 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Search
- Page Path
- HOME > Search
Original Article
- Association of soy oil-based lipid injectable emulsion with early body weight loss after minimally invasive esophagectomy in Japan: a retrospective cohort study
-
Tomonori Narita
 , Kazuhiko Fukatsu, Kenichi Kono, Satoshi Murakoshi, Reo Inoue, Midori Noguchi, Nana Matsumoto, Shoh Yajima, Koichi Yagi, Yoshifumi Baba
, Kazuhiko Fukatsu, Kenichi Kono, Satoshi Murakoshi, Reo Inoue, Midori Noguchi, Nana Matsumoto, Shoh Yajima, Koichi Yagi, Yoshifumi Baba - Ann Clin Nutr Metab 2026;18(1):34-43. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0030
-
 Graphical Abstract
Graphical Abstract
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Purpose
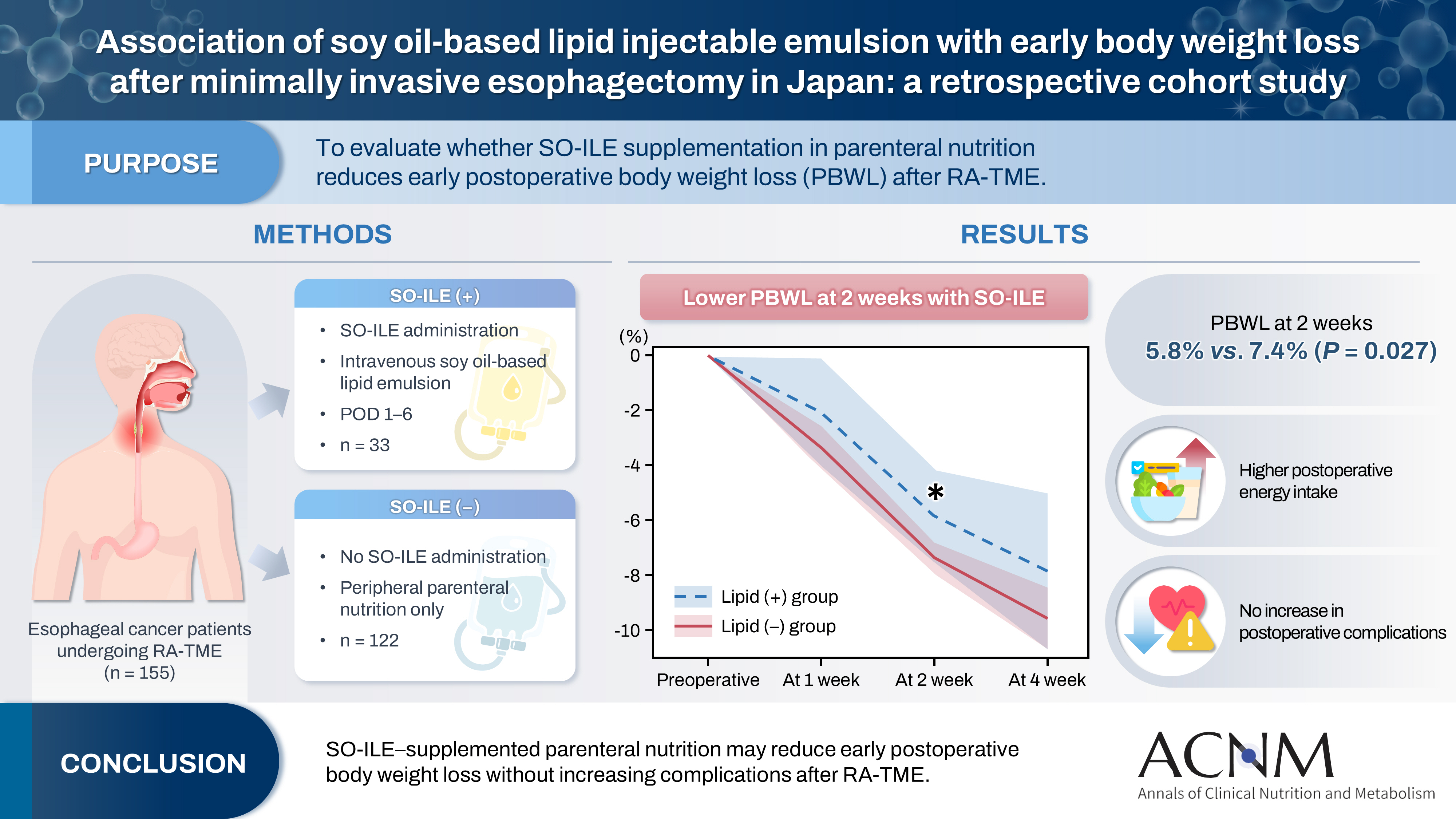
Postoperative body weight loss (PBWL) is associated with poor long-term outcomes following esophagectomy for esophageal cancer, underscoring the critical importance of perioperative nutritional management. Although minimally invasive procedures, such as robot-assisted radical transmediastinal esophagectomy (RA-TME), have become increasingly prevalent, perioperative nutritional strategies have received comparatively limited attention. This study evaluated the impact of soy oil-based injectable lipid emulsion (SO-ILE) on PBWL in patients undergoing RA-TME.
