 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Search
- Page Path
- HOME > Search
Guideline
- The 2024 Korean Enhanced Recovery After Surgery guidelines for hepatobiliary and pancreatic surgery
-
Kwangpyo Hong
 , Hongbeom Kim, Hyung Sun Kim, Hae Won Lee, Ho Joong Choi, YoungRok Choi, Jae Do Yang, Sung-Moon Jeong, Dae Wook Hwang, Do Joong Park, Sang-Jae Park, The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition
, Hongbeom Kim, Hyung Sun Kim, Hae Won Lee, Ho Joong Choi, YoungRok Choi, Jae Do Yang, Sung-Moon Jeong, Dae Wook Hwang, Do Joong Park, Sang-Jae Park, The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition - Ann Clin Nutr Metab 2025;17(3):172-180. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0034
-
 Abstract
Abstract
 PDF
PDF - Purpose
The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition has developed comprehensive guidelines for hepatobiliary and pancreatic (HBP) surgery by adapting established international protocols. These guidelines provide evidence-based recommendations specifically tailored to the Korean healthcare system and address perioperative management for both pancreatoduodenectomy and hepatectomy.
Methods
The HBP subcommittee reviewed existing international ERAS guidelines and conducted an adaptation process. Key questions were identified based on national survey results from Korean HBP surgeons and were prioritized according to clinical relevance. The committee focused on elements supported by moderate- to high-quality evidence with strong recommendation grades. Literature searches were conducted through January 2025, and evidence quality was evaluated using GRADE methodology. Four key questions underwent formal assessment, and eight additional questions were adapted from international guidelines.
Results
Twelve key questions were selected and addressed, covering critical perioperative care domains: prehabilitation, preoperative nutritional assessment and support, anti-thrombotic prophylaxis, prophylactic abdominal drainage, preoperative biliary drainage, smoking and alcohol cessation, pre-anesthetic medication, minimally invasive surgical approaches, prophylactic nasogastric intubation, postoperative glycemic control, perianastomotic drainage management, and early mobilization protocols. Each recommendation was assigned specific evidence levels and graded for strength. High-quality evidence supported strong recommendations for the routine avoidance of prophylactic drainage in uncomplicated hepatectomy, early drain removal after pancreatoduodenectomy in low-risk patients, elimination of routine nasogastric decompression, and the implementation of early mobilization strategies.
Conclusion
These Korean-adapted ERAS guidelines for HBP surgery are expected to standardize perioperative care, reduce postoperative complications, shorten hospital stays, and enhance overall patient outcomes across Korean healthcare institutions. -
