17.88 | 0.003g | 107.61±10.75 | 102.74±7.53 | 0.022d,g | 0.260 | 0.837 | |
| Ca (mg/dL) | 8.46±1.06 | 8.73±0.77 | 0.105 | 8.42±0.99 | 8.35±0.77 | 0.713d | 0.749 | 0.027 | |
| P (mg/dL) | 3.44±1.91 | 3.28±1.38 | 0.855 | 4.46±2.41 | 3.06±1.11 | 0.001g | 0.041h | 0.460 | |
| CRP (mg/L) | 87.90±85.11 | 35.81±41.24 | <0.001g | 142.62±70.01 | 54.81±50.05 | <0.001g | <0.001h | 0.013 | |
Values are presented as mean±standard deviation.
ENS = patients who received enteral or parenteral nutritional support within 48 hours of admission; CON = patients who received enteral or parenteral nutritional support 48 hours after admission; TLC = total lymphocyte count; Hb = hemoglobin; Hct = hematocrit; BUN = blood urea nitrogen; AST = aspartate aminotransferase; ALT=alanine aminotransferase; CRP = C-reactive protein.
aStatistical analysis by Wilcoxon signed-rank test within the group; bstatistical analysis by Mann–Whitney U-test at admission between group; cstatistical analysis by Mann–Whitney U-test at discharge between groups; dstatistical analysis by paired t-test; estatistical analysis by independent t-test at admission; fstatistical analysis by independent t-test at discharge; gP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group between groups; hP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group between groups.
Table 5
Effect of ENS on ICU admission for general ward patients
| Variable | Model 1 (n=146) | Model 2 (n=146) | Model 3 (n=62) | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | P-value | aOR (95% CI) | P-value | OR (95% CI) | P-value | |||
| No | 1 | 1 | 1 | |||||
| Yes | 0.32 (0.12–0.82) | 0.018 | 0.14 (0.04–0.53) | 0.004 | 0.08 (0.01–0.69) | 0.022 | ||
Model 1 = univariable logistic regression; Model 2 = multivariable analysis with adjustment of age, admission type, and nutrition support access; Model 3 = logistic regression after propensity score matching.
ENS = patients who received enteral or parenteral nutrition within 48 hours of admission; ICU = intensive care unit; OR = odds ratio; aOR = adjusted odds ratio.
- 1. Skipper A. Agreement on defining malnutrition. JPEN J Parenter Enteral Nutr 2012;36:261-2. ArticlePubMedPDF
- 2. Böhne SEJ, Hiesmayr M, Sulz I, Tarantino S, Wirth R, Volkert D. Recent and current low food intake - prevalence and associated factors in hospital patients from different medical specialities. Eur J Clin Nutr 2022;76:1440-8. ArticlePubMedPMCPDF
- 3. Seol E, Suh YS, Ju DL, Bae HJ, Lee HJ. Characteristics and clinical course of patients who received enteral or parenteral nutrition in tertiary referral hospitals in Korea. J Clin Nutr 2016;8:58-65. Article
- 4. Keller U. Nutritional laboratory markers in malnutrition. J Clin Med 2019;8:775.ArticlePubMedPMC
- 5. Hwang HS, Lee SH, Lee H, Kim KS, Chung SJ, Lee JG. Effects of nutrition consultation on nutritional status in critically ill surgical patients. J Clin Nutr 2015;7:28-34. Article
- 6. Lee JS, Cho MR, Lee GJ. Validation of the developed nutritional screening tool for hospital patients. Korean J Nutr 2010;43:189-96. Article
- 7. Kim BH, Kim H, Kwon O. A comparison of nutritional status by intensive nutritional support in enteral nutrition patients. J Nutr Health 2018;51:132-9. ArticlePDF
- 8. Koga Y, Fujita M, Yagi T, Todani M, Nakahara T, Kawamura Y, et al. Early enteral nutrition is associated with reduced in-hospital mortality from sepsis in patients with sarcopenia. J Crit Care 2018;47:153-8. ArticlePubMed
- 9. Haac B, Henry S, Diaz J, Scalea T, Stein D. Early enteral nutrition is associated with reduced morbidity in critically ill soft tissue patients. Am Surg 2018;84:1003-9. ArticlePubMedPDF
