 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Search
- Page Path
- HOME > Search
Original Article
- Association between the calcium-to-phosphorus ratio and early hypophosphatemia in preterm infants receiving parenteral nutrition in Korea: a retrospective cohort study
-
Miseon Han
 , Jin Ok Kyun, Yoong-A Suh, Jang Hoon Lee
, Jin Ok Kyun, Yoong-A Suh, Jang Hoon Lee - Ann Clin Nutr Metab 2026;18(1):44-53. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0039
-
 Graphical Abstract
Graphical Abstract
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Purpose
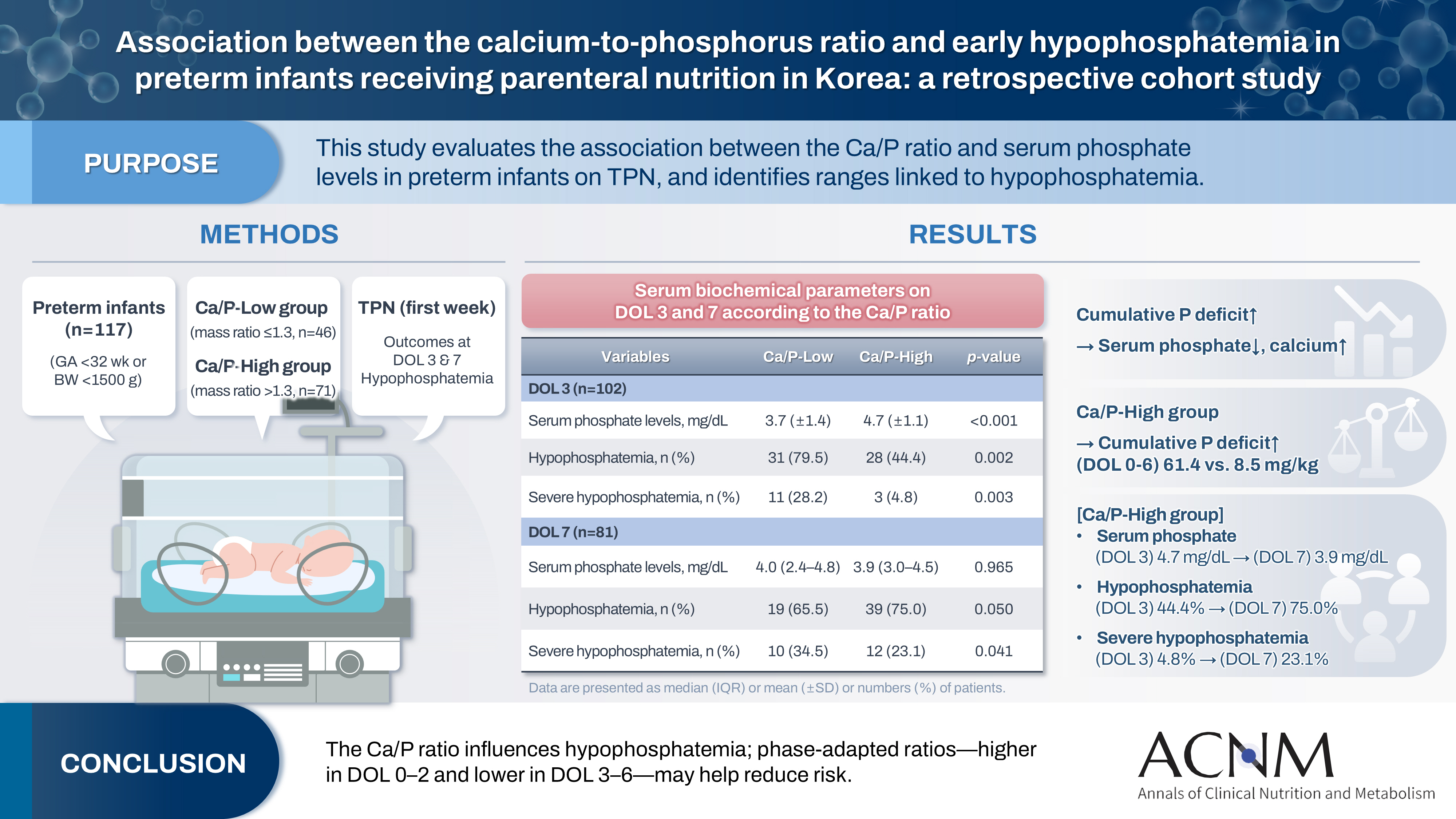
This study aimed to evaluate the association between the calcium-to-phosphorus (Ca/P) ratio and serum phosphate levels in preterm infants receiving total parenteral nutrition (TPN) and to explore Ca/P ratio ranges associated with hypophosphatemia.