Citations
Citations to this article as recorded by
- Adapting Enhanced Recovery After Surgery for hepatobiliary and pancreatic surgery: a Korean perspective
Sang Hyun Shin
Ann Clin Nutr Metab.2026; 18(1): 1. CrossRef - Comparative evaluation of immediate outcomes of ERAS-associated and traditional postoperative management after pancreatic resection
J. A. Abdullozoda, Y. F. Tagoymurodov, A. I. Murodzoda, S. G. Ali-Zade
Health care of Tajikistan.2026; (2): 11. CrossRef
- Adapting Enhanced Recovery After Surgery for hepatobiliary and pancreatic surgery: a Korean perspective
- 4,121 View
- 98 Download
- 2 Crossref

Original Articles
- Perioperative nutritional practices and pediatric nutrition support team implementation in Korea: a cross-sectional study
-
Dayoung Ko, Honam Hwang, Hee-Beom Yang, Joong Kee Youn, Hyun-Young Kim
- Ann Clin Nutr Metab 2025;17(3):181-187. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0027
-
 Graphical Abstract
Abstract
PDF
Graphical Abstract
Abstract
PDF Supplementary Material
Supplementary Material - Purpose
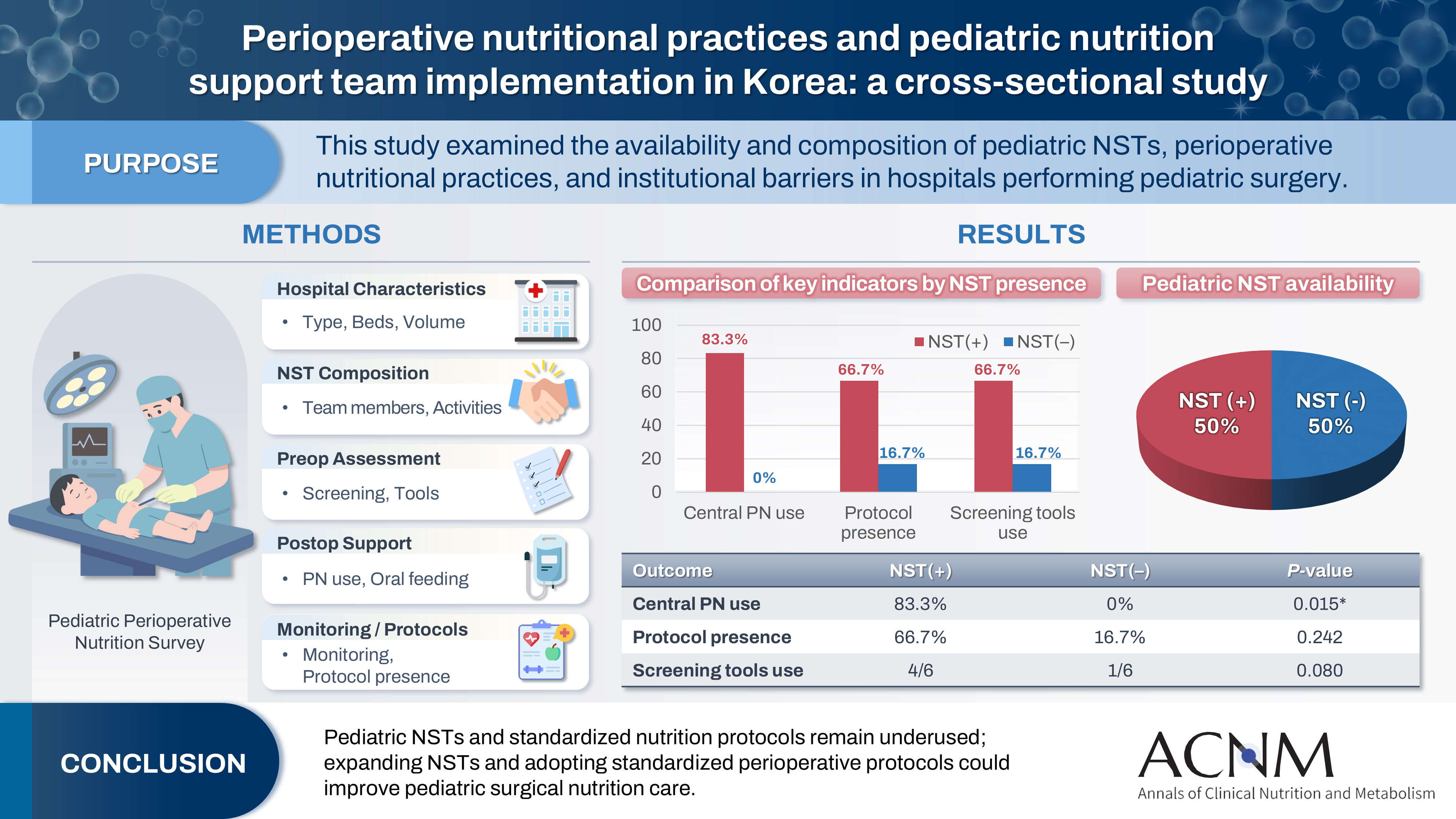
Pediatric surgical patients are vulnerable to perioperative malnutrition, yet standardized nutritional care and structured nutrition support team (NST) involvement remain inconsistent across institutions. Although multidisciplinary nutritional support has gained increasing attention, data on pediatric NST practices within surgical settings in Korea are limited. This study examined the availability and composition of pediatric NSTs, perioperative nutritional practices, and barriers in hospitals performing pediatric surgery.
Methods
A nationwide cross-sectional survey was conducted among tertiary and secondary hospitals that perform pediatric surgery in Korea. The questionnaire assessed hospital characteristics, the presence and composition of pediatric NSTs, perioperative nutritional screening and support practices, monitoring protocols.
Results
A total of 12 hospitals participated. Although all were high-capacity institutions, only half reported having a pediatric NST. Routine preoperative nutritional screening was performed in 50% of hospitals, and validated tools such as Screening Tool for the Assessment of Malnutrition in Pediatrics (STAMP) and Pediatric Yorkhill Malnutrition Score (PYMS) were used in 41.7%. Hospitals with a pediatric NST more frequently had institutional protocols for nutritional evaluation (66.7% vs. 16.7%) and were more likely to administer central venous parenteral nutrition postoperatively (83.3% vs. 0%, P=0.015). Enhanced Recovery After Surgery protocols were implemented in only two hospitals (16.7%). Major barriers to pediatric NST operation included insufficient staffing and time constraints.
