 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 18(1); 2026 > Article
- Original Article Current status and short-term results regarding frailty in patients undergoing gastrointestinal cancer resection in Japan: a retrospective cohort study
-
Asuka Yasueda1
 , Junichi Nishimura2, Seiji Ikeda3, Naotsugu Haraguchi4, Hirofumi Akita4, Hiroshi Wada4, Chu Matsuda4, Takeshi Omori4, Masayoshi Yasui4, Hironari Tamiya5, Hideaki Tahara6, Hiroshi Miyata4
, Junichi Nishimura2, Seiji Ikeda3, Naotsugu Haraguchi4, Hirofumi Akita4, Hiroshi Wada4, Chu Matsuda4, Takeshi Omori4, Masayoshi Yasui4, Hironari Tamiya5, Hideaki Tahara6, Hiroshi Miyata4 -
Annals of Clinical Nutrition and Metabolism 2026;18(1):54-62.
DOI: https://doi.org/10.15747/ACNM.25.0013
Published online: March 30, 2026
1Faculty of Health and Nutrition, Otemae University, Osaka, Japan
2Department of Medical Informatics, Osaka International Cancer Institute, Osaka, Japan
3Department of Rehabilitation, Osaka International Cancer Institute, Osaka, Japan
4Department of Gastroenterological Surgery, Osaka International Cancer Institute, Osaka, Japan
5Department of Orthopaedic Surgery, Osaka International Cancer Institute, Osaka, Japan
6Department of Clinical Research Center, Osaka International Cancer Institute, Osaka, Japan
- Corresponding author: Asuka Yasueda email: yasueda@otemae.ac.jp
This article is a secondary publication of an article in Japanese published in the Japanese Journal of Surgical Metabolism and Nutrition, 2023;57(4):127-134. https://doi.org/10.11638/jssmn.57.4_127. The editors of both journals have granted permission for secondary publication.
This article includes content that was presented at the 22nd Annual Meeting of the Japanese Society of Anti-Aging Medicine and the 44th Annual Meeting of the Japanese Society of Clinical Nutrition.
• Received: November 29, 2025 • Revised: January 4, 2026 • Accepted: January 8, 2026
© 2026 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition · Asian Society of Surgical Metabolism and Nutrition
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 564 Views
- 10 Download
Abstract
-
Purpose Frailty is a state of physical and cognitive decline that exists between robust health and the need for nursing care. Frailty is reported to occur at a high rate among patients with cancer and is associated with postoperative complications, such as delirium, infection, reduced survival, and rehospitalization. In this study, we investigated the incidence of frailty and surgical outcomes in patients who underwent surgery for gastrointestinal cancer.
-
Methods A total of 201 patients who underwent preoperative physical assessment at Osaka International Cancer Institute between July and September 2021 were included. The Japanese version of the Cardiovascular Health Study (J-CHS) index was used to assess the frequency of frailty and related postoperative outcomes.
-
Results Among the 201 patients, 27 (13%) were classified as frail and 126 (63%) as pre-frail. Of the 27 frail patients, 22 (81%) were older adults—a significantly higher proportion compared to the pre-frail/robust group (P=0.004). The median hospital stay for frail patients was 17 days (range, 5–98 days), which was significantly longer than that for robust patients (P<0.001). Postoperative complications occurred in 15 frail patients (56%), which was higher than in pre-frail (n=40, 32%) and robust (n=6, 13%) patients. Furthermore, multivariate analysis showed that frailty was an independent risk factor for postoperative complications.
-
Conclusion These findings indicate that frailty is common among older adults with gastrointestinal cancer and has a significant impact on both the length of hospital stay and the risk of postoperative complications.
Graphical abstract
Introduction
Frailty refers to a state of weakness, vulnerability, and senility and is considered a transitional stage between good health and the need for nursing care. According to the Japan Geriatrics Society, “Frailty is a state in which physiological reserves decline with age, increasing vulnerability to stress and resulting in outcomes such as impaired daily functioning, the need for nursing care, and death. This concept encompasses not only physical issues, such as decreased muscle strength and increased risk of falls due to loss of agility, but also mental and psychological issues, including cognitive impairment and depression, as well as social problems, such as living alone or experiencing economic hardship [1].” It is known that frailty, characterized by physical and mental vulnerability in older adults, can be improved with appropriate and targeted interventions.
It is well established that cancer—particularly when combined with prolonged hospitalization, invasive surgery, or chemotherapy/radiotherapy—can significantly impact prognosis. Frailty is strongly affected by the coexistence of lifestyle-related diseases. According to the “National Cancer Registry: Incidence and Rate Report” published by the Japanese Ministry of Health, Labour and Welfare in 2019, gastrointestinal cancers, especially colorectal cancer, represent a substantial proportion of cases: 43% in men and 29.7% in women [2]. Furthermore, a National Clinical Database survey by Hasegawa et al. (2019) [3] reported an increase in older patients undergoing gastrointestinal cancer surgery, along with a rise in preoperative comorbidities and postoperative complications. Although advanced age is often considered a risk factor, a review of optimal surgical treatment and geriatric assessment in older colorectal cancer patients suggests that surgery should not be withheld solely on the basis of age [4].
However, older patients frequently present with additional risk factors for postoperative complications, such as frailty, malnutrition (including low serum total protein and albumin levels), cognitive decline, comorbidities, polypharmacy, and sarcopenia (loss of skeletal muscle mass). These factors can increase the risks of death, sepsis, postoperative infection, and delirium [5]. Preoperative assessment of such risk factors has been reported to reduce both mortality and postoperative complications, shorten hospital stays, facilitate discharge to home, and help maintain activities of daily living and improve quality of life [6,7]. Nonetheless, a variety of risk factors for postoperative complications exist even among younger adults with cancer, particularly gastrointestinal cancers, yet little is known about frailty risk assessment independent of age.
The aim of this study was to investigate the impact of frailty on prognosis according to cancer site and age, and to examine the relationship between the incidence of frailty and surgical outcomes.
Methods
This study was approved by the Ethics Committee of the Osaka International Cancer Institute (Number: 18033-6). Informed consent was not required in accordance with institutional policy for this retrospective study.
This retrospective cohort study is described in accordance with the STROBE statement (https://www.strobe-statement.org/).
From July to September 2021, a retrospective analysis was conducted on 201 cases (131 males, 70 females; mean age, 67 years [range, 28–86 years]) selected from 268 patients who underwent gastrointestinal cancer resection at the Osaka International Cancer Institute. All included patients underwent preoperative physical function assessments, such as the 6-minute walking distance (6MWD), performed by the Department of Rehabilitation.
Of the 268 patients who underwent gastrointestinal cancer resection, those who did not receive surgical treatment were excluded (Fig. 1).
Preoperative baseline characteristics included age, five-item physical function, 6MWD, and grip strength. Outcome variables consisted of postoperative complications.
The frequency of frailty was assessed using the revised Japanese 2020 version of the Cardiovascular Health Study (J-CHS) criteria [8]. At the time of preoperative physical function assessment, five factors were evaluated: (1) weight loss (≥2 kg in 6 months), (2) fatigue, (3) decreased physical activity (exercise less than once a week), (4) decreased walking speed (<1.0 m/sec), and (5) decreased grip strength (<28 kg for men, <18 kg for women). Patients were categorized into three groups: frail (meeting three or more criteria), pre-frail (meeting one or two criteria), and robust (meeting none). Weight loss, fatigue, and physical activity were assessed using subjective participant reports. The 6MWD was measured according to American Thoracic Society guidelines. Grip strength was measured twice on each hand using a digital dynamometer (Grip-D, Takei Scientific Instruments Co., Ltd.), with the highest value recorded. Postoperative complications were classified according to the Japan Clinical Oncology Group postoperative complication criteria (Clavien-Dindo classification) [9]; complications not included in this classification were recorded as "other." The severity of complications was graded from I to V according to this system.