Methods
We retrospectively analyzed 155 patients who underwent RA-TME for esophageal or esophagogastric junction cancer at our hospital between 2011 and 2022. Patients were divided into two groups: the lipid (+) group (n=33), which received SO-ILE between postoperative days 1 and 6, and the lipid (–) group (n=122), which did not receive SO-ILE. Oral or enteral nutrition was withheld until postoperative day 6. Nutrient intake, postoperative outcomes, and nutritional status were compared between the two groups.
Results
Patient backgrounds, surgical outcomes, and postoperative complication rates were similar between the two groups. However, patients in the lipid (+) group received significantly greater total energy and nutrient intake. PBWL at 2 weeks after surgery was significantly lower in the lipid (+) group than in the lipid (–) group (5.8% vs. 7.4%; P=0.027). Univariate analysis showed that absence of SO-ILE administration was the only significant risk factor for PBWL greater than 5% at 2 weeks after RA-TME (P=0.038).
Conclusion
SO-ILE may have the potential to mitigate early PBWL after RA-TME.
- 784 View
- 14 Download

Review
- Effectiveness of perioperative rehabilitation and nutrition in esophageal cancer: a narrative review
-
Ryoma Haneda, Yuki Sakai, Kenichi Sekimori, Tomohiro Murakami, Eisuke Booka, Tomohiro Matsumoto, Hirotoshi Kikuchi, Yoshihiro Hiramatsu, Hiroya Takeuchi
- Ann Clin Nutr Metab 2026;18(1):18-26. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0021
-
Abstract
PDF
- Purpose
Esophageal cancer surgery requires robust perioperative management to reduce its high rate of complications. This review evaluates the clinical utility of comprehensive exercise and nutritional therapy, with a specific focus on initiatives led by the multidisciplinary Hamamatsu Perioperative Care Team (HOPE), established at Hamamatsu University Hospital to optimize patient safety and postoperative recovery outcomes.
Current concept
The HOPE protocol involves a diverse team, including surgeons, nurses, pharmacists, and dietitians, who collaboratively implement a multifaceted perioperative care bundle. These interventions include strict smoking cessation, intensive oral care, and immunonutrition incorporating n-3 fatty acids. A distinctive feature of this program is the integration of patient-reported treatment diaries and wearable fitness tracking devices (WFTs) to visualize daily activity, thereby helping to sustain patient motivation. Preoperative rehabilitation focuses on preventing sarcopenia through combined aerobic and resistance training, while postoperative care emphasizes immediate enteral nutrition and early mobilization. Retrospective analyses demonstrated that HOPE implementation reduced Clavien-Dindo grade III or higher infectious complications, pneumonia and surgical site infections, compared with historical controls. In addition, a propensity score–matched analysis showed that WFT users experienced lower pneumonia rates, shorter hospital stays, and better preservation of nutritional markers, including albumin and transthyretin, during the recovery phase compared with non-users.
Conclusion
The HOPE strategy illustrates that combining standard nutritional support and exercise therapy with digital tools enables individualized rehabilitation. This integrated approach reduces morbidity and preserves function, strongly suggesting that incorporation of wearable technology into established surgical care protocols represents a strategy for improving long-term outcomes in high-risk cancer patients.