Conclusion
Pediatric NSTs and standardized perioperative nutrition protocols remain underutilized in Korean surgical centers. Institutions with a pediatric NST demonstrated more structured nutritional practices. Expanding NST infrastructure and establishing standardized perioperative protocols for pediatric surgical patients may enhance the quality and consistency of nutritional care.
- 2,522 View
- 43 Download
- Successful introduction of ERAS in pancreaticoduodenectomy: what is real minimally invasive surgery?
-
Toshimi Kaido
 , Yosuke Miyachi, Koichiro Mitsuoka, Mariko Sambommatsu
, Yosuke Miyachi, Koichiro Mitsuoka, Mariko Sambommatsu - Ann Clin Nutr Metab 2025;17(2):156-161. Published online August 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0014
-
Graphical Abstract
Abstract
PDF
- Purpose
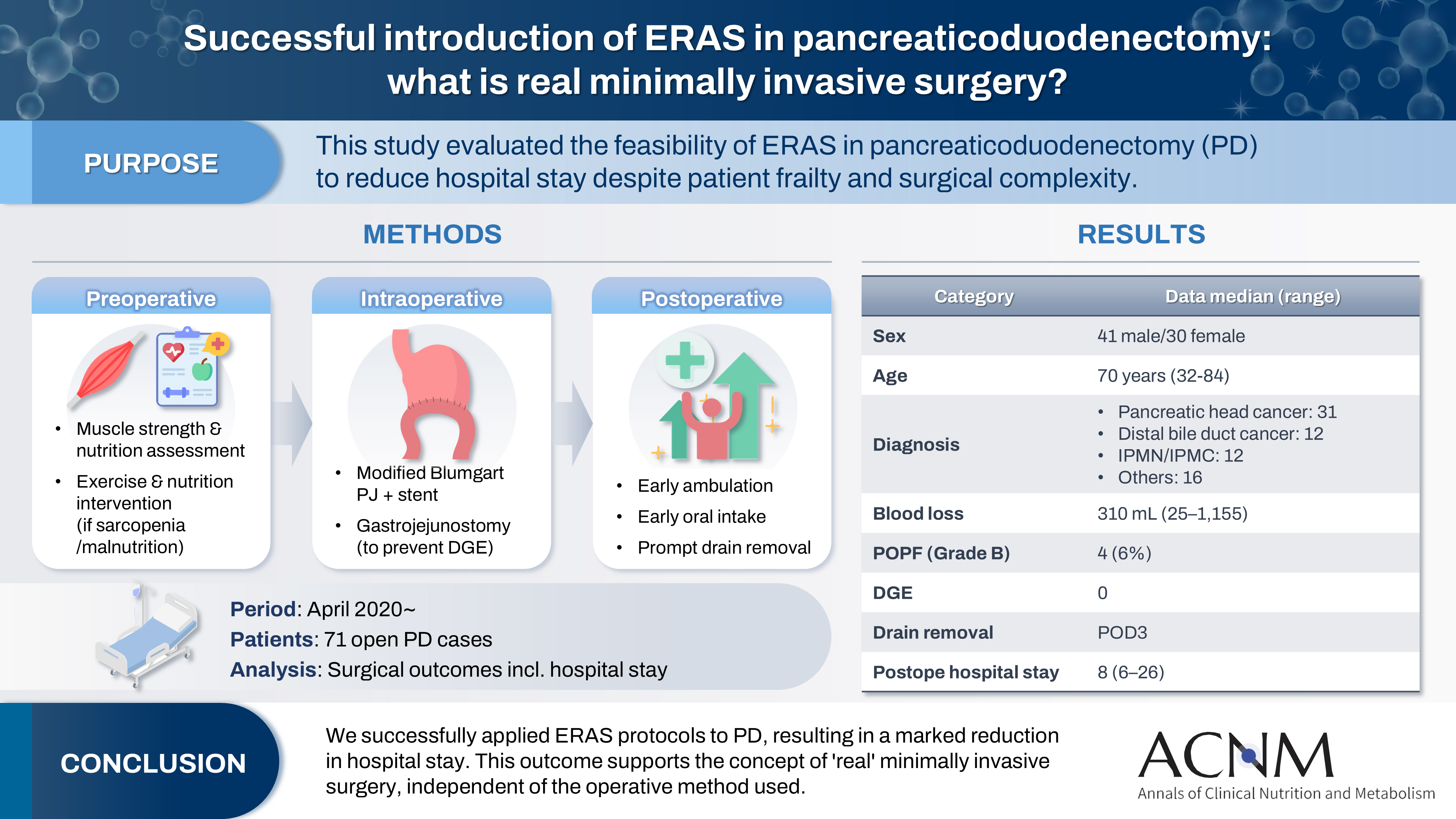
The introduction of Enhanced Recovery After Surgery (ERAS) protocols for pancreaticoduodenectomy (PD) has been considered challenging due to factors such as preexisting malnutrition, sarcopenia, the complexity of the surgery, and the high incidence of postoperative complications, including postoperative pancreatic fistula (POPF) and delayed gastric emptying (DGE). This study aimed to determine whether ERAS could be implemented in PD to achieve shorter postoperative hospital stays.