As all eligible patients from a single institution during the study period were included, selection bias was not an issue
No sample size estimation was performed because the study encompassed the entire target population.
All numerical data are presented as median (range). Statistical analyses were performed using JMP Pro 14 (SAS Institute Inc.). Differences between groups were analyzed using the Dunnett test, with the robust group as the control. Temporal changes were evaluated using the paired t-test before and after the intervention. The Fisher exact test was used to compare patient backgrounds between groups. Univariate and multivariate logistic regression analyses were conducted to identify independent risk factors for postoperative complications. A P-value less than 0.05 was considered statistically significant in all analyses.
Results
Among the 201 patients, 68 (34%) had upper gastrointestinal cancers, including gastric and esophageal cancers. Fifty-one patients (25%) had hepatobiliary and pancreatic cancers (such as liver, biliary tract, and pancreatic cancers), and 82 patients (41%) had lower gastrointestinal cancers, such as colon and rectal cancers. The baseline characteristics of the participants are presented in Table 1.
Patient characteristics by perioperative group are shown in Table 2. According to the J-CHS criteria [8], 27 cases (13%) were classified as frail, and 126 (63%) as pre-frail. Among the 27 frail cases, 22 (81%) were aged 65 years or older, a significantly higher proportion compared to 90 cases (52%) in the pre-frail and robust groups (P=0.004). With respect to sex, 20% of female patients were classified as frail, compared to 10% of male patients (P=0.05). The proportion of frailty increased among older adults in all cancer site categories, but there was no significant difference between sites (Fig. 2). The highest proportion of frailty by cancer site was observed in esophageal cancer at 27% (Fig. 3).
For preoperative factors, there were no differences in body mass index (BMI) or the proportion of patients with emaciation (BMI ≤17 kg/m²) between groups. However, the proportion of frail patients with malnutrition (albumin ≤3.5 g/dL) was significantly higher (6 cases, 22%) compared to 13 cases (7%) in the other groups. No differences were observed in operative time.
Within 30 days postoperatively, there was one surgical death (due to infection) in the frail group, with none in the pre-frail or robust groups. The postoperative hospital stay was significantly longer in the frail group compared to the robust group (median 17 days [range, 5–98] vs. 9 days [range, 5–52], respectively; P<0.001). Postoperative complications—such as ileus, pneumonia, and surgical site infection—occurred in 15 frail patients (56%), significantly higher than the 46 cases (26%) observed in the other two groups combined (P=0.002) (Table 2). The number of frail, pre-frail, and robust patients by cancer site is shown in Table 3.
A high complication rate in the frail group was observed after esophagectomy (5 cases, 63%), pancreatectomy (5 cases, 100%), and colectomy (3 cases, 75%) (Table 3). Among these, the most common complications after esophagectomy were pneumonia, recurrent laryngeal nerve paralysis, and surgical site infection. Pancreatic fistula was most frequently observed after pancreatectomy (Table 4). In terms of severity, mild complications predominated in lower gastrointestinal cancer cases, and there were no grade III or higher complications in this category (Fig. 4A). When comparing severity by group, there was one grade V case in the frail group. In this group, the highest proportion of complications was grade II, and there were no differences in the rates of grade II or III complications between frail, pre-frail, and robust groups (Fig. 4B).
Univariate and multivariate analyses revealed that age ≥65 years (P=0.039), frailty (P=0.046), and pancreatic cancer (P=0.011) were significantly associated with an increased risk of postoperative complications (Table 5).
Discussion
Among the 201 analyzed cases, upper gastrointestinal cancers comprised 34%, hepatobiliary and pancreatic cancers 25%, and lower gastrointestinal cancers 41%. Frailty, as defined by J-CHS criteria, affected 13% of cases, with 81% of frail patients aged 65 years or older. Frailty was more common in females (20%) than in males (10%). Frail patients exhibited higher rates of malnutrition and postoperative complications (56% in frail vs. 26% in non-frail), and experienced longer hospital stays (17 days vs. 9 days). Age, frailty, and pancreatic cancer were all independent risk factors for postoperative complications.
In this study, as in previous reports, frailty was highly prevalent among older adult patients; however, a notable number of frail cases were also observed among patients under 65 years of age. Furthermore, frailty was frequently identified in patients with esophageal cancer and was shown to be an independent risk factor for postoperative complications across all types of gastrointestinal cancer. Previous studies have similarly reported that frailty, as assessed by the Geriatric 8 screening tool, predicts both overall survival and cancer-specific survival following gastrointestinal cancer surgery. It has also been identified as an independent prognostic factor for recurrence and mortality after curative surgery for stage I–III colorectal cancer [10,11].
With the growing adoption of minimally invasive surgery, some studies have demonstrated that, in frail patients, the 30-day mortality rate after laparoscopic colorectal cancer surgery is lower than that after open surgery, likely due to reduced invasiveness [12]. However, studies not limited to cancer surgery have reported that frailty remains a substantial risk factor regardless of the surgical approach, and that even minimally invasive procedures are associated with high mortality rates in frail patients [13]. Notably, while laparoscopic and robot-assisted operations are generally considered to result in fewer postoperative complications than open surgery, some reports indicate that, in frail colorectal cancer patients, robot-assisted surgery is actually associated with a higher incidence of postoperative complications compared to laparoscopic or open surgery [14]. In the present study, we did not observe a significant association between the type of surgical procedure and the incidence of mortality or complications among frail patients. Nevertheless, these findings suggest that surgical procedure selection in frail patients should be approached with greater caution than in robust patients.
In Japan, where the population is rapidly aging, there is increasing interest in the relationship between frailty and cancer treatment. In 2021, as part of a Ministry of Health, Labour and Welfare research project on the development of guidelines for older adult cancer care, the Japanese Society of Coloproctology established clinical guidelines for the evaluation, treatment, and care of pre-frail older adult colorectal cancer patients [15-22]. Frailty and pre-frailty significantly impact postoperative prognosis, complication rates, and mortality in gastrointestinal cancer, underscoring the importance of identifying frail patients and providing appropriate interventions before surgery.
In our study, postoperative hospital stay was significantly longer in frail patients compared to robust patients. Esophageal cancer, known for being the most invasive among gastrointestinal surgeries and for having the highest rate of postoperative complications, had a median hospital stay of 14 days (range, 6–58 days), and accounted for 29% of frail cases. However, even after excluding esophageal cancer cases, postoperative hospital stays remained significantly longer in frail patients (median, 17 days; range, 5–98 days) compared to robust patients (median, 9 days; range, 5–52 days) (P=0.007). Further analysis revealed no correlation between frailty and markers of body constitution or malnutrition, such as albumin or BMI. Although various indices, including subjective evaluations, have been proposed for the assessment of frailty, it is essential that data be collected through objective preoperative physical function assessments. Our institution has initiated efforts to accumulate and share such data following preoperative evaluations, which led to the design of this preliminary study. The benefits of perioperative rehabilitation have been well documented, and for colorectal cancer, preoperative intervention has been shown to reduce postoperative complications compared to rehabilitation initiated only after surgery [23]. Thus, comprehensive interventions, including preventive rehabilitation before surgery and restorative rehabilitation, are required to improve postoperative physical function and assess motor function.