Methods
We retrospectively reviewed the medical records of preterm infants admitted to the neonatal intensive care unit at Ajou University Hospital between January 2022 and June 2024. The review focused on TPN composition and serum electrolyte changes during the first week of life. Based on the cumulative Ca/P ratio during this period, infants were categorized into two groups: Ca/P-Low (mass ratio ≤1.3) and Ca/P-High (mass ratio >1.3).
Results
A total of 117 preterm infants were included in the analysis (Ca/P-Low group, n=46; Ca/P-High group, n=71). During the first week of life, the cumulative phosphorus deficit was significantly greater in the Ca/P-High group (61.4 mg/kg vs. 8.5 mg/kg; P<0.001). By day of life (DOL) 7, both hypophosphatemia and severe hypophosphatemia had increased markedly in the Ca/P-High group compared with DOL 3. In the Ca/P-High group, the incidence of hypophosphatemia increased from 44.4% on DOL 3 to 75.0% on DOL 7, while the incidence of severe hypophosphatemia increased from 4.8% to 23.1%.
Conclusion
These findings suggest that parenteral nutrition strategies may benefit from phase-adapted Ca/P ratios rather than a fixed ratio during the first week of life. A higher ratio may be considered during DOL 0–2, whereas a lower ratio may be considered during DOL 3–6, particularly when overall calcium and phosphorus supply is suboptimal.
- 1,622 View
- 30 Download

Review
- Recent advances in refeeding syndrome in critically ill patients: a narrative review
-
Sang Woo Ha, Suk-Kyung Hong
- Ann Clin Nutr Metab 2024;16(1):3-9. Published online April 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.1.3
-
Abstract
PDF
- Purpose: The aim of this article is to provide a narrative review of the most recent studies on refeeding syndrome (RS) in critically ill patients and to summarize recent advancements that can be referenced in the treatment of these patients.
Current concept: RS in critically ill patients is a potentially lethal nutrition-related condition leading to sudden death. Initiation of food intake after a period of fasting can trigger rapid electrolyte uptake due to increased insulin release, leading to a decline in serum electrolytes with thiamine. This depletion may cause severe complications, such as cardiac arrhythmias, respiratory failure, seizures, and even death. The incidence of RS varies significantly, ranging from 7.4%–89%. Despite updates in diagnostic criteria over time, there remains a crucial need for criteria applicable to critically ill patients with underlying disorders such as metabolic derangement and organ dysfunction. To prevent RS, it is strongly recommended to start food intake after a fast at 20%–25% of estimated goals, gradually increasing the intake over several days. Close monitoring and electrolyte supplementation—especially of phosphorus, potassium, magnesium, and thiamine—are crucial, especially in critically ill patients. If electrolyte imbalances persist, slowing down or halting the progression of nutrition should be considered.
Conclusion: Clinicians should continue their efforts to promptly identify high-risk patients and to provide prevention and treatment for RS, particularly during the initiation of nutritional therapy in critically ill patients. Developing evidence-based protocols through further well-designed research is essential for effectively managing critically ill patients at risk of RS. -
Citations
Citations to this article as recorded by
- Actualización en terapia médica nutricional del paciente críticamente enfermo: avances, desafíos y evidencia reciente
Nestor David Caicedo-Buitrago, Mateo Londoño-Pereira, Claudia Milena Ardila Melendez, Ricardo Merchán, Fernando Pereira-Paternina, Cristian Pinilla, Sonia Gamboa, Alejandra Cabral, Janeth Barbosa Barbosa, Maria del Pilar Morales, Bladimir Gil
Acta Colombiana de Cuidado Intensivo.2026; : 100612. CrossRef - Refeeding Syndrome: A Comprehensive Review of Pathophysiology, Risk Stratification and Evidence-based Management in the Intensive Care Unit
Paras Chandrakant Zunke
Vidarbha Journal of Internal Medicine.2026; 35(1): 22. CrossRef - Nutrition in the critically ill in resource-limited settings/low- and middle-income countries
Mervyn Mer, Martin W. Dünser
Current Opinion in Clinical Nutrition & Metabolic Care.2025; 28(2): 181. CrossRef - Nutritional Management of Liver Failure in the Intensive Care Unit
Zsófia Verzár, Rudolf Kiss, Csaba Pál Bálint, Annamária Pakai, Tímea Csákvári
Medicina.2025; 61(7): 1210. CrossRef - Comprehensive care of the patient with Refeeding Syndrome
Magdalena Kwiatkowska, Dominika Krupnik, Fabian Wesołek, Agnieszka Jonczyk, Łukasz Krzych
Polish Journal of Surgery.2025; 97(5): 64. CrossRef
- Actualización en terapia médica nutricional del paciente críticamente enfermo: avances, desafíos y evidencia reciente
- 65,535 View
- 1,692 Download
- 5 Crossref
Case Report
- Refeeding Syndrome after Gastrectomy in a Patient with Hypophosphatemia: A Case Report
-
Cheong Ah Oh
- Ann Clin Nutr Metab 2022;14(2):88-92. Published online December 1, 2022
- DOI: https://doi.org/10.15747/ACNM.2022.14.2.88
-
Abstract
PDF
- This study describes an 81-year-old male who was highly suspicious for refeeding syndrome (RFS) after a retrospective review of his postoperative clinical progression. This highlights the importance of clinicians’ awareness of the possibility of RFS development in surgical patients with any RFS risk factors.