Methods
Our novel approach consists of three components. Preoperatively, we routinely assess patients' muscle strength and nutritional status and initiate exercise and nutritional interventions for those identified with sarcopenia or malnutrition. Intraoperatively, we perform pancreaticojejunostomy using a modified Blumgart’s technique with our stent placement policy and utilize new gastrojejunostomy methods to prevent DGE. Principles of postoperative management are early ambulation, early oral intake, and early drain removal. Since April 2020, we have employed this strategy and retrospectively evaluated its effectiveness. We enrolled 71 consecutive patients who underwent open PD with curative intent. Various surgical outcomes, including postoperative hospital stay, were analyzed.
Results
There were 41 men and 30 women, with a median age of 70 years. Preoperative diagnoses included pancreatic head cancer in 31, distal bile duct cancer in 12, and others. Median intraoperative blood loss was 310 mL. Grade B POPF occurred in four patients (6%). No cases of DGE were observed. The median postoperative hospital stay was 8 days (range, 6–26 days).
Conclusion
We successfully implemented ERAS protocols in PD and achieved a significantly reduced postoperative hospital stay. We propose that this approach is “real minimally invasive surgery," regardless of the surgical technique used.
- 5,015 View
- 33 Download
- Comparison of efficacy of enteral versus parenteral nutrition in patients after esophagectomy in Malaysia: a prospective cohort study
-
Ramizah Mohd Shariff
 , Sze Chee Tee, Shukri Jahit Mohammad, Khei Choong Khong
, Sze Chee Tee, Shukri Jahit Mohammad, Khei Choong Khong - Ann Clin Nutr Metab 2025;17(1):41-49. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.24.016
-
Graphical Abstract
Abstract
PDF
- Purpose
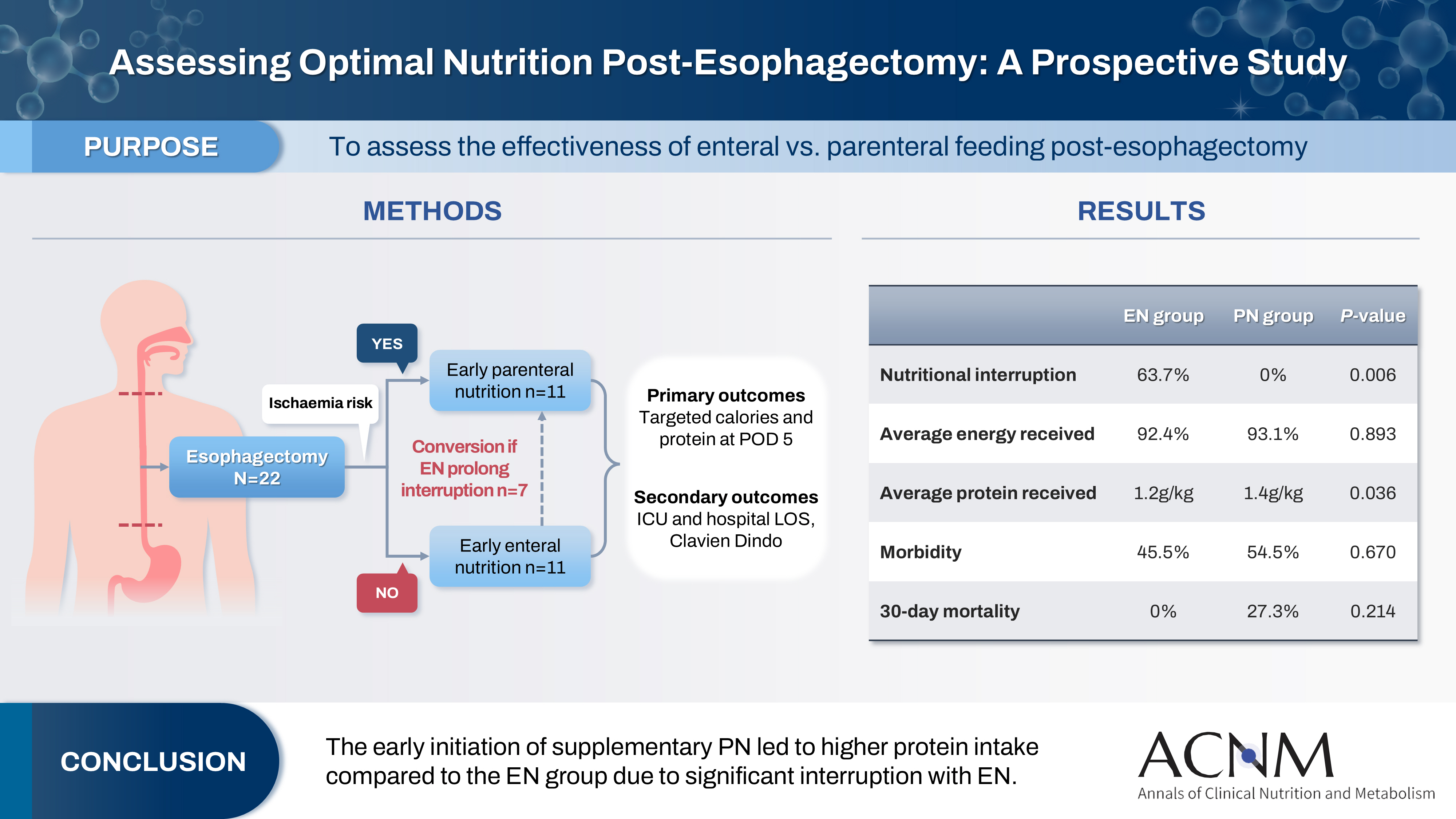
This study aims to assess the effectiveness of enteral versus parenteral feeding in patients after esophagectomy.
Methods
This a prospective cohort study of post-esophagectomy intensive care unit (ICU) patients over 12 months in the National Cancer Institute, Malaysia. Early enteral feeding followed the Enhanced Recovery After Surgery protocol, and parenteral nutrition (PN) was considered if there was a risk for conduit ischemia. It compared the effectiveness of enteral versus PN following esophagectomy, and assessed the correlations between biochemical nutritional markers and hospital lengths of stay or ventilation days.