Nutritional intervention also plays a crucial role in the prevention and improvement of frailty. Frailty is closely associated with sarcopenia, cancer cachexia, and subsequent loss of muscle strength, all of which significantly affect prognosis. In this study, we also examined the provision of nutritional intervention among frail patients. Nutritional support team involvement was documented in 44% of frail cases, 30% of pre-frail cases, and 13% of robust cases, indicating that frail patients were more likely to receive nutritional support team support. Despite growing recognition of the risks associated with frailty in Japan, information essential for the identification and management of frailty is still not sufficiently shared among healthcare professionals. Improving postoperative outcomes for frail patients requires not only efforts by the primary department but also active multidisciplinary collaboration for identification, data sharing, and implementation of appropriate nutritional and rehabilitative interventions to restore muscle strength and facilitate effective information exchange. Notably, because a significant proportion of frail cases were also observed among younger cancer patients in this study, our findings suggest that frailty screening should not be limited to older adults.
This study had several limitations. First, its retrospective, single-center design may limit generalizability to other populations. Second, frailty assessment relied in part on subjective, self-reported measures, which could introduce reporting bias. Third, the relatively small sample size of frail patients may have restricted statistical power. Finally, we did not obtain long-term follow-up data, so the impact of frailty on long-term survival and functional outcomes could not be assessed.
In summary, our findings demonstrate that frailty is an independent risk factor for postoperative complications in patients undergoing gastrointestinal cancer resection. To improve surgical outcomes, it is essential to identify frailty through preoperative physical function assessment and to implement targeted interventions through multidisciplinary collaboration.
Authors’ contribution
Conceptualization: AY, JN. Data curation: AY, SI. Formal analysis: JN, AY. Investigation: SI. Methodology: AY, CM, NH. Project administration: HA, HW. Supervision: TO, MY, HT, HT, HM. Validation: JN. Visualization: AY. Writing–original draft: AY. Writing–review: JN, NH, CM, HA, HW, TO, MY, HT, HM, HT. All authors read and approved the final manuscript.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
We would like to express our sincere gratitude to all the members of the Research Institute of Osaka International Cancer Center for their cooperation in conducting this study. We would also like to take this opportunity to thank everyone who supported us.
Supplementary materials
None.
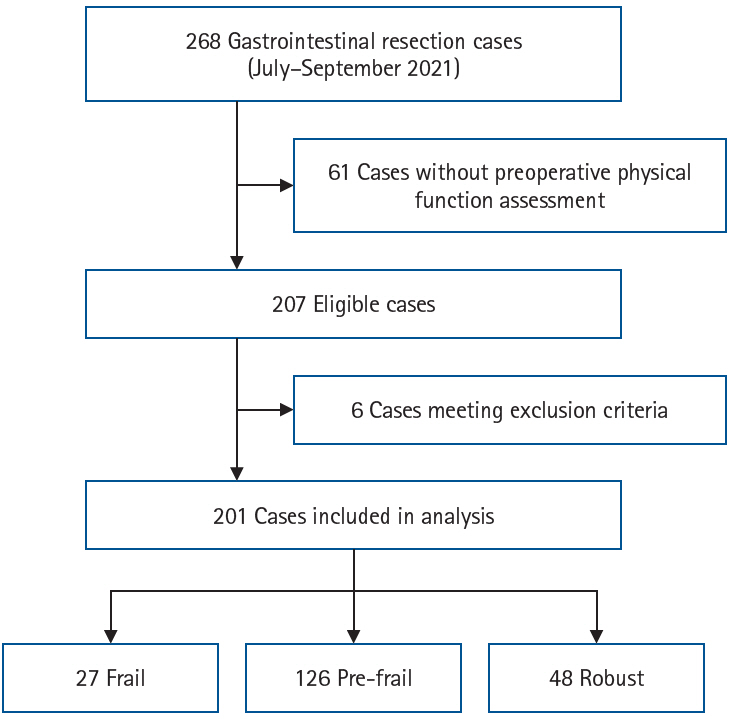
Fig. 2.
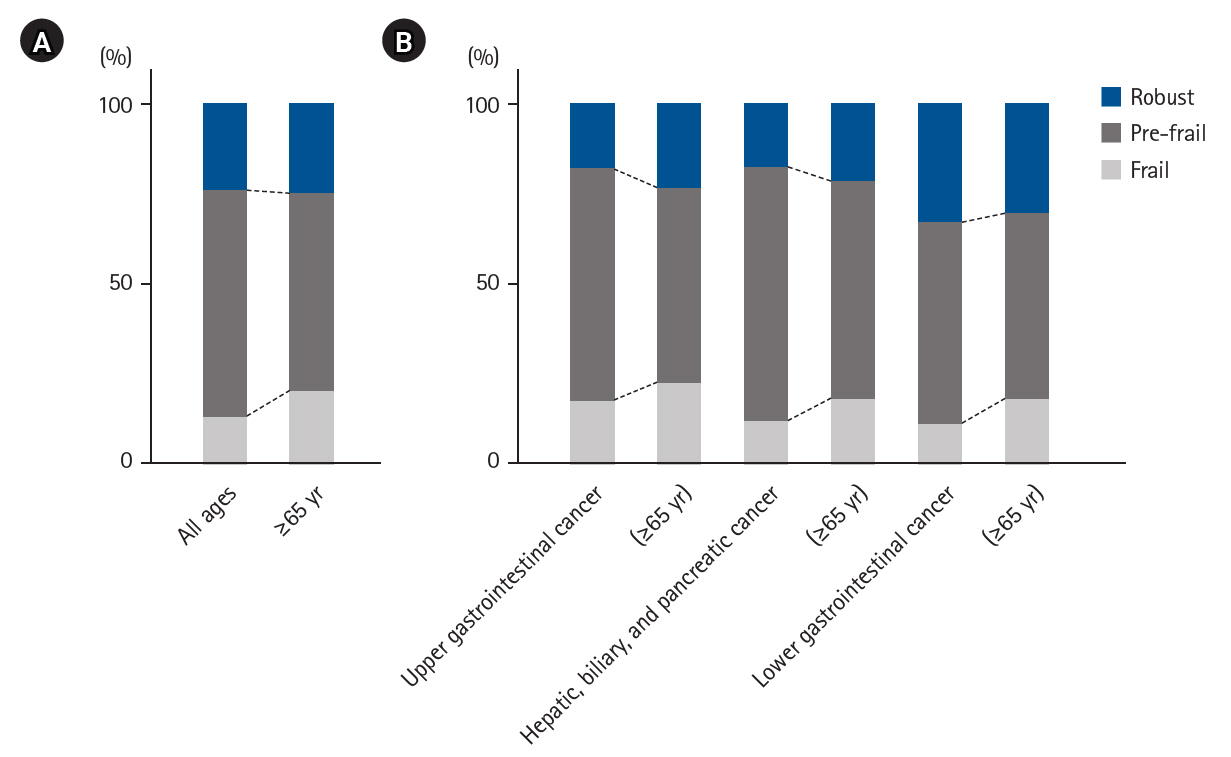
Prevalence of frailty status. (A) Proportions of each group among all patients and those aged ≥65 years. (B) Proportions of each group according to cancer site, overall and among patients aged ≥65 years.
Fig. 3.