- 757 View
- 17 Download
Original Articles
- Peripheral vein infusions of amino acids prevent early postoperative weight loss after robot-assisted radical transmediastinal esophagectomy: a retrospective study in Japan
-
Tomonori Narita, Kazuhiko Fukatsu, Satoshi Murakoshi, Reo Inoue, Kenichi Kono, Midori Noguchi, Nana Matsumoto, Shoh Yajima, Koichi Yagi, Yoshifumi Baba
- Ann Clin Nutr Metab 2025;17(2):149-155. Published online August 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0012
-
Graphical Abstract
Abstract
PDFSupplementary Material
- Purpose
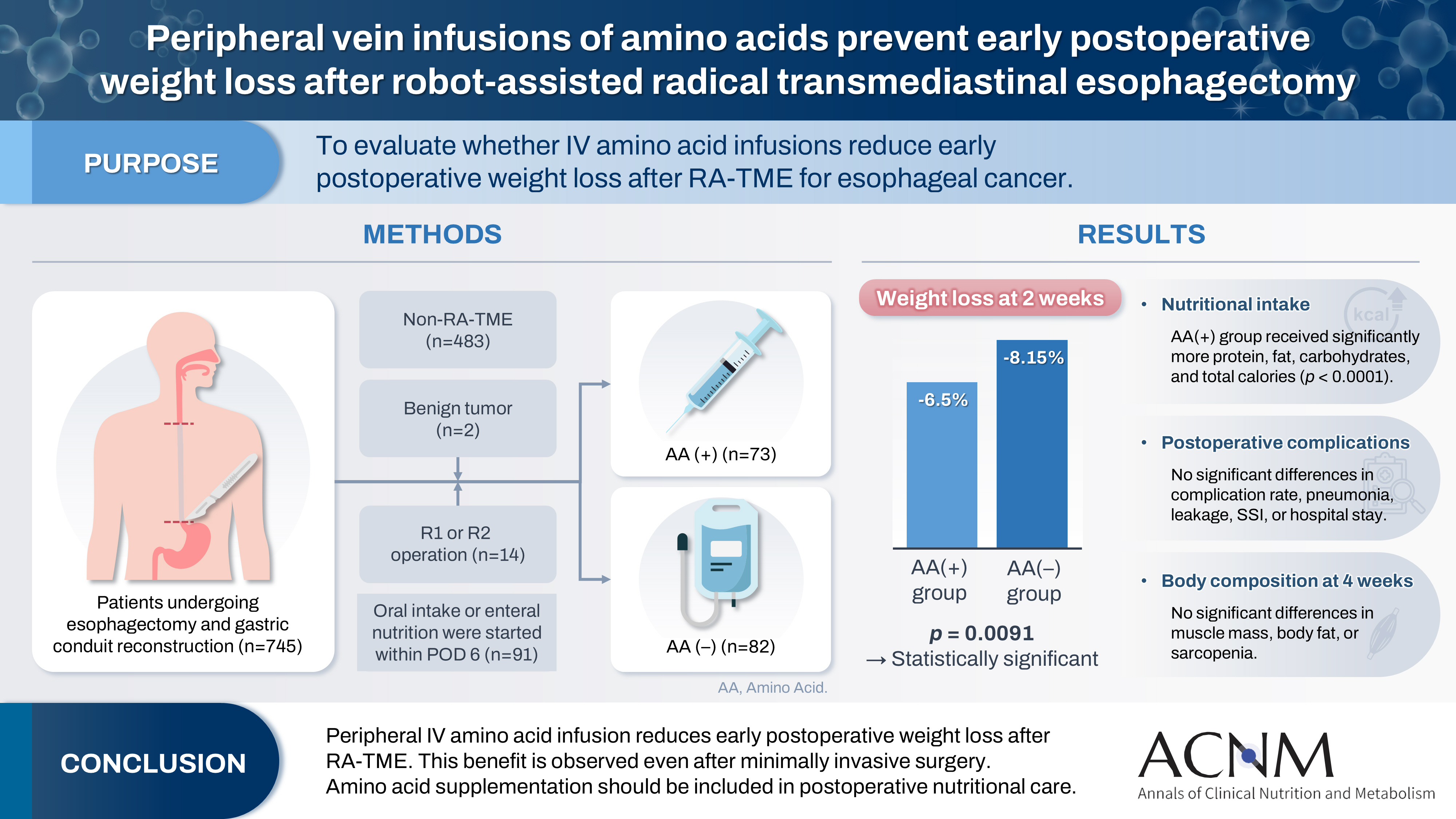
Postoperative body weight loss (PBWL) is linked to poor long-term outcomes following esophagectomy for esophageal cancer, making perioperative nutrition critically important. Although minimally invasive procedures such as robot-assisted radical transmediastinal esophagectomy (RA-TME) have become more prevalent, less attention has been paid to perioperative nutritional management. This study evaluates the impact of intravenous (IV) amino acid infusions on PBWL in patients undergoing RA-TME.