Results
It included two cohorts receiving PN (n=11) or enteral nutrition (EN) (n=11) following elective esophagectomy. Preoperative weight, body mass index, and Subjective Global Assessment were higher in the EN group (P=0.033, P=0.021, P=0.031, respectively). Nutritional interruption occurred more frequently in the EN group (63.7%) compared to the PN group (P=0.001). Mean levels of energy and protein received were 93.1 kcal/kg and 1.4 g/kg for PN versus 92.4 kcal/kg and 1.2 g/kg for EN (P=0.893, P=0.036). The median lengths of ICU stay (P=0.688) and postoperative stay (P=0.947) between groups showed no significant difference. In addition, 30-day mortality (P=0.214) and other postoperative complications (P>0.05) were comparable in the two groups.
Conclusion
Early initiation of supplementary PN due to significant interruption in EN led to higher protein intake compared to the EN group. However, there were no significant differences in postoperative outcomes, including 30-day mortality, ICU length of stay, and ventilation days. PN ensures adequate nutritional intake, especially in terms of protein delivery, without adversely affecting postoperative recovery and clinical outcomes. -
Citations
Citations to this article as recorded by- Optimizing nutritional support in upper gastrointestinal surgery: A comprehensive review of feeding jejunostomy techniques and outcomes
Ioana Alexandra Prisacariu, Konstantinos Eleftherios Koumarelas, Konstantinos Argyriou, Alexandros Charalabopoulos, Grigorios Christodoulidis
World Journal of Gastrointestinal Surgery.2025;[Epub] CrossRef
- Optimizing nutritional support in upper gastrointestinal surgery: A comprehensive review of feeding jejunostomy techniques and outcomes
- 7,478 View
- 88 Download
- 1 Crossref
- Perioperative nutritional practice of surgeons in Korea: a survey study
-
Ji-Hyeon Park, Mi Ran Jung, Sang Hyun Kim, Hongbeom Kim, Gyeongsil Lee, Jae-Seok Min, Heung-Kwon Oh, Jung Hoon Bae, Yoona Chung, Dong-Seok Han, Seung Wan Ryu, The External Relation Committee of the Korean Society of Surgical Metabolism and Nutrition
- Ann Clin Nutr Metab 2024;16(3):134-148. Published online December 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.3.134
-
Abstract
PDFSupplementary Material
- Purpose: Enhanced recovery after surgery (ERAS) protocols advocate reduced fasting and early nutrition to improve recovery in surgical patients. However, data on ERAS implementation among Korean surgeons performing major abdominal surgeries remain sparse.