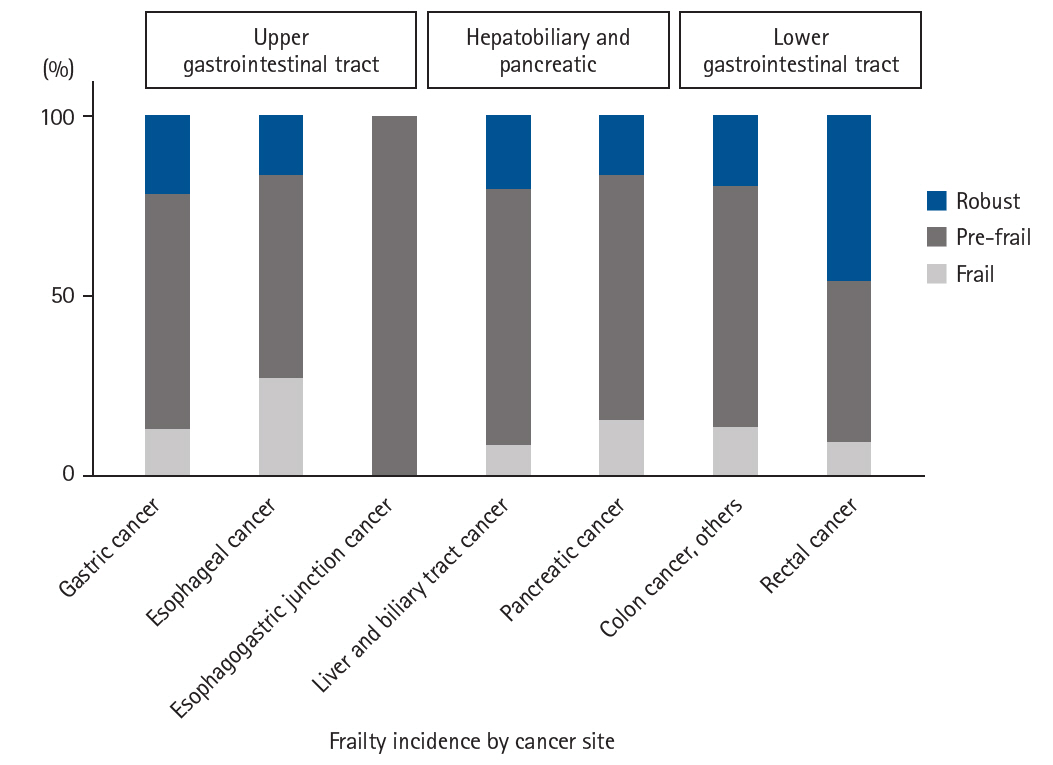
Proportion of each group by cancer site. Frailty, pre-frailty, and robust proportions in upper gastrointestinal, hepatobiliary-pancreatic, and lower gastrointestinal cancers.
Fig. 4.
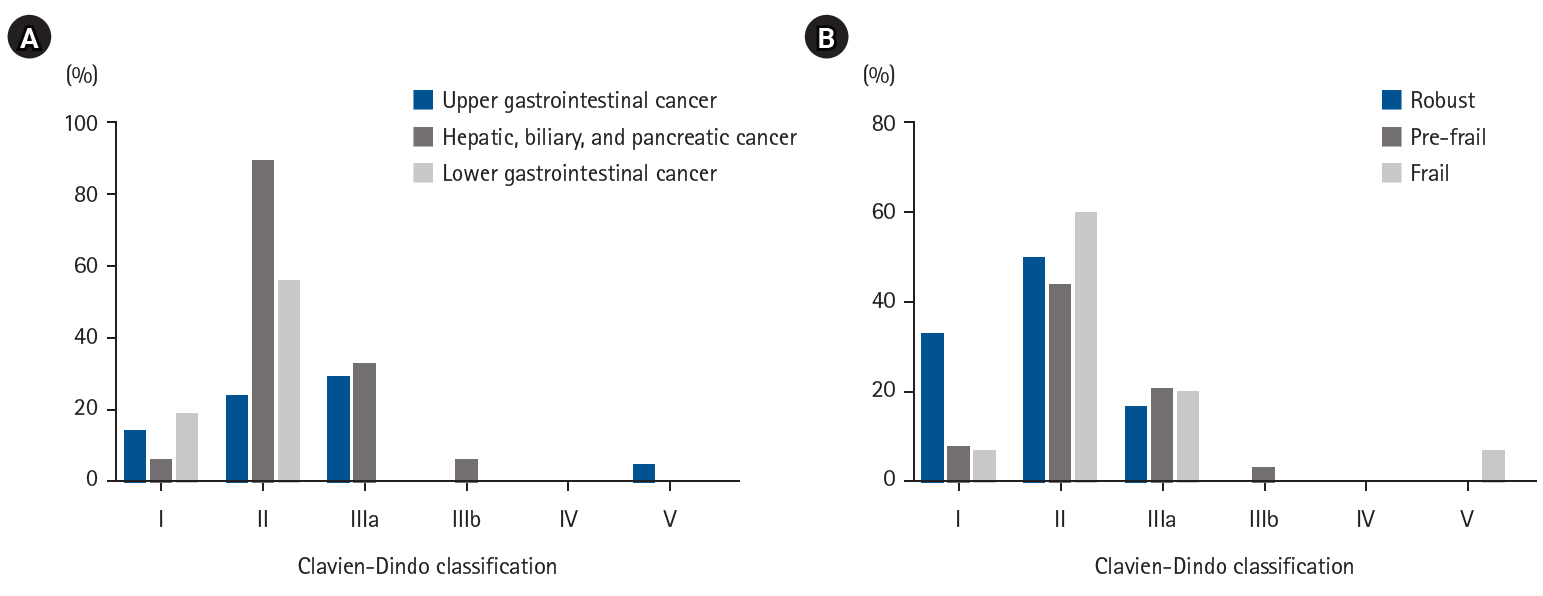
Clavien-Dindo classification of complications. Proportion of each grade in the Clavien-Dindo classification among the number of complications that occurred, by cancer site (A) and by group (B).
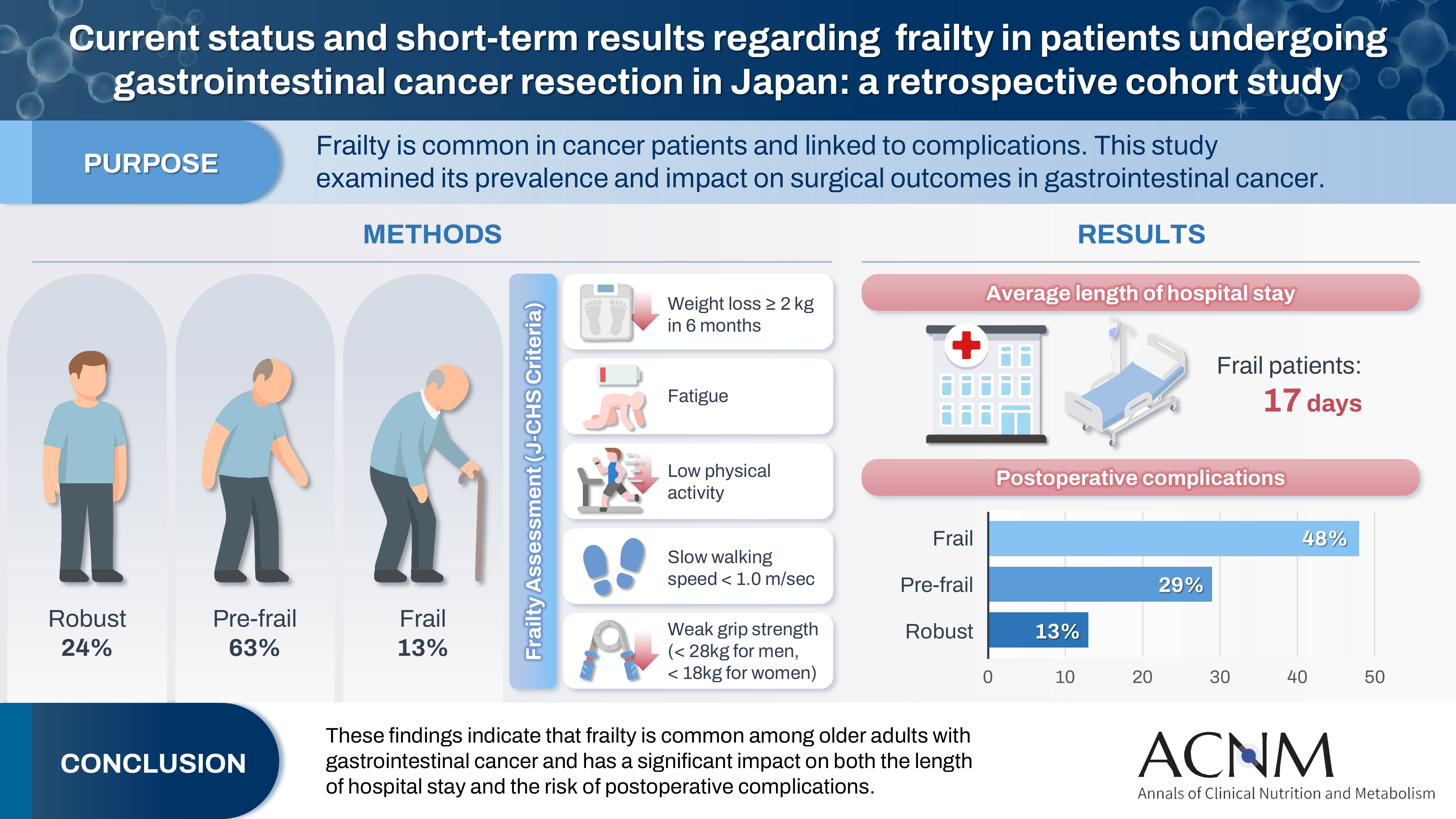
Table 1.
