 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Search
- Page Path
- HOME > Search
Original Article
- Epigallocatechin gallate increases fatty acid oxidation but not 24-hour survival in lipopolysaccharide-induced endotoxic shock in mice
-
Takayuki Irahara
 , Ryusuke Katsuki, Dai Oishi, Tsuguaki Terashima, Md. Monirul Islam
, Ryusuke Katsuki, Dai Oishi, Tsuguaki Terashima, Md. Monirul Islam , Umme Salma, Shohag Majumder, Ridwan Ahmed, Eizo Watanabe
, Umme Salma, Shohag Majumder, Ridwan Ahmed, Eizo Watanabe - Ann Clin Nutr Metab 2026;18(1):27-33. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0036
-
 Graphical Abstract
Graphical Abstract
 Abstract
Abstract
 PDF
PDF - Purpose
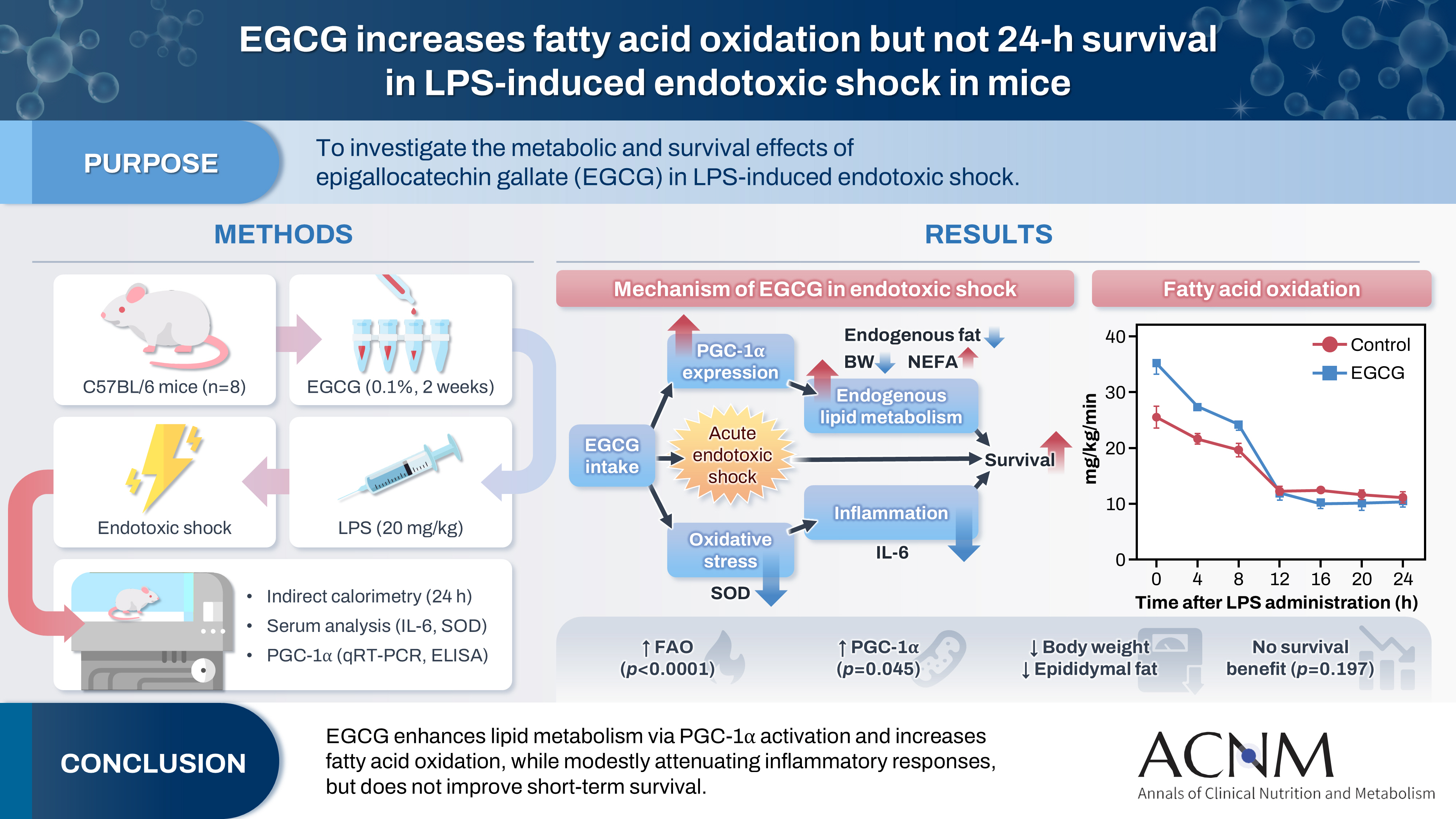
This study aimed to explore the effects of epigallocatechin gallate (EGCG) in critically ill patients using a mouse model.