- 10. Pardo E, Lescot T, Preiser JC, Massanet P, Pons A, Jaber S, et al. FRANS Study Group. Association between early nutrition support and 28-day mortality in critically ill patients: the FRANS prospective nutrition cohort study. Crit Care 2023;27:7.PubMedPMC
- 11. Singer P, Blaser AR, Berger MM, Calder PC, Casaer M, Hiesmayr M, et al. ESPEN practical and partially revised guideline: clinical nutrition in the intensive care unit. Clin Nutr 2023;42:1671-89. ArticlePubMed
- 12. Gressies C, Tribolet P, Schuetz P. Nutrition issues in the general medical ward patient: from general screening to specific diagnosis and individualized treatment. JPEN J Parenter Enteral Nutr 2023;47 Suppl 1:S16-23. ArticlePubMedPDF
- 13. Lee JR, Choi HR. Analysis of risk factors to predict intensive care unit transfer in medical in-patients. J Korean Biol Nurs Sci 2014;16:259-66. Article
- 14. Devita MA, Bellomo R, Hillman K, Kellum J, Rotondi A, Teres D, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med 2006;34:2463-78. ArticlePubMed
- 15. Jang JN, Lee YM, Park HJ, Lee HJ. The risk factors related to early readmission to the intensive care unit. J Korean Crit Care Nurs 2019;12:36-45. ArticlePDF
- 16. Wilson RM, Harrison BT, Gibberd RW, Hamilton JD. An analysis of the causes of adverse events from the Quality in Australian Health Care Study. Med J Aust 1999;170:411-5. ArticlePubMedPDF
- 17. Hillman KM, Bristow PJ, Chey T, Daffurn K, Jacques T, Norman SL, et al. Duration of life-threatening antecedents prior to intensive care admission. Intensive Care Med 2002;28:1629-34. ArticlePubMedPDF
- 18. Kause J, Smith G, Prytherch D, Parr M, Flabouris A, Hillman K. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom--the ACADEMIA study. Resuscitation 2004;62:275-82. ArticlePubMed
- 19. Cederholm T, Jensen GL, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. J Cachexia Sarcopenia Muscle 2019;10:207-217. ArticlePubMedPMCPDF
- 20. Takagi K, Murotani K, Kamoshita S, Kuroda A. Clinical impact of lipid injectable emulsion in internal medicine inpatients exclusively receiving parenteral nutrition: a propensity score matching analysis from a Japanese medical claims database. BMC Med 2022;20:371.ArticlePubMedPMCPDF
- 21. Austin PC. An Introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res 2011;46:399-424. ArticlePubMedPMC
- 22. Tomino T, Harada N, Toshida K, Tomiyama T, Kosai Y, Kurihara T, et al. Effect of early enteral nutrition on graft loss after living donor liver transplantation: a propensity score matching analysis. Transplant Proc 2023;55:2164-70. ArticlePubMed
- 23. Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun Stat Simul Comput 2009;38:1228-34. Article
- 24. McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. Society of Critical Care Medicine; American Society for Parenteral and Enteral Nutrition. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2016;40:159-211. PubMed
- 25. Barker LA, Gout BS, Crowe TC. Hospital malnutrition: prevalence, identification and impact on patients and the healthcare system. Int J Environ Res Public Health 2011;8:514-27. ArticlePubMedPMC
- 26. Zhang Z, Pereira SL, Luo M, Matheson EM. Evaluation of blood biomarkers associated with risk of malnutrition in older adults: a systematic review and meta-analysis. Nutrients 2017;9:829.ArticlePubMedPMC
- 27. Korean Dietetic Association (KDA). Korean Dietetic Association (KDA). Manual of medical nutrition therapy. 4th ed. Vol. 1. KDA, 2022.
- 28. Marcason W. Should albumin and prealbumin be used as indicators for malnutrition? J Acad Nutr Diet 2017;117:1144.ArticlePubMed
- 29. Park HS, Lim YS, Kim KA. Park HS, Lim YS, Kim KA. Advanced nutrition and metabolism. Hyoil, 2010.