Methods
We retrospectively analyzed 155 patients who underwent RA-TME for esophageal or esophagogastric junction cancer at our hospital between 2011 and 2022. Patients were divided into two groups: AA(+) (n=73, received IV amino acids between postoperative days 1–6) and AA(–) (n=82, did not receive IV amino acids). Oral or enteral nutrition was withheld until postoperative day 6. We compared nutrient intake, postoperative outcomes, and nutritional status between groups.
Results
Patient backgrounds, surgical outcomes, and complication rates were similar in both groups. However, the AA(+) group received significantly greater energy and nutrient intake. PBWL at 2 weeks post-surgery was significantly lower in the AA(+) group than in the AA(–) group (6.50% vs. 8.15%, P=0.0091).
Conclusion
IV amino acid infusion may help mitigate early PBWL after RA-TME.
- 1,868 View
- 25 Download
- The enteral feeding tube access route in esophageal cancer surgery in Japan: a retrospective cohort study
-
Hiroyuki Kitagawa, Keiichiro Yokota, Tsutomu Namikawa, Kazuhiro Hanazaki
- Ann Clin Nutr Metab 2025;17(1):58-65. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0003
-
Graphical Abstract
Abstract
PDF
- Purpose
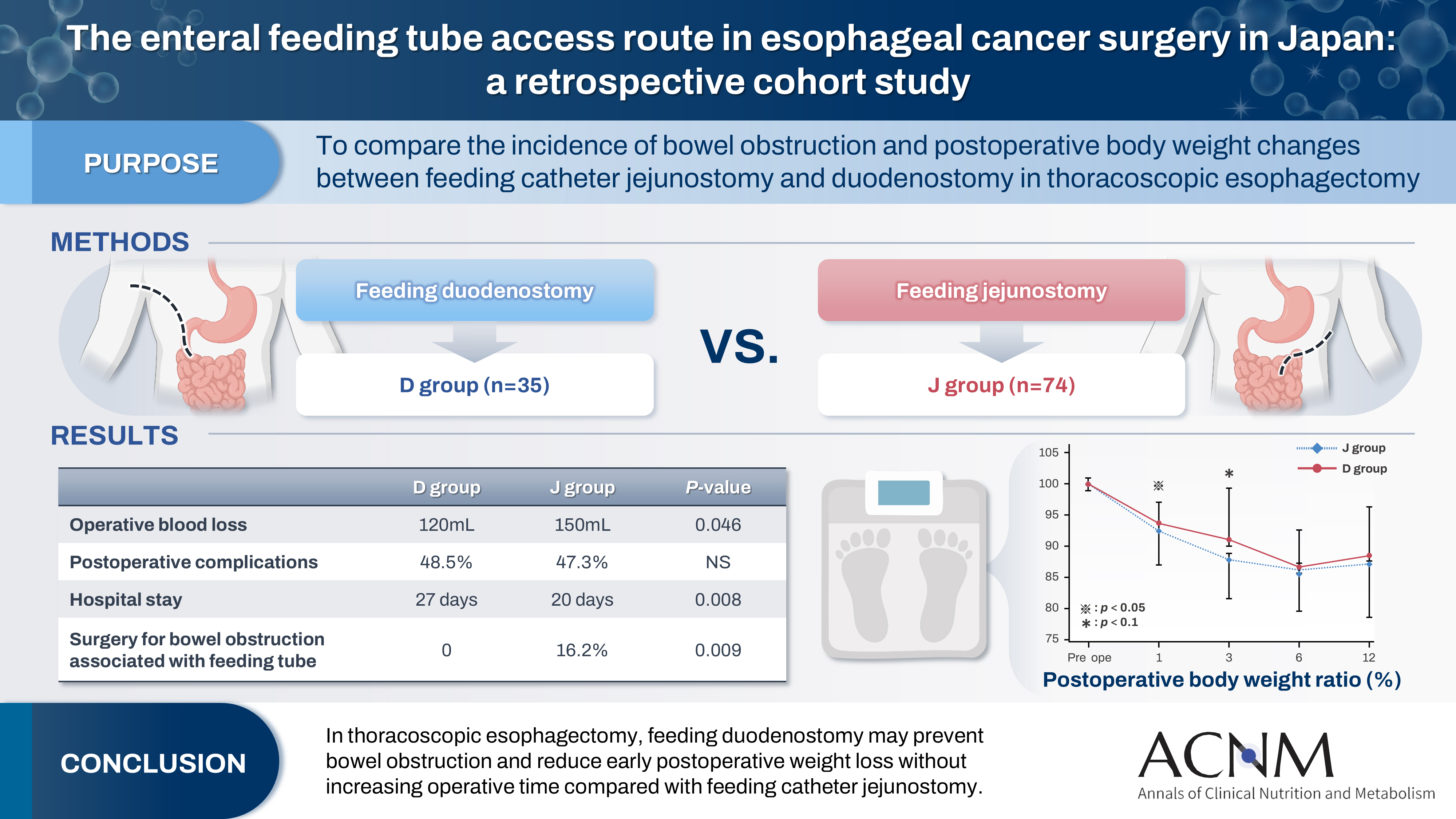
Feeding catheter jejunostomy is a useful access route for early enteral nutrition during esophageal cancer surgery. However, it may lead to postoperative bowel obstruction associated with feeding jejunostomy (BOFJ). To prevent BOFJ, we introduced feeding catheter duodenostomy via the round ligament in 2018. This study aimed to compare the incidence of BOFJ and postoperative body weight changes between feeding catheter jejunostomy and duodenostomy.