Patient background (n=201)
Table 2.
Patient characteristics by group during perioperative period
Table 3.
Number and proportion of postoperative complications by cancer site and group
Table 4.
Breakdown of number of complications by cancer site
Table 5.
Univariate and multivariate analyses of risk factors for postoperative complications
- 1. Arai H. Statement from the Japan Geriatrics Society on Frailty 2014. Nihon Ronen Igakkai Zasshi 2016;53:11.
- 2. Cancer and Disease Control Division, Health Bureau, Ministry of Health, Labour and Welfare. National Cancer Registry: Incidence and Rate Report; 2019.
- 3. Hasegawa H, Takahashi A, Kakeji Y, Ueno H, Eguchi S, Endo I, et al. Surgical outcomes of gastroenterological surgery in Japan: Report of the National Clinical Database 2011-2017. Ann Gastroenterol Surg 2019;3:426-50. ArticlePubMedPMCPDF
- 4. Vacante M, Cristaldi E, Basile F, Borzi AM, Biondi A. Surgical approach and geriatric evaluation for elderly patients with colorectal cancer. Updates Surg 2019;71:411-7. ArticlePubMedPDF
- 5. Jin L, Inoue N, Sato N, Matsumoto S, Kanno H, Hashimoto Y, et al. Comparison between surgical outcomes of colorectal cancer in younger and elderly patients. World J Gastroenterol 2011;17:1642-8. ArticlePubMedPMC
- 6. Chen SY, Stem M, Cerullo M, Gearhart SL, Safar B, Fang SH, et al. The effect of frailty index on early outcomes after combined colorectal and liver resections. J Gastrointest Surg 2018;22:640-9. ArticlePubMedPDF
- 7. Indrakusuma R, Dunker MS, Peetoom JJ, Schreurs WH. Evaluation of preoperative geriatric assessment of elderly patients with colorectal carcinoma: a retrospective study. Eur J Surg Oncol 2015;41:21-7. ArticlePubMed
- 8. Satake S, Arai H. The revised Japanese version of the Cardiovascular Health Study criteria (revised J-CHS criteria). Geriatr Gerontol Int 2020;20:992-3. PubMed
- 9. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205-13. PubMedPMC
- 10. Ono R, Makiura D, Nakamura T, Okumura M, Fukuta A, Saito T, et al. Impact of preoperative social frailty on overall survival and cancer-specific survival among older patients with gastrointestinal cancer. J Am Med Dir Assoc 2021;22:1825-30. ArticlePubMed
- 11. Mima K, Miyanari N, Morito A, Yumoto S, Matsumoto T, Kosumi K, et al. Frailty is an independent risk factor for recurrence and mortality following curative resection of stage I-III colorectal cancer. Ann Gastroenterol Surg 2020;4:405-12. ArticlePubMedPMCPDF
- 12. Gietelink L, Wouters MW, Bemelman WA, Dekker JW, Tollenaar RA, Tanis PJ, et al. Reduced 30-day mortality after laparoscopic colorectal cancer surgery: a population based study from the Dutch Surgical Colorectal Audit (DSCA). Ann Surg 2016;264:135-40. PubMed
- 13. Shinall MC Jr, Arya S, Youk A, Varley P, Shah R, Massarweh NN, et al. Association of preoperative patient frailty and operative stress with postoperative mortality. JAMA Surg 2020;155:e194620.PubMedPMC
- 14. Lo BD, Leeds IL, Sundel MH, Gearhart S, Nisly GRC, Safar B, et al. Frailer patients undergoing robotic colectomies for colon cancer experience increased complication rates compared with open or laparoscopic approaches. Dis Colon Rectum 2020;63:588-97. ArticlePubMed
- 15. Murofushi K, Murakami Y, Makishima H, Moriwaki T, Sasaki T, Nakamura M, et al. Provisional clinical opinions for radiation therapy in prefrail elderly colorectal cancer patients: part two. J Jpn Soc Coloproctol 2021;74:422-29. Article
- 16. Murofushi K, Murakami Y, Makishima H, Moriwaki T, Sasaki T, Nakamura M, et al. Provisional clinical opinions for radiation therapy in prefrail elderly colorectal cancer patients: part one. J Jpn Soc Coloproctol 2021;74:413-21. Article
- 17. Mizuno I, Matsuda K, Oka S, Nishimura J, Murata K, Tanaka C, et al. Clinical recommendations for pre-frail elderly colorectal cancer patients: Clinical question—What is the appropriate anesthesia method for elderly colorectal cancer patients? Program and Abstracts of the 33rd Annual Meeting of the Japanese Society of Geriatric Anesthesiology (online meeting): 42, 2021.