- 30. Lanser L, Fuchs D, Kurz K, Weiss G. Physiology and inflammation driven pathophysiology of iron homeostasis-mechanistic insights into anemia of inflammation and its treatment. Nutrients 2021;13:3732.ArticlePubMedPMC
- 31. Tadlock MD, Hannon M, Davis K, Lancman M, Pamplin J, Shackelford S, et al. Nutritional support using enteral and parenteral methods. Mil Med 2018;183(Suppl 2):153-60. ArticlePubMed
- 32. Jeong HS, Teong CH, Choi YJ, Kim WJ, Lee AR. 2014;Attitudes of medical staff and factors related to nutritional support for patient care in a university hospital. J Clin Nutr 6:37-41. Article
- 33. Choi J, Park E. Different perceptions of clinical nutrition services between doctors and dietitians in the Busan-Gyeongnam area. J Korean Diet Assoc 2013;19:69-81. Article
- 34. Park T, Hong SB, Lim CM, Koh Y. Effect of admission time to the medical intensive care unit on acute critical patient outcomes. Korean J Crit Care Med 2010;25:71-5. Article
- 35. Gearhart AM, Furmanek S, English C, Ramirez J, Cavallazzi R. Predicting the need for ICU admission in community-acquired pneumonia. Respir Med 2019;155:61-5. ArticlePubMed
- 36. Huang Y, Zhang Q, Li P, Chen M, Wang R, Hu J, et al. The prognostic nutritional index predicts all-cause mortality in critically ill patients with acute myocardial infarction. BMC Cardiovasc Disord 2023;23:339.ArticlePubMedPMCPDF
- 37. Gao T, Yu X. Association between nutritional status scores and the 30-day mortality in patients with acute kidney injury: an analysis of MIMIC-III database. BMC Nephrol 2023;24:296.ArticlePubMedPMCPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteEarly nutritional support for inpatients reduces admission rates to intensive care units in Korea: a single-center case-control study
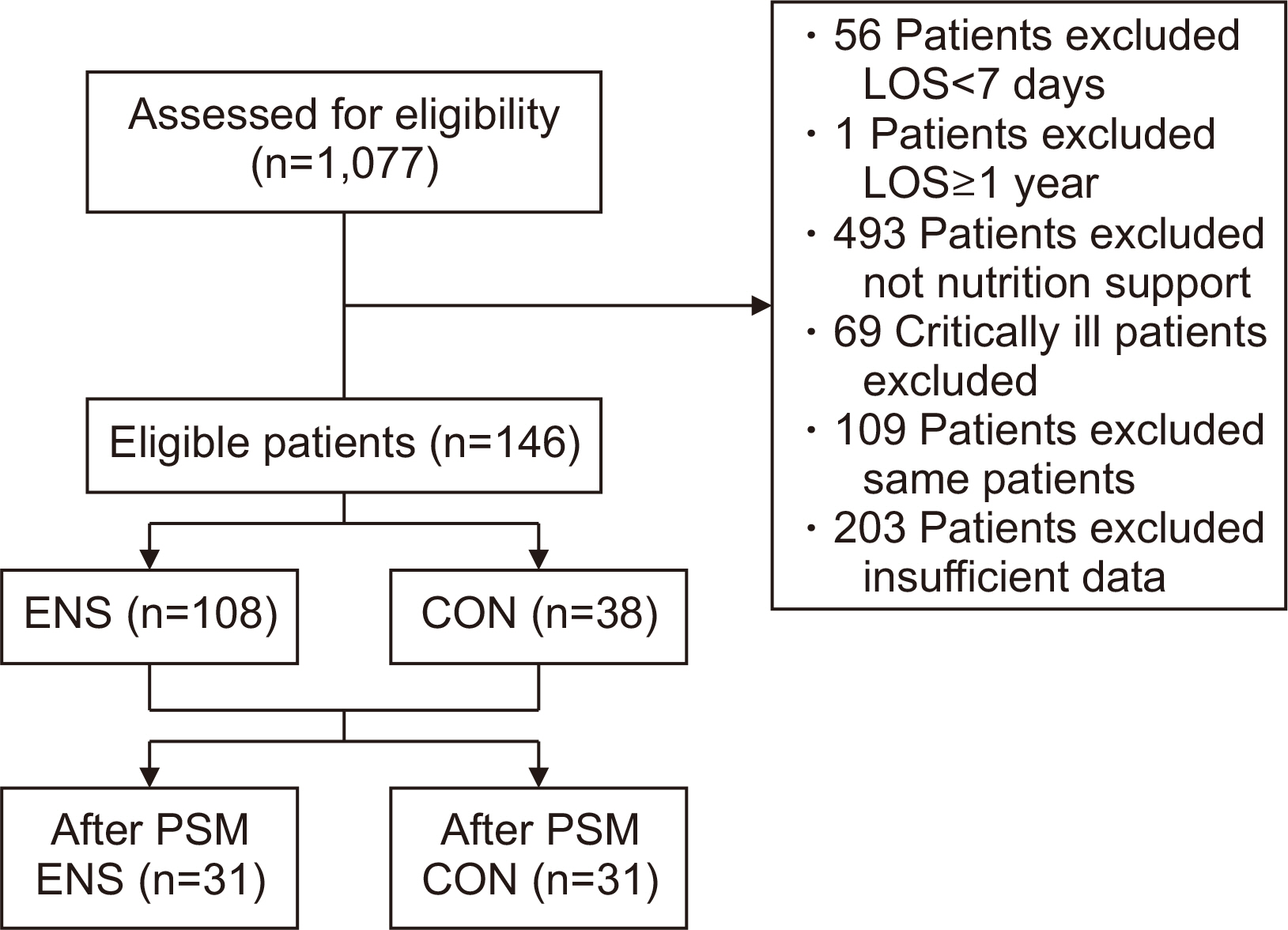
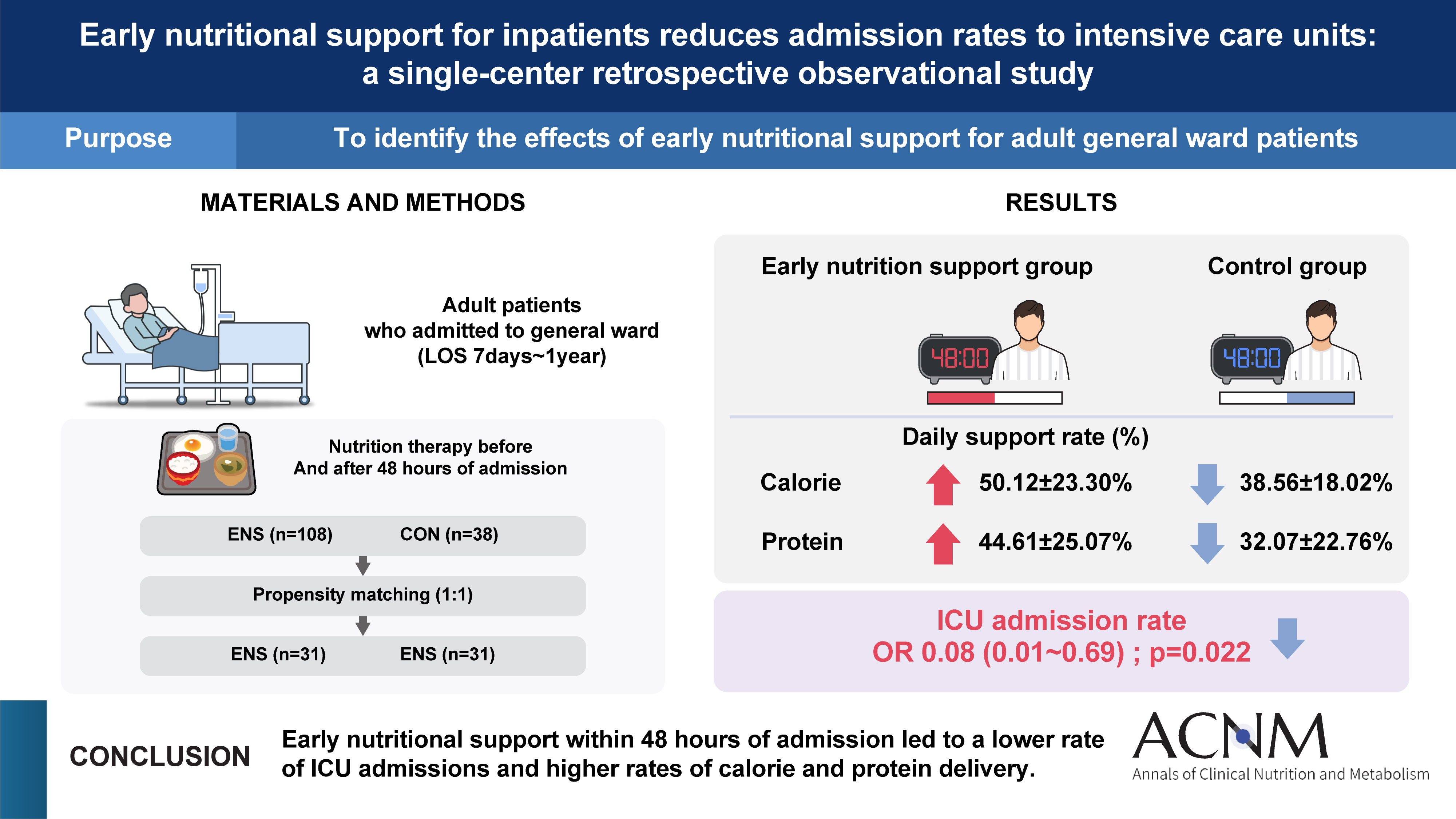
Fig. 1
low chart of this study. LOS = length of stay; ENS = patients who received enteral or parenteral nutrition 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; PSM = propensity score matching.