Methods
C57BL/6 mice were divided into control and EGCG groups (n=8 per group). The EGCG group received a 0.1% EGCG solution for 2 weeks, after which the mice were intraperitoneally injected with a lethal dose of lipopolysaccharide to induce acute endotoxic shock. Indirect calorimetry was performed for 24 hours. Changes in body weight, epididymal fat weight, and survival were measured, together with serum lipid levels, interleukin-6 (IL-6), and superoxide dismutase (SOD) concentrations. The expression of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α) was determined using quantitative real-time polymerase chain reaction, and its serum concentration was subsequently measured.
Results
Indirect calorimetry showed a significant increase in fatty acid oxidation (P<0.0001) in the EGCG group, along with significant decreases in body weight and epididymal fat weight (P<0.01 and P<0.05, respectively). Survival did not differ significantly between groups (P=0.197). Serum lipid levels, IL-6, and SOD showed numerical differences, although these differences were not statistically significant. Furthermore, hepatic PGC-1α expression showed a tendency toward upregulation, and serum PGC-1α levels were significantly higher (P<0.05).
Conclusion
EGCG stimulates endogenous lipid metabolism through PGC-1α activation and may suppress inflammatory responses; therefore, it may represent a potentially useful nutrient for acute nutritional therapy.
- 3,012 View
- 36 Download

Review
- Recent advances in refeeding syndrome in critically ill patients: a narrative review
-
Sang Woo Ha
 , Suk-Kyung Hong
, Suk-Kyung Hong - Ann Clin Nutr Metab 2024;16(1):3-9. Published online April 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.1.3
-
Abstract
PDF
- Purpose: The aim of this article is to provide a narrative review of the most recent studies on refeeding syndrome (RS) in critically ill patients and to summarize recent advancements that can be referenced in the treatment of these patients.
Current concept: RS in critically ill patients is a potentially lethal nutrition-related condition leading to sudden death. Initiation of food intake after a period of fasting can trigger rapid electrolyte uptake due to increased insulin release, leading to a decline in serum electrolytes with thiamine. This depletion may cause severe complications, such as cardiac arrhythmias, respiratory failure, seizures, and even death. The incidence of RS varies significantly, ranging from 7.4%–89%. Despite updates in diagnostic criteria over time, there remains a crucial need for criteria applicable to critically ill patients with underlying disorders such as metabolic derangement and organ dysfunction. To prevent RS, it is strongly recommended to start food intake after a fast at 20%–25% of estimated goals, gradually increasing the intake over several days. Close monitoring and electrolyte supplementation—especially of phosphorus, potassium, magnesium, and thiamine—are crucial, especially in critically ill patients. If electrolyte imbalances persist, slowing down or halting the progression of nutrition should be considered.