- 3,898 View
- 34 Download
Original Article
- Refeeding Syndrome in Critically Ill Patients
-
Sang Woo Ha, Suk-Kyung Hong
- Ann Clin Nutr Metab 2022;14(2):72-80. Published online December 1, 2022
- DOI: https://doi.org/10.15747/ACNM.2022.14.2.72
-
Abstract
PDFSupplementary Material
- Purpose: The aim of this study is to demonstrate clinical characteristics of refeeding syndrome (RS) and clinical utility of several guidelines including American Society for Parenteral and Enteral Nutrition consensus recommendations for RS and National Institute for Clinical Excellence guidelines.
Materials and Methods: Eighty-six patients screened for RS based on two guidelines were enrolled in this study. We evaluated the severity of RS after the initiation of ‘dextrose infusion’ and ‘balanced nutrition support’ with calculation of 5-day electrolyte changes. The primary outcome was 6-month mortality and secondary outcomes were duration of intensive care unit stay in days, duration of mechanical ventilation in days, and ventilator-free days at the 28th day.
Results: We observed statistically different distributions in terms of prevalence of RS on the basis of two different start times of caloric support (P=0.021). There was no statistically significant relationship between the risk of RS and severity of RS based on both guidelines. Also, the relevance between severity of RS and outcomes was not significant in our study. In multivariable logistic regression analysis of factors associated with outcomes, the significant factor for primary outcome was the ‘patients with significant risk’ (odds ratio, 9.65; 95% confidence interval, 1.83~50.90; P=0.007).
Conclusion: We demonstrated that even initial administration of dextrose solution and propofol could cause severe RS in critically ill patients. In addition, significant risk of RS was a predictive factor for 6-month mortality. Thus, it is essential to monitor the occurrence of RS even during initial resuscitation in patients with unstable metabolism. -
Citations
Citations to this article as recorded by- Recent advances in refeeding syndrome in critically ill patients: a narrative review
Sang Woo Ha, Suk-Kyung Hong
Annals of Clinical Nutrition and Metabolism.2024; 16(1): 3. CrossRef
- Recent advances in refeeding syndrome in critically ill patients: a narrative review
- 6,699 View
- 62 Download
- 1 Crossref
Review Article
- Refeeding Syndrome
- Jeong Wook Kim
- J Clin Nutr 2015;7(1):15-22. Published online April 30, 2015
- DOI: https://doi.org/10.15747/jcn.2015.7.1.15
-
Abstract
PDF
Refeeding syndrome refers to a life-threatening shift of electrolytes and fluid with metabolic abnormalities in malnourished patients undergoing refeeding, whether orally, enterally, or parenterally. Clinical findings are fluid-balance abnormalities, abnormal glucose metabolism, hypophosphatemia, hypomagnesemia, hypokalemia and deficiencies of vitamin and trace element. Multiple organ systems including cardiac, respiratory, neurologic, renal, hematologic, and gastrointestinal can be affected. When recognized in a timely manner, these complications can be easily and successfully prevented and treated. Four factors appear fundamental: early identification of patients at risk, correction of abnormalities before refeeding, close monitoring during refeeding, and an appropriate feeding regimen.
-
Citations
Citations to this article as recorded by- Be Biologist: Basic Knowledge for Biologist Which No One Told 4
Jong-Eun Kim
Journal of Biotechnology and Bioindustry.2024; 12: 61. CrossRef - Refeeding Syndrome after Gastrectomy in a Patient with Hypophosphatemia: A Case Report
Cheong Ah Oh
Annals of Clinical Nutrition and Metabolism.2022; 14(2): 88. CrossRef - Effects of Early Phosphorus Intake on Respiratory Distress in Extremely Low-Birth-Weight Infants
Hye Jung Bae, Hyung Woo Yoon, Moon Jin Kim, Ae Hee Jung, Sun Hoi Jung, Hyeon Joo Hahn, Yun Hee Jo, Yoon Sook Cho, Ee-Kyung Kim, Seung Han Shin, In Gyu Song, Seung Hyun Shin
Neonatal Medicine.2019; 26(3): 155. CrossRef
- Be Biologist: Basic Knowledge for Biologist Which No One Told 4
- 5,767 View
- 66 Download
- 3 Crossref
 First
First Prev
Prev