Graphical abstract
Fig. 1
Graphical abstract
Early nutritional support for inpatients reduces admission rates to intensive care units in Korea: a single-center case-control study
Baseline characteristics of the two groups
| Variable | ENS (n=108) | CON (n=38) | P-value |
|---|---|---|---|
| Sex | |||
| Male | 64 (59.3) | 21 (55.3) | 0.705 |
| Female | 44 (40.7) | 17 (44.7) | |
| Age (yr) | 77.56±9.79 | 81.66±9.34 | 0.028 |
| Admission type | |||
| Medical | 90 (83.3) | 38 (100) | 0.007 |
| Surgical | 18 (16.7) | 0 (0) | |
| Height (cm) | 160.50±8.90 | 163.18±10.27 | 0.061 |
| Weight (kg) | 50.15±10.47 | 53.00±12.67 | 0.233 |
| BMI (kg/m2) | 19.41±3.56 | 19.86±4.54 | 0.703 |
| BMI range (kg/m2) | |||
| <18.5 (underweight) | 51 (47.2) | 17 (44.7) | 0.677 |
| 18.5–22.9 (normal) | 39 (36.1) | 14 (36.8) | |
| 23.0–24.9 (overweight) | 10 (9.3) | 2 (5.3) | |
| ≥25.0 (obese) | 8 (7.4) | 5 (13.2) | |
| PIBW (%) | 89.57±16.87 | 91.71±21.51 | 0.703 |
| Smoking status | |||
| Former smoker | 25 (23.1) | 9 (23.7) | >0.999 |
| Nonsmoker | 79 (73.1) | 28 (73.7) | |
| Current smoker | 4 (3.7) | 1 (2.6) | |
| Drinking status | |||
| Former | 22 (20.4) | 12 (31.6) | 0.252 |
| None | 78 (72.2) | 22 (57.9) | |
| Current | 8 (7.4) | 4 (10.5) | |
| Nutrition consultation |
|||
| Yes | 26 (24.1) | 6 (15.8) | 0.365 |
| No | 82 (75.9) | 32 (84.2) | |
| Nutrition support access | |||
| EN only | 28 (25.9) | 18 (47.4) | 0.045 |
| PN only | 17 (15.7) | 3 (7.9) | |
| EN & PN | 63 (58.3) | 17 (44.7) | |
| Nutritional status | |||
| No malnutrition | 30 (27.8) | 5 (13.2) | 0.057 |
| Moderate malnutrition | 33 (30.6) | 19 (50.0) | |
| Severe malnutrition | 45 (41.7) | 14 (36.8) |
Values are presented as number (%) or mean±standard deviation.
aConsultation for nutrition support.
bStatistical analysis by χ2-test, cstatistical analysis by Mann–Whitney U-test.
ENS = patients who received enteral or parenteral nutrition within 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; BMI = body mass index; PIBW = percentage ideal body weight; EN = enteral nutrition; PN = parenteral nutrition.
Outcomes of patients in the two groups
| Variable | ENS (n=108) | CON (n=38) | P-value |
|---|---|---|---|
| Length of NPO (day) | 4.23±6.45 | 6.32±5.69 | <0.001 |
| Length of stay (day) | 22.83±14.89 | 27.42±13.83 | 0.016 |
| ICU admission | |||
| Yes | 11 (10.2) | 10 (26.3) | 0.019 |
| No | 97 (89.8) | 28 (73.7) | |
| In-hospital mortality | |||
| Yes | 10 (9.3) | 9 (23.7) | 0.029 |
| No | 98 (90.7) | 29 (76.3) |
Values are presented as mean±standard deviation or number (%).