Conclusion: Clinicians should continue their efforts to promptly identify high-risk patients and to provide prevention and treatment for RS, particularly during the initiation of nutritional therapy in critically ill patients. Developing evidence-based protocols through further well-designed research is essential for effectively managing critically ill patients at risk of RS. -
Citations
Citations to this article as recorded by
- Actualización en terapia médica nutricional del paciente críticamente enfermo: avances, desafíos y evidencia reciente
Nestor David Caicedo-Buitrago, Mateo Londoño-Pereira, Claudia Milena Ardila Melendez, Ricardo Merchán, Fernando Pereira-Paternina, Cristian Pinilla, Sonia Gamboa, Alejandra Cabral, Janeth Barbosa Barbosa, Maria del Pilar Morales, Bladimir Gil
Acta Colombiana de Cuidado Intensivo.2026; : 100612. CrossRef - Refeeding Syndrome: A Comprehensive Review of Pathophysiology, Risk Stratification and Evidence-based Management in the Intensive Care Unit
Paras Chandrakant Zunke
Vidarbha Journal of Internal Medicine.2026; 35(1): 22. CrossRef - Nutrition in the critically ill in resource-limited settings/low- and middle-income countries
Mervyn Mer, Martin W. Dünser
Current Opinion in Clinical Nutrition & Metabolic Care.2025; 28(2): 181. CrossRef - Nutritional Management of Liver Failure in the Intensive Care Unit
Zsófia Verzár, Rudolf Kiss, Csaba Pál Bálint, Annamária Pakai, Tímea Csákvári
Medicina.2025; 61(7): 1210. CrossRef - Comprehensive care of the patient with Refeeding Syndrome
Magdalena Kwiatkowska, Dominika Krupnik, Fabian Wesołek, Agnieszka Jonczyk, Łukasz Krzych
Polish Journal of Surgery.2025; 97(5): 64. CrossRef
- Actualización en terapia médica nutricional del paciente críticamente enfermo: avances, desafíos y evidencia reciente
- 65,535 View
- 1,692 Download
- 5 Crossref
Review Article
- Muscle Protein Metabolism in Critically Illness
-
Min Chang Kang
- Surg Metab Nutr 2020;11(2):35-39. Published online December 30, 2020
- DOI: https://doi.org/10.18858/smn.2020.11.2.35
-
Abstract
PDF
- Most patients experience a considerable amount of muscle wasting during critical care. A decrease in muscle mass causes weakness which inevitably leads to delayed recovery. Since muscle also plays an important role in protein metabolism, metabolic instability increases as muscle mass decreases. Accordingly, various treatments have been attempted to maintain muscle mass and function in critically ill patients; however, it is still difficult to prevent muscle loss. It is known that muscle wasting in critical illness is primarily due to increased muscle protein breakdown rather than a decrease in muscle protein synthesis. Nutritional therapy and rehabilitation are fundamentally important, but additional anabolic agents may be needed to overcome anabolic resistance. In this review, we will learn about muscle protein metabolism in critically ill patients and how various treatments affect muscle protein metabolism.
-
Citations
Citations to this article as recorded by- Combined intravenous bolus amino acid supplementation and mobilization on early muscle loss in critically ill adults: A randomized controlled trial
Lizl Veldsman, Guy A. Richards, Daniel Nel, Tertius A. Kohn, Renée Blaauw
Journal of Parenteral and Enteral Nutrition.2026; 50(2): 170. CrossRef - Reply to “Mechanical tension and autophagy suppression: Unmasking the confounders in ICU muscle preservation strategies”
Lizl Veldsman, Guy A. Richards, Daniel Nel, Tertius A. Kohn, Renée Blaauw
Journal of Parenteral and Enteral Nutrition.2026; 50(5): 640. CrossRef - Low protein content of plant-derived nutrition limits the protein transition in hospitalized patients: Results from an observational study
M.A. van Bree, B.C. Schouten, E.S. Wolters, M.R. Soeters, H.M. Kruizenga