- 18. Tanaka C, Mizuno I, Nishimura J, Matsuda K, Murata K, Oka S, et al. Provisional clinical opinions (PCOs) recommended by the Surgical Treatment Working Group for vulnerable elderly patients in colorectal cancer: general remarks on surgical treatment. J Jpn Soc Coloproctol 2021;74:391-400. Article
- 19. Tamura K, Karasawa K, Yamamoto H, Ogawa T, Umihori M, Watanabe K, et al. provisional clinical opinions (PCO) recommended by the Overview and Geriatric Assessment Working Group for vulnerable elderly patients in colorectal cancer: Part 2. J Jpn Soc Coloproctol 2021;74:276-86. Article
- 20. Tamura K, Karasawa K, Yamamoto H, Ogawa T, Umihori M, Watanabe K, et al. Provisional clinical opinions (PCO) Recommended by the Overview and Geriatric Assessment Working Group for vulnerable elderly patients in colorectal cancer: Part 1. J Jpn Soc Coloproctol 2021;74:269-75. Article
- 21. Ishiguro H, Ishibashi H, Yamaguchi T, Watanuki S, Hanai A, Sakurai N, et al. Provisional clinical opinions recommended by the Supportive and Palliative Care Working Group for vulnerable elderly patients with colorectal cancer. J Jpn Soc Coloproctol 2021;74:349-56. Article