ENS = patients who received enteral or parenteral nutrition within 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; NPO = nil per os; ICU = intensive care unit.
aStatistical analysis by Mann–Whitney U-test; bstatistical analysis by χ2-test; cP<0.05 by χ2-test in internal medicine patients of sub-group.
Daily required and delivered nutrition amount in the two groups
| Variable | ENS (n=108) | CON (n=38) | P-value |
|---|---|---|---|
| Energy (kcal) | |||
| Requirement | 1,388.23±181.52 | 1,434.87±203.64 | 0.113 |
| Order (delivered) | 678.02±294.79 | 546.18±260.58 | 0.016 |
| Total ordered/required calorie ratio (%) | 50.12±23.30 | 38.56±18.02 | 0.006 |
| Protein (g) | |||
| Requirement | 59.99±13.43 | 52.00±12.83 | 0.002 |
| Order (delivered) | 25.24±12.39 | 16.74±12.54 | <0.001 |
| Total ordered/required protein ratio (%) | 44.61±25.07 | 32.07±22.76 | 0.002 |
Values are presented as mean±standard deviation.
ENS = patients who received enteral or parenteral nutrition within 48 hours of admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission.
aStatistical analysis by Mann–Whitney U-test; bstatistical analysis by independent t-test; cP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group; dP<0.05 by independent t-test in internal medicine patients of sub-group.
Laboratory data in the two groups
| Variable | ENS (n=108) | CON (n=38) | P-value |
P-value |
|||||
|---|---|---|---|---|---|---|---|---|---|
| Admission | Discharge | P-value |
Admission | Discharge | P-value |
||||
| Albumin (g/dL) | 3.21±0.66 | 3.10±0.47 | 0.061 | 2.97±0.51 | 2.95±0.42 | 0.879 | 0.098 | 0.093 | |
| TLC (cell/mm3) | 856.18±650.48 | 1,191.21±586.11 | <0.001 |
920.16±670.09 | 1,309.48±828.75 | <0.001 |
0.641 | 0.882 | |
| Hb (g/dL) | 10.71±2.50 | 9.85±1.58 | <0.001 |
10.89±2.83 | 9.15±1.27 | 0.002 |
0.717 |
0.015 |
|
| Hct (%) | 32.19±8.23 | 32.15±21.27 | 0.985 |
33.34±8.36 | 28.51±3.91 | 0.003 |
0.418 |
0.008 |
|
| Glucose (mg/L) | 156.92±77.00 | 152.82±71.55 | 0.258 | 191.82±100.62 | 136.25±42.89 | 0.007 |
0.114 | 0.117 |
|
| BUN (mg/dL) | 33.23±32.42 | 29.14±29.55 | 0.172 | 64.61±48.74 | 28.47±22.11 | <0.001 |
<0.001 |
0.503 | |
| Creatinine (mg/dL) | 1.63±2.50 | 1.19±1.47 | <0.001 |
2.71±3.42 | 1.18±0.07 | <0.001 |
<0.001 |
0.478 | |
| AST (IU/L) | 43.06±40.42 | 57.94±125.30 | 0.537 | 165.82±507.39 | 36.97±25.59 | 0.004 |
0.012 |
0.635 | |
| ALT (IU/L) | 26.80±29.87 | 28.36±40.84 | 0.490 | 64.84±145.14 | 27.75±24.22 | 0.295 | 0.077 | 0.720 | |
| Na (mmol/L) | 136.47±7.68 | 137.52±7.07 | 0.268 | 140.34±11.53 | 137.71±5.11 | 0.359 | 0.118 | 0.878 |
|
| K (mmol/L) | 4.07±1.02 | 4.05±0.79 | 0.867 | 4.22±1.03 | 3.87±0.65 | 0.064 | 0.172 | 0.175 | |
| Cl (mmol/L) | 107.73±28.77 | 103.60±17.88 | 0.003 |
107.61±10.75 | 102.74±7.53 | 0.022 |
0.260 | 0.837 | |
| Ca (mg/dL) | 8.46±1.06 | 8.73±0.77 | 0.105 | 8.42±0.99 | 8.35±0.77 | 0.713 |
0.749 | 0.027 | |
| P (mg/dL) | 3.44±1.91 | 3.28±1.38 | 0.855 | 4.46±2.41 | 3.06±1.11 | 0.001 |
0.041 |
0.460 | |
| CRP (mg/L) | 87.90±85.11 | 35.81±41.24 | <0.001 |
142.62±70.01 | 54.81±50.05 | <0.001 |
<0.001 |
0.013 | |
Values are presented as mean±standard deviation.