Clinical Nutrition ESPEN.2025; 69: 311. CrossRef - Combined Protein, Probiotics, and Exercise Therapy for Sarcopenia: A Comprehensive Review
Ryuk Jun Kwon, Mohammad Al Mijan, Soo Min Son, Wanho Yoo, Taehwa Kim
Cells.2025; 14(17): 1375. CrossRef - Double-Edge Effects of Leucine on Cancer Cells
Burkitkan Akbay, Zhannur Omarova, Alexander Trofimov, Bayan Sailike, Orynbassar Karapina, Ferdinand Molnár, Tursonjan Tokay
Biomolecules.2024; 14(11): 1401. CrossRef - Compartmental analysis: a new approach to estimate protein breakdown and meal response in health and critical illness
Nicolaas E. P. Deutz, Mariëlle P. K. J. Engelen
Frontiers in Nutrition.2024;[Epub] CrossRef - Amino acid kinetics in the critically ill
Nicolaas E.P. Deutz, Krista L. Haines, Paul E. Wischmeier, Mariëlle P.K.J. Engelen
Current Opinion in Clinical Nutrition & Metabolic Care.2024; 27(1): 61. CrossRef
- Combined intravenous bolus amino acid supplementation and mobilization on early muscle loss in critically ill adults: A randomized controlled trial
- 7,511 View
- 65 Download
- 7 Crossref
Original Articles
- Effect of Obesity on 30-Day Mortality in Critically Ill Surgical Patients
- Jung Yeob Ko, Yun Tae Jung, Jae Gil Lee
- J Clin Nutr 2018;10(2):51-55. Published online December 31, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.2.51
-
Abstract
PDF
Purpose:
This study was conducted to assess how extreme obesity affects 30-day mortality in this patient group.
Methods:
A total of 802 patients who underwent emergency gastrointestinal surgery from January 2007 to December 2017 were retrospectively reviewed. Patients were divided into three groups according to their body mass index (BMI): group 1, normal weight (BMI: 18.5∼22.9 kg/m2); group 2, overweight (BMI: 23.0∼29.9 kg/m2); and group 3, obesity (BMI≥30 kg/m2). Patients with a BMI under 18.5 were excluded from the analysis. Chi-squared test, Fisher’s exact test, Kaplan-Meier survival analysis, and the log-rank test were used to assess and compare 30-day mortality rates between groups.
Results:
The mortality rates of group 1, group 2, and group 3 were 11.3%, 9.0%, and 26.9%, respectively (P<0.017). The mortality rate did not differ significantly between group 1 and 2 (11.3% vs. 9.0%; P=0.341), but group 1 and 2 showed better survival rates than group 3 (11.3% vs. 26.9%; P=0.028, 9.0% vs. 26.9%; P=0.011). Kaplan-Meier survival analysis revealed that group 3 had higher mortality than the other two groups (P=0.001).
Conclusion:
Obesity (BMI≥30 kg/m2) was one of the risk factors influencing critically ill patients who underwent emergency surgery.
- 1,117 View
- 3 Download
- Clinical Outcomes of Nutritional Supply in Critically Ill Patients in the Prone Position
- Yeonju Lee, Hyung-Sook Kim, Hyungwook Namgung, Eun Sook Lee, Euni Lee, Young-Jae Cho, Yeon Joo Lee
- J Clin Nutr 2018;10(1):2-8. Published online June 30, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.1.2
-
Abstract
PDF
Purpose:
Enteral nutrition is recommended in critically ill patients. On the other hand, the recommendation of nutritional support is limited and often controversial in critically ill patients in the prone position. Therefore, this study evaluated the clinical outcomes of nutritional support in critically ill patients in the prone position.
Methods:
A retrospective evaluation of the electronic medical records was conducted, including adult patients who were in the medical intensive care unit (ICU) in the prone position in Seoul National University Bundang Hospital from May 1, 2015 to June 30, 2017. The patients’ characteristics, nutritional support status while they were in the prone position, mortality in ICU and during hospitalization, ICU length of stay, mechanical ventilation days, and complications, such as ventilator associated pneumonia (VAP) and vomiting were collected.