Methods: A survey conducted by the External Relation Committee of the Korean Society of Surgical Metabolism and Nutrition assessed perioperative nutritional practices among 389 Korean general surgeons from February to September 2023. The survey covered preoperative fasting, carbohydrate drinks, nasogastric tube use, postoperative dietary progression, parenteral nutrition (PN), and oral supplements, yielding 551 responses stratified by specialty.
Results: More than 80% of respondents practiced “midnight NPO (Nil Per Os)” fasting, often at the anesthesiology department’s request, while 70%–80% reported no use of preoperative carbohydrate drinks. Most surgeons began dietary progression with water on postoperative day one, advancing to a liquid or soft diet by day two. PN was routinely prescribed by 49% of respondents, with a common dosage of 1,000–1,500 kcal/d. Oral supplements were selectively provided, with 21% of surgeons prescribing them universally.
Conclusion: The results reveal significant variability in perioperative nutrition practices across Korean surgical specialties, with many adhering to traditional practices despite ERAS guidelines. These findings highlight a need for standardized guidelines in Korea to optimize perioperative nutritional support and improve patient recovery outcomes following major abdominal surgeries. -
Citations
Citations to this article as recorded by- Development of the Korean enhanced recovery after surgery audit program
Soo-Hyuk Yoon, Jae-Woo Ju, Ho-Jin Lee, Jeesun Kim, Min Jung Kim, Ji Won Park, Do Joong Park, Seung Yong Jeong
Scientific Reports.2025;[Epub] CrossRef - Perioperative nutrition practices in gastrointestinal cancer surgery: A nationwide survey among German surgical departments
Rahel Maria Strobel, Katharina Beyer, Johannes Christian Lauscher, Marc Martignoni, Christoph Reißfelder, Tim Vilz, Arved Weimann, Maria Wobith
Langenbeck's Archives of Surgery.2025;[Epub] CrossRef
- Development of the Korean enhanced recovery after surgery audit program
- 8,414 View
- 99 Download
- 2 Crossref
Guideline
- The 2024 Korean Enhanced Recovery After Surgery guidelines for colorectal cancer
-
Kil-yong Lee, Soo Young Lee, Miyoung Choi, Moonjin Kim, Ji Hong Kim, Ju Myung Song, Seung Yoon Yang, In Jun Yang, Moon Suk Choi, Seung Rim Han, Eon Chul Han, Sang Hyun Hong, Do Joong Park, Sang-Jae Park, The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition
- Ann Clin Nutr Metab 2024;16(2):22-42. Published online August 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.2.22
-
Abstract
PDFSupplementary Material
- The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition was established to develop ERAS guidelines tailored to the Korean context. This guideline focuses on creating the most current evidence-based practice guidelines for ERAS based on systematic reviews. All key questions targeted randomized controlled trials (RCTs) exclusively. If fewer than two RCTs were available, studies using propensity score matching were also included. Recommendations for each key question were marked with strength of recommendation and level of evidence following internal and external review processes by the committee.
-
Citations
Citations to this article as recorded by- Development of the Korean enhanced recovery after surgery audit program
Soo-Hyuk Yoon, Jae-Woo Ju, Ho-Jin Lee, Jeesun Kim, Min Jung Kim, Ji Won Park, Do Joong Park, Seung Yong Jeong
Scientific Reports.2025;[Epub] CrossRef - Optimizing postoperative pain management in minimally invasive colorectal surgery
Soo Young Lee
Annals of Coloproctology.2024; 40(6): 525. CrossRef
- Development of the Korean enhanced recovery after surgery audit program
- 13,728 View
- 191 Download
- 2 Crossref
Original Articles
- Survey and Analysis of the Application and Implementations of Enhanced Recovery after Surgery (ERAS) Program for Surgical Patients in the Major Hospitals in Korea
- Eun Young Kim, In Kyu Lee
- Surg Metab Nutr 2019;10(2):32-45. Published online December 30, 2019
- DOI: https://doi.org/10.18858/smn.2019.10.2.32
-
Abstract
PDF
Purpose:
A questionnaire survey was conducted using e-mail to investigate the application status of ERAS in Korea and its implementation by their institution. The perceptions of ERAS by medical staff and the factors that interfered with the application of ERAS were investigated.