- 22. Nishimura J, Yoshida Y, Tanaka C, Matsuda K, Oka S, Murata K, et al. Provisional clinical opinions (PCOs) recommended by the Surgical Treatment Working Group for vulnerable elderly patients in colorectal cancer: clinical questions with answers. J Jpn Soc Coloproctol 2021;74:401-12. Article
- 23. Fujii S, Hashimoto Y, Sakata M, Yoshimizu N, Shimamura K, Deguchi T, et al. Impact of preoperative rehabilitation interventions on perioperative outcomes in frail patients with colorectal cancer. J Jpn Soc Coloproctol 2022;75:114-23. Article
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
Cite- Figure
-
- Related articles
-
- Association between the calcium-to-phosphorus ratio and early hypophosphatemia in preterm infants receiving parenteral nutrition in Korea: a retrospective cohort study
- The enteral feeding tube access route in esophageal cancer surgery in Japan: a retrospective cohort study
- Perioperative outcomes of older adult patients with pancreatic cancer based on nutritional status: a retrospective cohort study
Current status and short-term results regarding frailty in patients undergoing gastrointestinal cancer resection in Japan: a retrospective cohort study
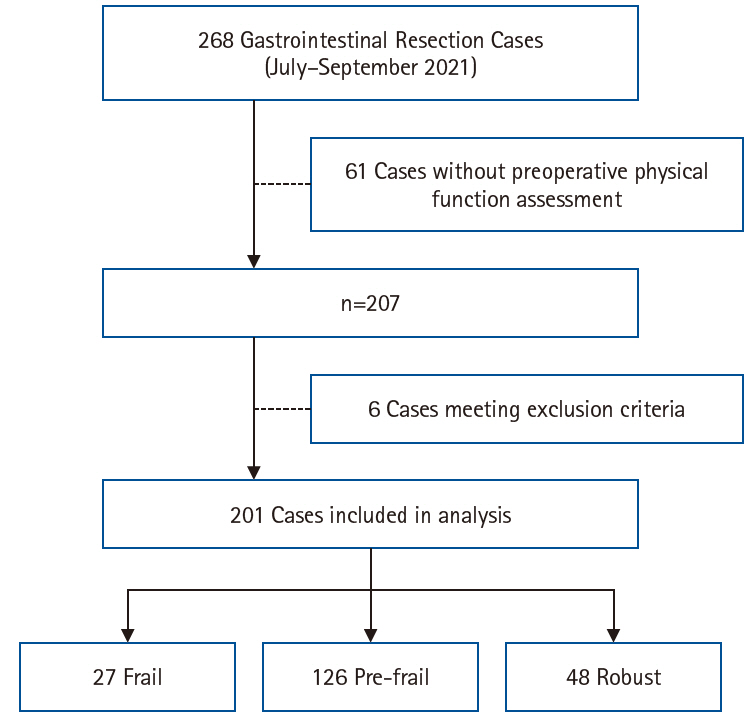
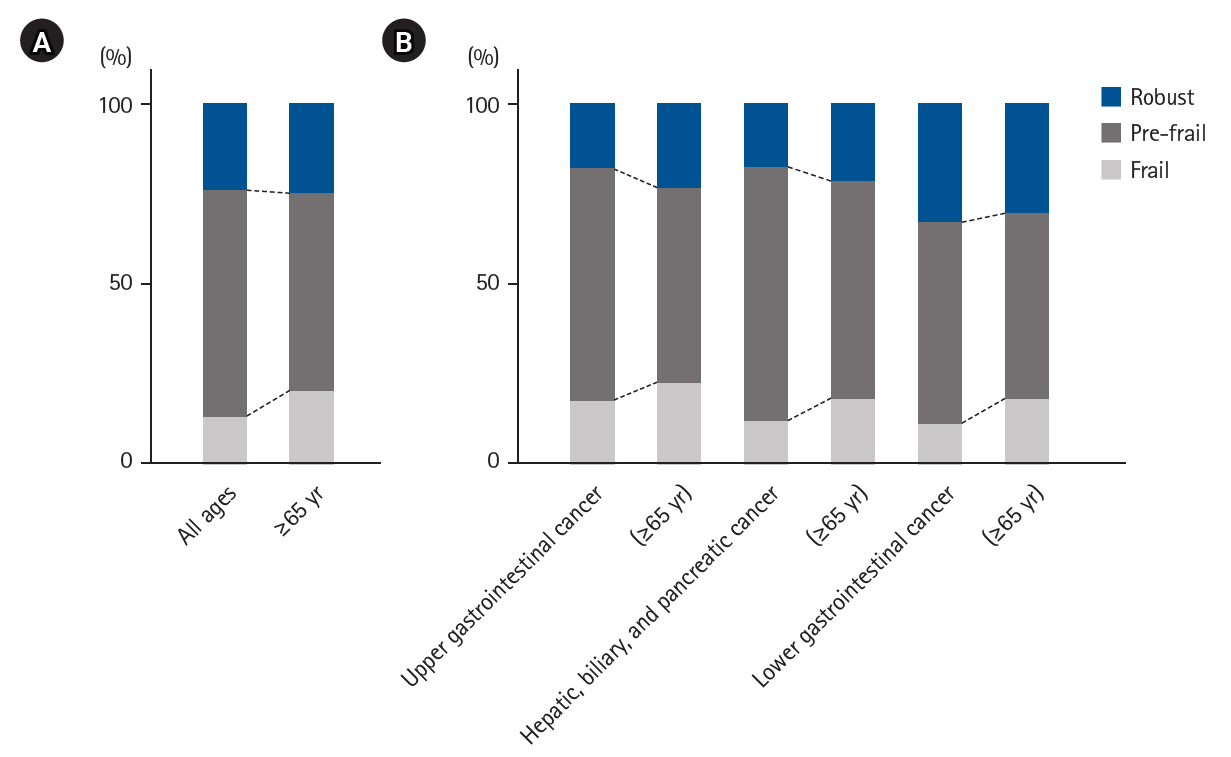
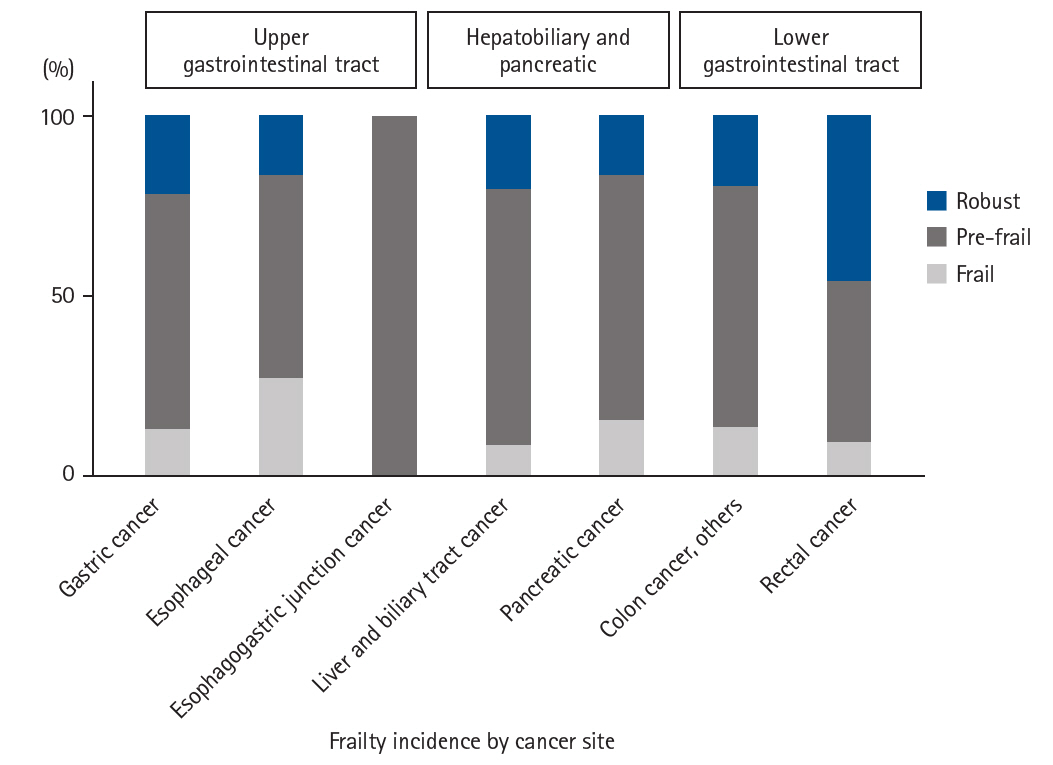
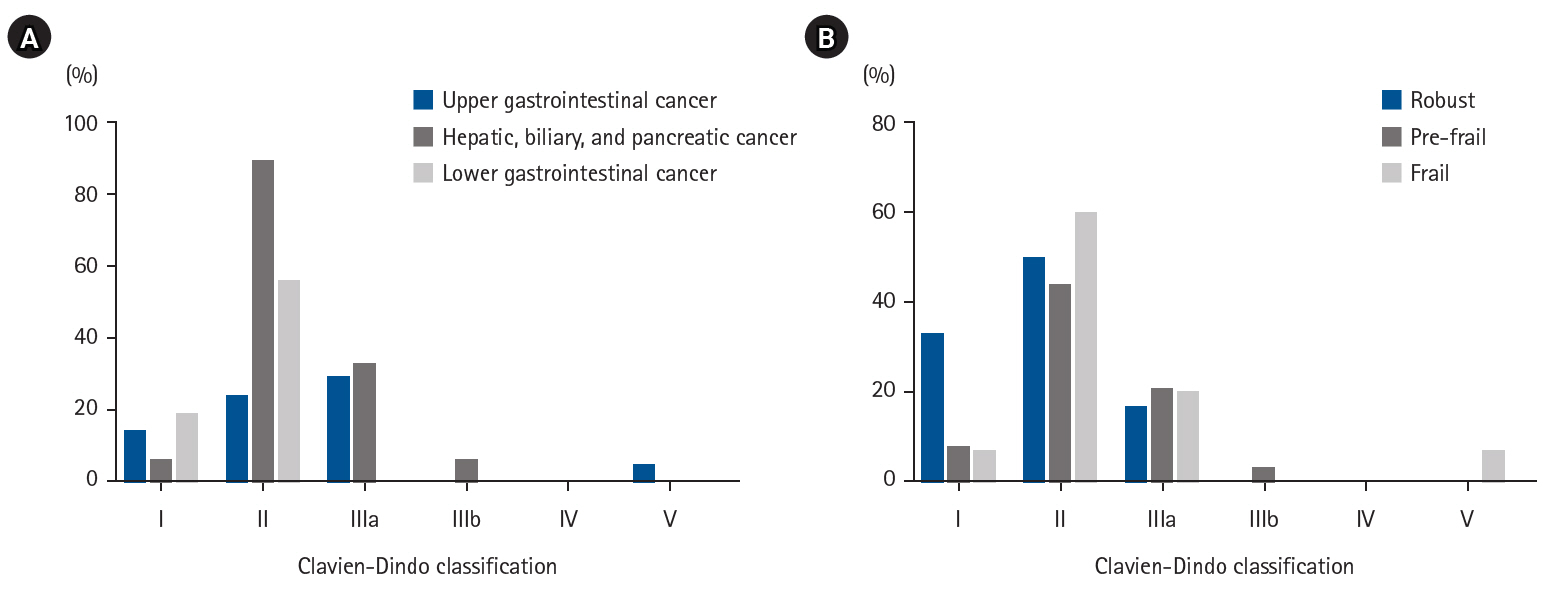
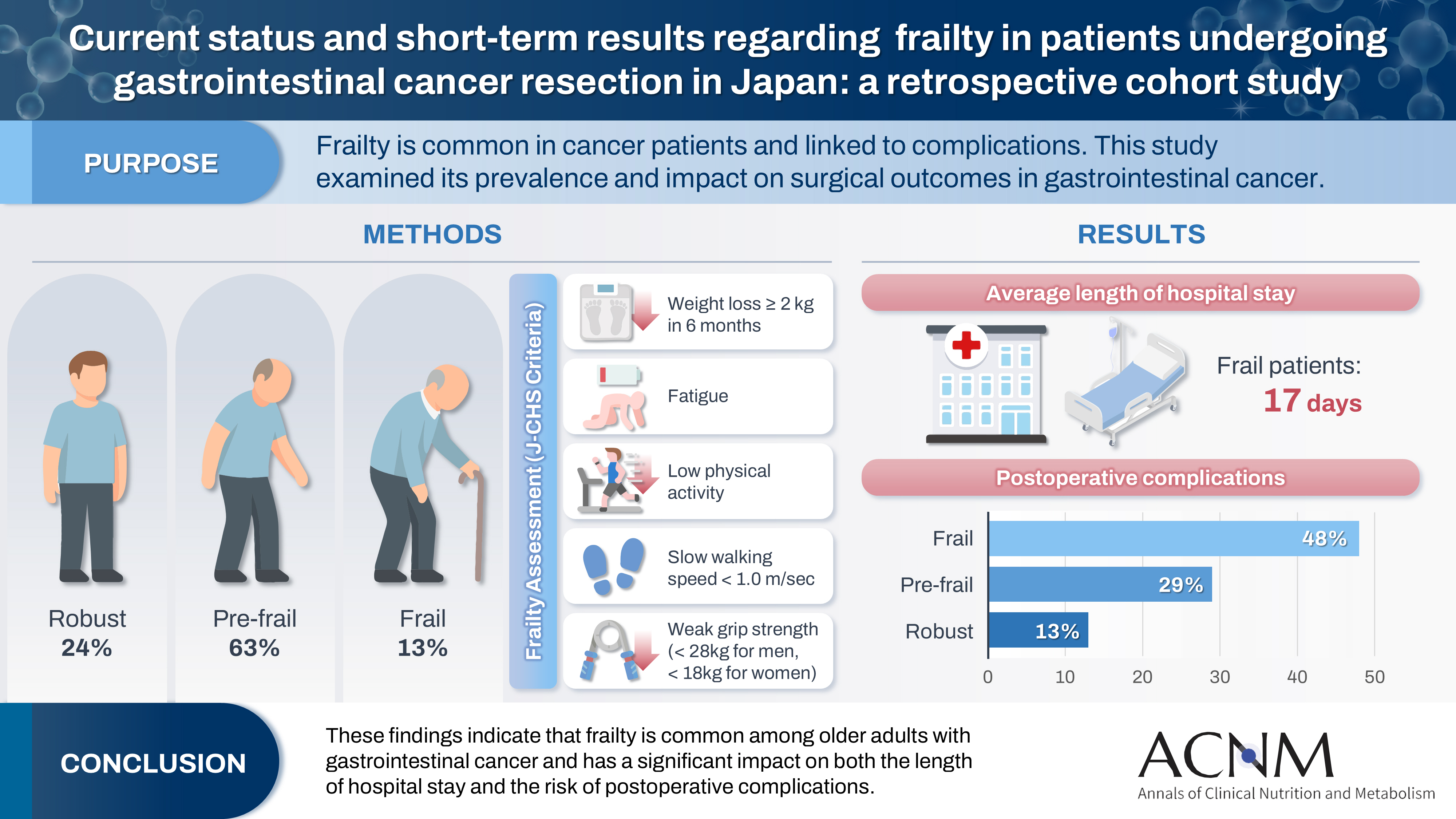
Fig. 1. Flowchart for frailty assessment.