Results:
In total, 100 patients were included. Of these, 12 received enteral nutrition and parenteral nutrition and 88 received only parenteral nutrition. The groups were similar in terms of age, sex, number of comorbidity, weight, PaO2/FiO2, hours of prone position, Simplified Acute Physiology Score II (SAPS II), Acute Physiologic and Chronic Health Evaluation II (APACHE II) score, and Sequential Organ Failure Assessment (SOFA) score. No differences were observed in ICU mortality (75.0%
vs . 46.6%; P=0.065), hospital mortality (83.3%vs . 58.0%; P=0.081), ICU length of stay (22.2±14.6vs . 18.2±21.2; P=0.128) and mechanical ventilation days (19.3±14.8vs . 14.5±19.1; P=0.098). In addition, there were no differences in the possible complications of the prone position, such as VAP (8.3%vs . 4.5%; P=0.480) and vomiting (8.3%vs . 1.1%; P=0.227).Conclusion:
No significant differences in the clinical outcomes were observed. Further studies will be needed to confirm the way of nutrition support while in the prone position.
- 1,219 View
- 7 Download
- Clinical Application of Bioelectrical Impedance Analysis and its Phase Angle for Nutritional Assessment of Critically III Patients
- Hyung-Sook Kim, Eun Sook Lee, Yeon Joo Lee, Jae Ho Lee, Choon-Taek Lee, Young-Jae Cho
- J Clin Nutr 2015;7(2):54-61. Published online August 31, 2015
- DOI: https://doi.org/10.15747/jcn.2015.7.2.54
-
Abstract
PDF
Purpose:
Phase angle (PA) is objectively determined from resistance and reactance measured by bioelectrical impedance analysis (BIA)−a quick, noninvasive method. The aim of this study was to evaluate the clinical application of PA by BIA for nutritional assessment of critically ill patients.
Methods:
Eighty nine adult patients admitted to a medical intensive care unit (ICU) of a tertiary academic hospital from August 2012 to September 2013 were analyzed. PA values were measured by direct segmental multi-frequency BIA. As traditional nutrition assessment tools, body mass index (BMI), serum albumin levels, total lymphocyte counts, and our hospital’s nutrition screening index (NSI) were also recorded. Correlations between the results of BIA and other traditional parameters were analyzed.
Results:
PA showed correlation with traditional nutritional parameters, including BMI (r=0.479), serum albumin (r=0.347), and NSI score (r=0.483). Patients with PA lower than the median value (3.5°) had significantly lower nutritional status, increased duration of mechanical ventilation (P=0.039), and increased length of ICU stay (P=0.041).
Conclusion:
PA, as a reflection of body cell mass, measured by BIA could be a potentially useful parameter for nutritional assessment in critically ill patients.
-
Citations
Citations to this article as recorded by- Optimal Enteral Nutrition Support Preserved Muscle Mass in Critically Ill Children
Kantisa Sirianansopa, Chavisa Rassameehirun, Sirinuch Chomtho, Orapa Suteerojntrakool, Lalida Kongkiattikul, Eric Gumpricht
Journal of Nutrition and Metabolism.2022; 2022: 1. CrossRef - Prognostic value of phase angle and bioelectrical impedance vector in critically ill patients: A systematic review and meta-analysis of observational studies
Júlia Lima, Igor Eckert, Maria Cristina Gonzalez, Flávia Moraes Silva
Clinical Nutrition.2022; 41(12): 2801. CrossRef - Bioelectrical Impedance Analysis for Prediction of Early Complications after Gastrectomy in Elderly Patients with Gastric Cancer: the Phase Angle Measured Using Bioelectrical Impedance Analysis
Byunghyuk Yu, Ki Bum Park, Ji Yeon Park, Seung Soo Lee, Oh Kyoung Kwon, Ho Young Chung
Journal of Gastric Cancer.2019; 19(3): 278. CrossRef
- Optimal Enteral Nutrition Support Preserved Muscle Mass in Critically Ill Children
- 4,758 View
- 22 Download
- 3 Crossref
 First
First Prev
Prev