Materials and Methods:
From July 2017 to March 2019, a questionnaire was sent by e-mail to members of the KSSMN. This consisted of 41 questions divided into three parts to investigate 1) respondents’ prior knowledge and understanding of ERAS, 2) actual components of ERAS and its clinical application, and 3) performance and preference of the respondents to ERAS. The items were categorized into “high acceptance” when more than 75% of respondents answered “yes”, or the items into “low acceptance” when less than 25% answered “no”.
Results:
Overall, 86 participants completed the survey. Of these, 59(68.6%) had prior knowledge of ERAS and 29 (33.7%) applied ERAS clinically. Seventy (81.4%) and 40 (46.5%) answered that ERAS would have a positive effect on shortening the hospital stay and reducing the number of complications. Seventy four (86%) indicated that they would implement ERAS in the future. The factors impeding the implementation of ERAS were a lack of understanding of physicians and a shortage of manpower and resources for ERAS.
Conclusion:
The ERAS implementation rate and awareness level of surgeons were low, but the positive expectations of the clinical efficacy of ERAS and the wiliness to accept were high. Overall, it would be necessary to cooperate with institutions to improve the manpower and resources, and supplement the education to overcome the lack of awareness, which has been pointed out as an obstacle to the implementation of ERAS.
-
Citations
Citations to this article as recorded by- Enhancing postoperative recovery with multimodal prehabilitation: the journey begins before surgery
Ah-Reum Cho, Wariya Vongchaiudomchoke, Detlef Balde, Do Jun Kim, Francesco Carli
Korean Journal of Anesthesiology.2025; 78(5): 401. CrossRef - Challenging issues of implementing enhanced recovery after surgery programs in South Korea
Soo-Hyuk Yoon, Ho-Jin Lee
Anesthesia and Pain Medicine.2024; 19(1): 24. CrossRef - Perioperative nutritional practice of surgeons in Korea: a survey study
Ji-Hyeon Park, Mi Ran Jung, Sang Hyun Kim, Hongbeom Kim, Gyeongsil Lee, Jae-Seok Min, Heung-Kwon Oh, Jung Hoon Bae, Yoona Chung, Dong-Seok Han, Seung Wan Ryu
Annals of Clinical Nutrition and Metabolism.2024; 16(3): 134. CrossRef - Effects of the Enhanced Recovery After Surgery (ERAS) Program for Colorectal Cancer Patients Undergoing Laparoscopic Surgery
Jeongwon Yeom, Hee-Sook Lim
Clinical Nutrition Research.2022; 11(2): 75. CrossRef - Effect of Non-contact Korean Medical Treatment for Patients Recovering at Home with Positive Coronavirus Disease 2019 Diagnostic Test Results at a Local Public Health Center : A Retrospective Chart Review
Chaeheun Jeon, Daejun Choi, Gyeongmuk Kim, Hyejin Kim, Jungtae Leem, Gyoo-yong Chi
Journal of Physiology & Pathology in Korean Medicine.2022; 36(4): 130. CrossRef - Perception and implementation status of enhanced recovery after surgery
Eun Young Kim
Journal of the Korean Medical Association.2021; 64(12): 826. CrossRef - Background for the introduction of enhanced recovery after surgery and patient outcomes
Do Joong Park
Journal of the Korean Medical Association.2021; 64(12): 801. CrossRef
- Enhancing postoperative recovery with multimodal prehabilitation: the journey begins before surgery
- 1,883 View
- 26 Download
- 7 Crossref
- Pilot Study for Safety and Efficacy of Newly Developed Oral Carbohydrate-Rich Solution Administration in Adult Surgery Patients
- Won-Bae Chang, Kyuwhan Jung, Sang-Hoon Ahn, Heung-Gwon Oh, Mi-Ok Yoon
- J Clin Nutr 2016;8(1):24-28. Published online April 30, 2016
- DOI: https://doi.org/10.15747/jcn.2016.8.1.24
-
Abstract
PDF
Purpose:
In surgical procedures under general anesthesia, 6 to 8 hours of a
nulla per os (NPO; nothing by mouth) has been regarded as essential for prevention of respiratory complication such as aspiration. However, recent studies have reported that oral intake of water and other clear fluids up to 2 hours before induction of anesthesia does not increase respiratory problems. The purpose of this pilot study is to investigate the safety and efficacy of a newly developed carbohydrate-rich solution in elective hernia repair surgery patients.Methods:
A group of 30 adult patients scheduled for elective surgeries under general anesthesia were enrolled. The enrolled study group of patients was permitted to drink a carbohydrate-rich solution until two hours before the operation without volume limitation. Respiratory complication was investigated in the patients using the carbohydrate-rich solution until two hours before induction of general anesthesia. The feelings of thirst, hunger sense were measured pre- and post-operatively. In addition, hoarseness of voice, nausea and vomiting were investigated post-operatively. Satisfaction regarding the short time of fasting was measured. Visual analogue scale (VAS) was used for measurement of these six variables.