Fig. 2. Prevalence of frailty status. (A) Proportions of each group among all patients and those aged ≥65 years. (B) Proportions of each group according to cancer site, overall and among patients aged ≥65 years.
Fig. 3. Proportion of each group by cancer site. Frailty, pre-frailty, and robust proportions in upper gastrointestinal, hepatobiliary-pancreatic, and lower gastrointestinal cancers.
Fig. 4. Clavien-Dindo classification of complications. Proportion of each grade in the Clavien-Dindo classification among the number of complications that occurred, by cancer site (A) and by group (B).
Graphical abstract
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Graphical abstract
Current status and short-term results regarding frailty in patients undergoing gastrointestinal cancer resection in Japan: a retrospective cohort study
| Variable | Value |
|---|---|
| Sex | |
| Male | 131 (65) |
| Female | 70 (35) |
| At surgery age (yr) | 67 (28–86) |
| ≥65 yr | 112 (55) |
| Preoperative BMI (kg/m2) | 22.2 (14.1–31.6) |
| Emaciation (BMI <17 kg/m2) | 9 (4) |
| Upper GI tract | 68 (34) |
| Gastric cancer | 32 (47) |
| Esophageal cancer | 30 (44) |
| Esophagogastric junction cancer | 6 (9) |
| Hepato-biliary-pancreatic | 51 (25) |
| Liver, biliary tract cancer | 25 (49) |
| Pancreatic cancer | 26 (51) |
| Lower GI tract | 82 (41) |
| Colon cancer | 38 (46) |
| Rectal cancer | 44 (54) |
| Factor | Frail (n=27) | Pre-frail (n=126) | Robust (n=48) |
|---|---|---|---|
| Preoperative factors | |||
| Sex | |||
| Male | 13 (48) | 81 (64) | 37 (77) |
| Female | 14 (52)* | 45 (36) | 11 (33) |
| Age at surgery (≥65 yr) | 22 (81)* | 62 (49) | 28 (58) |
| Preoperative BMI (kg/m²) | 20.3 (14.1–31.1) | 22.35 (14.3–31.6) | 22.35 (18.5–31.6) |
| Emaciation (BMI <17 kg/m²) | 1 (4) | 8 (6) | 0 |
| Malnutrition (albumin <3.5 g/dL) | 6 (22)* | 11 (9) | 2 (4) |
| Intraoperative factors | |||
| Operation time (min) | 379 (167–719) | 299 (35–936) | 297 (102–687) |
| Laparoscopic surgery | 17 (63) | 74 (58) | 28 (58) |
| Robot-assisted surgery | 3 (11) | 30 (24) | 13 (27) |
| Open surgery | 7 (26) | 22 (17) | 7 (15) |
| Length of hospital stay | 17 (5–98)* | 10 (4–74) | 9 (5–52) |
| Postoperative BMI (kg/m2) | 20.3 (14.2–27.8) | 21.1 (14.5–31.9) | 21.8 (17.2–29.2) |
| Postoperative death (within 30 day) | 1 (4) | 0 | 0 |
| Postoperative complications | 15 (56)* | 40 (32) | 6 (13) |
| Cancer site/subtype | Frail | Pre-frail | Robust |
|---|---|---|---|
| Upper GI tract | |||
| Gastric cancer | 4 | 21 | 7 |
| Complications (%) | 0 | 2 (10) | 0 |
| Esophageal cancer | 8 | 17 | 5 |
| Complications (%) | 5 (63) | 9 (53) | 1 (20) |
| Esophagogastric junction cancer | 0 | 6 | 0 |
| Complications (%) | 0 | 1 (17) | 0 |
| Hepato-biliary-pancreatic | |||
| Liver, biliary tract cancer | 2 | 18 | 5 |
| Complications (%) | 1 (50) | 8 (44) | 1 (20) |
| Pancreatic cancer | 4 | 18 | 4 |
| Complications (%) | 5 (100) | 9 (50) | 1 (25) |
| Lower GI tract | |||
| Colon cancer, others | 5 | 26 | 7 |
| Complications (%) | 1 (20) | 7 (27) | 1 (14) |
| Rectal cancer | 4 | 20 | 2 |
| Complications (%) | 3 (75) | 4 (20) | 2 (10) |
| Obstructive ileus | Ureteral injury | Postoperative bleeding | Surgical site infection | Pneumonia | Recurrent laryngeal nerve palsy | Pleural effusion | Cholecystitis | Pancreatic fistula | Delayed gastric emptying | Others | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gastric cancer | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| Esophageal cancer | 0 | 0 | 0 | 3 | 4 | 4 | 1 | 0 | 0 | 0 | 4 |
| Esophagogastric junction cancer | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Liver, biliary tract cancer | 0 | 0 | 1 | 2 | 1 | 0 | 0 | 3 | 2 | 0 | 1 |
| Pancreatic cancer | 1 | 0 | 2 | 1 | 0 | 0 | 0 | 2 | 4 | 2 | 3 |
| Colon cancer, others | 2 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 3 |
| Rectal cancer | 2 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 4 |
| Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P-value | RR | 95% CI | P-value | |
| Sex (male/female) | 1.27 | 0.663–2.518 | 0.471 | |||
| Age (≥65 yr/<65 yr) | 2.741 | 1.418–5.523 | 0.002* | 2.252 | 1.121–4.682 | 0.039* |
| Frailty (frail/pre-frail, robust) | 2.918 | 1.261–6.738 | 0.013* | 2.482 | 1.013–6.042 | 0.046* |
| Cancer site | ||||||
| Gastric cancer | 0.078 | 0.004–0.381 | <0.001 | |||
| Esophageal cancer | 1.925 | 0.889–4.080 | 0.096 | |||
| Esophagogastric junction cancer | 1.300 | 0.060–13.830 | 0.834 | |||
| Liver, biliary tract cancer | 1.037 | 0.383–2.546 | 0.939 | |||
| Pancreatic cancer | 4.602 | 1.973–11.061 | <0.001* | 3.173 | 1.294–7.983 | 0.011* |
| Colon cancer, others | 1.611 | 0.743–3.809 | 0.234 | |||
| Rectal cancer | 1.267 | 0.575–3.025 | 0.568 | |||
Table 1. Patient background (n=201)
Values are presented as number (%) or median (range). BMI, body mass index; GI, gastrointestinal.
Table 2. Patient characteristics by group during perioperative period
Values are presented as number (%) or median (range). Fisher exact test was used for comparison of numbers of cases; Dunnett’s test was used for body mass index (BMI), operation time, and hospital stay, with the robust group as control. *P<0.05
Table 3. Number and proportion of postoperative complications by cancer site and group
Cases with multiple complications are included.
Table 4. Breakdown of number of complications by cancer site
Number of postoperative complications according to Japan Clinical Oncology Group Clavien-Dindo classification v.2.0. Cases with multiple complications are included.
Table 5. Univariate and multivariate analyses of risk factors for postoperative complications
OR, odds ratio; CI, confidence interval; RR, relative risk. Logistic regression was used for the analysis of risk factors for postoperative complications. *P<0.05.