ENS = patients who received enteral or parenteral nutritional support within 48 hours of admission; CON = patients who received enteral or parenteral nutritional support 48 hours after admission; TLC = total lymphocyte count; Hb = hemoglobin; Hct = hematocrit; BUN = blood urea nitrogen; AST = aspartate aminotransferase; ALT=alanine aminotransferase; CRP = C-reactive protein.
aStatistical analysis by Wilcoxon signed-rank test within the group; bstatistical analysis by Mann–Whitney U-test at admission between group; cstatistical analysis by Mann–Whitney U-test at discharge between groups; dstatistical analysis by paired t-test; estatistical analysis by independent t-test at admission; fstatistical analysis by independent t-test at discharge; gP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group between groups; hP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group between groups.
Effect of ENS on ICU admission for general ward patients
| Variable | Model 1 (n=146) | Model 2 (n=146) | Model 3 (n=62) | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | P-value | aOR (95% CI) | P-value | OR (95% CI) | P-value | |||
| No | 1 | 1 | 1 | |||||
| Yes | 0.32 (0.12–0.82) | 0.018 | 0.14 (0.04–0.53) | 0.004 | 0.08 (0.01–0.69) | 0.022 | ||
Model 1 = univariable logistic regression; Model 2 = multivariable analysis with adjustment of age, admission type, and nutrition support access; Model 3 = logistic regression after propensity score matching.
ENS = patients who received enteral or parenteral nutrition within 48 hours of admission; ICU = intensive care unit; OR = odds ratio; aOR = adjusted odds ratio.
Table 1
Baseline characteristics of the two groups
Values are presented as number (%) or mean±standard deviation. aConsultation for nutrition support. bStatistical analysis by χ2-test, cstatistical analysis by Mann–Whitney U-test. ENS = patients who received enteral or parenteral nutrition within 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; BMI = body mass index; PIBW = percentage ideal body weight; EN = enteral nutrition; PN = parenteral nutrition.
Table 2
Outcomes of patients in the two groups
Values are presented as mean±standard deviation or number (%). ENS = patients who received enteral or parenteral nutrition within 48 hours after admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission; NPO = nil per os; ICU = intensive care unit. aStatistical analysis by Mann–Whitney U-test; bstatistical analysis by χ2-test; cP<0.05 by χ2-test in internal medicine patients of sub-group.
Table 3
Daily required and delivered nutrition amount in the two groups
Values are presented as mean±standard deviation. ENS = patients who received enteral or parenteral nutrition within 48 hours of admission; CON = patients who received enteral or parenteral nutrition support 48 hours after admission. aStatistical analysis by Mann–Whitney U-test; bstatistical analysis by independent t-test; cP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group; dP<0.05 by independent t-test in internal medicine patients of sub-group.
Table 4
Laboratory data in the two groups
Values are presented as mean±standard deviation. ENS = patients who received enteral or parenteral nutritional support within 48 hours of admission; CON = patients who received enteral or parenteral nutritional support 48 hours after admission; TLC = total lymphocyte count; Hb = hemoglobin; Hct = hematocrit; BUN = blood urea nitrogen; AST = aspartate aminotransferase; ALT=alanine aminotransferase; CRP = C-reactive protein. aStatistical analysis by Wilcoxon signed-rank test within the group; bstatistical analysis by Mann–Whitney U-test at admission between group; cstatistical analysis by Mann–Whitney U-test at discharge between groups; dstatistical analysis by paired t-test; estatistical analysis by independent t-test at admission; fstatistical analysis by independent t-test at discharge; gP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group between groups; hP<0.05 by Mann–Whitney U-test in internal medicine patients of sub-group between groups.
Table 5
Effect of ENS on ICU admission for general ward patients
Model 1 = univariable logistic regression; Model 2 = multivariable analysis with adjustment of age, admission type, and nutrition support access; Model 3 = logistic regression after propensity score matching. ENS = patients who received enteral or parenteral nutrition within 48 hours of admission; ICU = intensive care unit; OR = odds ratio; aOR = adjusted odds ratio.