Results:
No patients showed serious respiratory complication such as dyspnea, desaturation. Eight of 30 study group patients complained of mild hoarseness. Most symptoms of hoarseness were mild, with VAS score less than 3 out of 10. Two patients complained 5 out of 10. Six patients felt nausea and 1 patient had vomiting. Pre/post-operative hunger sense and thirst feeling were 1.63/1.60 and 1.90/5.76, respectively. The satisfaction score was 3.00 out of 4.
Conclusion:
Allowing the administration of an oral carbohydrate-rich solution in elective surgery patients requiring general anesthesia is safe without serious respiratory complications and effective in providing satisfaction.
-
Citations
Citations to this article as recorded by- The safety and effect of preoperative reduced fasting time by oral clear liquid administration in adult surgery patients: a randomized controlled trial
Donghyoun Lee, Soo-Jin Kim, Won-Bae Chang
Annals of Surgical Treatment and Research.2025; 109(1): 1. CrossRef - Oral high-carbohydrate solution as an alternative dietary modality in patients with acute pancreatitis
See Young Lee, Jaein Lee, Jae Hee Cho, Dong Ki Lee, Yeseul Seong, Sung Ill Jang
Pancreatology.2024; 24(7): 1003. CrossRef - Patient-reported outcome measures on intake of nutrition drink for nutritional supplements after periodontal surgery
Hyeong-Seok Kim, In-Woo Cho, Hyun-Seung Shin, Jung-Chul Park
Journal of Dental Rehabilitation and Applied Science.2016; 32(3): 176. CrossRef
- The safety and effect of preoperative reduced fasting time by oral clear liquid administration in adult surgery patients: a randomized controlled trial
- 2,345 View
- 1 Download
- 3 Crossref
- Enhanced Recovery After Surgery is Feasible in Laparoscopic Low Anterior Resection for Rectal Cancer
- Jeong Seon Jo, Soo Young Lee, Hun Jin Kim, Chang Hyun Kim, Young Jin Kim, Hyeong Rok Kim
- Surg Metab Nutr 2015;6(1):11-15. Published online June 30, 2015
- DOI: https://doi.org/10.18858/smn.2015.6.1.11
-
Abstract
PDF
Purpose:
The aim of this study was to compare short-term outcomes in patients who underwent laparoscopic assisted low anterior resection for colorectal cancer. The patients received either conventional perioperative care or the Enhanced Recovery After Surgery (ERAS) procedural care.
Materials and Methods:
A retrospective review was conducted in patients who underwent elective laparoscopic low anterior resection for colorectal cancer between May, 2011 and December, 2013. Patients were grouped and analyzed according to the perioperative care program of ERAS and conventional care.
Results:
A total of 81 patients received care via the ERAS pathway and 230 patients received care via conventional pathway. There was no significant difference in postoperative morbidity rates (P=0.381). The post-operative morbidity rates were 30.9% and 25.2% in the ERAS and conventional groups. No significant difference in hospital stay (9.0±6.8 vs. 8.6±3.5 days; P=0.575) was observed between the 2 groups.
Conclusion:
No short-term perioperative disadvantages were found for the ERAS program compared with the conventional perioperative care for colorectal cancer patients who underwent laparoscopic low anterior resection. (Surg Metab Nutr 2015;6:11-15)
- 1,276 View
- 4 Download
 First
First Prev
Prev