Methods
A total of 109 patients who underwent thoracoscopic esophagectomy and gastric tube reconstruction for esophageal cancer at Kochi Medical School Hospital between March 2013 and November 2020 were included. Preoperative patient characteristics (age, sex, preoperative weight, body mass index, cancer stage, and preoperative treatment), surgical outcomes (operative time, blood loss, and postoperative complications [wound infection, pneumonia, anastomotic leakage, BOFJ]), and body weight changes at 1, 3, 6, and 12 months post-surgery were compared between the jejunostomy (J) and duodenostomy (D) groups.
Results
The D group consisted of 35 patients. No significant differences were observed between the groups regarding age, sex, weight, body mass index, cancer stage, operative time, postoperative complications, or duration of tube placement. However, the D group had a significantly lower rate of preoperative chemotherapy (45.7% vs. 78.4%, P=0.001) and lower operative blood loss (120 mL vs. 150 mL, P=0.046) than the J group. All 12 cases of BOFJ occurred in the J group. Furthermore, the D group experienced a significantly lower weight loss ratio at 1 month postoperatively (93.9% vs. 91.8%, P=0.039).
Conclusion
In thoracoscopic esophagectomy, feeding duodenostomy may prevent bowel obstruction and reduce early postoperative weight loss without increasing operative time compared with feeding catheter jejunostomy. -
Citations
Citations to this article as recorded by
- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
Ye Rim Chang
Ann Clin Nutr Metab.2025; 17(2): 95. CrossRef
- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
- 3,919 View
- 42 Download
- 1 Crossref
- Evaluation of Postoperative Nutrition Support with Commercial Peripheral Parenteral Nutrition after an Ivor-Lewis Esophagectomy in Patients with Esophageal Cancer
- Sun-woo Lee, Na-ri Lim, Hyo Jung Park, Yong-won In, Jeong-meen Seo, Young-mee Lee
- J Clin Nutr 2015;7(3):87-92. Published online December 31, 2015
- DOI: https://doi.org/10.15747/jcn.2015.7.3.87
-
Abstract
PDF
Purpose:
Deteriorated nutritional status is common during a hospital stay for esophagectomy in patients with esophageal cancer. Malnutrition in those patients is often marked compared with other gastrointestinal cancer. The purpose of this study is to evaluate the appropriateness of commercial peripheral parenteral nutrition (CPPN) use in patients who underwent Ivor-Lewis esophagectomy (I-L op).
Methods:
Patients who were provided with CPPN after I-L op were enrolled in this study from January to May 2015. Body weight, height, nutritional status, length of hospital stay, duration of CPPN therapy, and parenteral nutrition (PN) induced complications were assessed, respectively, using electronic medical records.
Results:
Thirty-nine patients were enrolled. Average age was 65.9 years and 36 patients were male. All patients were provided with the same CPPN. The duration of fasting and CPPN use was 5.8±1.4 days and 7.5±1.8 days, respectively. Calorie supported by CPPN was 22.6±3.5 kcal/kg/day and only 20.5% of patients (n=8) reached the daily target calories. Most frequent PN induced complication was phlebitis which occurred in 8 patients (20.5%). Calcium, magnesium, and transthyretin levels in serum were not monitored during the PN support period.
Conclusion:
The indications for CPPN were appropriate because the fasting duration in patients with I-L op was 5 to 10 days. Although a large portion of patients could not be supplied daily target calories, their nutrition status was not significantly changed on admission and at discharge. We did not find it necessary to individualize PN support for a short period after an I-L op in patients with esophageal cancer. Further study will be needed to determine why the incidence of phlebitis was dominant.
- 1,143 View
- 2 Download
 First
First Prev
Prev

