 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Search
- Page Path
- HOME > Search
Guideline
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part III. preparation of enteral nutrition formulas
-
In Seok Lee
 , Ye Rim Chang, Bo-Eun Kim, Youn Soo Cho, Sung-Sik Han, Eunjung Kim, Hyunjung Kim, Jae Hak Kim, Jeong Wook Kim, Sung Shin Kim, Eunhee Kong, Ja Kyung Min, Chi-Min Park, Jeongyun Park, Seungwan Ryu, Kyung Won Seo, Jung Mi Song, Minji Seok, Eun-Mi Seol, Jinhee Yoon, Jeong-Meen Seo, for the KSPEN Enteral Nutrition Committee
, Ye Rim Chang, Bo-Eun Kim, Youn Soo Cho, Sung-Sik Han, Eunjung Kim, Hyunjung Kim, Jae Hak Kim, Jeong Wook Kim, Sung Shin Kim, Eunhee Kong, Ja Kyung Min, Chi-Min Park, Jeongyun Park, Seungwan Ryu, Kyung Won Seo, Jung Mi Song, Minji Seok, Eun-Mi Seol, Jinhee Yoon, Jeong-Meen Seo, for the KSPEN Enteral Nutrition Committee - Ann Clin Nutr Metab 2026;18(1):3-9. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.26.0046
-
 Abstract
Abstract
 PDF
PDF - Purpose
This guideline was developed to provide evidence-based recommendations for the safe preparation and handling of enteral nutrition (EN) formulas in order to improve patient safety and promote standardized clinical practice in Korea.
Methods
The key questions addressed the selection of open versus closed feeding systems, the safe preparation and handling of EN formulas, precautions related to blenderized tube feeding (BTF), and essential labeling requirements. Recommendations were drafted and refined through multidisciplinary expert consensus under the auspices of the Korean Society for Parenteral and Enteral Nutrition (KSPEN).
Results
The choice of feeding system should be determined according to the patient’s condition, risk of infection, and anticipated duration of feeding. Closed feeding systems are recommended because they reduce contamination risk and nursing workload, whereas open feeding systems require strict adherence to aseptic technique. For open or reconstituted EN formulas, hang time at room temperature should not exceed 4 hours, whereas closed feeding systems should follow the manufacturer’s recommended hang time. For BTF, administration time should be limited to 2 hours to minimize bacterial growth, and their use is contraindicated in medically unstable or immunocompromised patients. Accurate labeling, including patient identifiers, formula information, administration route, and hang time, is essential to prevent administration errors.
Conclusion
These guidelines provide a practical framework for the safe preparation and management of EN formulas. Adherence to standardized preparation protocols, including appropriate feeding system selection and strict hygiene practices, is essential for reducing complications and improving the safety of EN therapy.
- 2,437 View
- 73 Download

Original Articles
- Association between the calcium-to-phosphorus ratio and early hypophosphatemia in preterm infants receiving parenteral nutrition in Korea: a retrospective cohort study
-
Miseon Han, Jin Ok Kyun, Yoong-A Suh, Jang Hoon Lee
- Ann Clin Nutr Metab 2026;18(1):44-53. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0039
-
 Graphical Abstract
Abstract
PDF
Graphical Abstract
Abstract
PDF Supplementary Material
Supplementary Material - Purpose
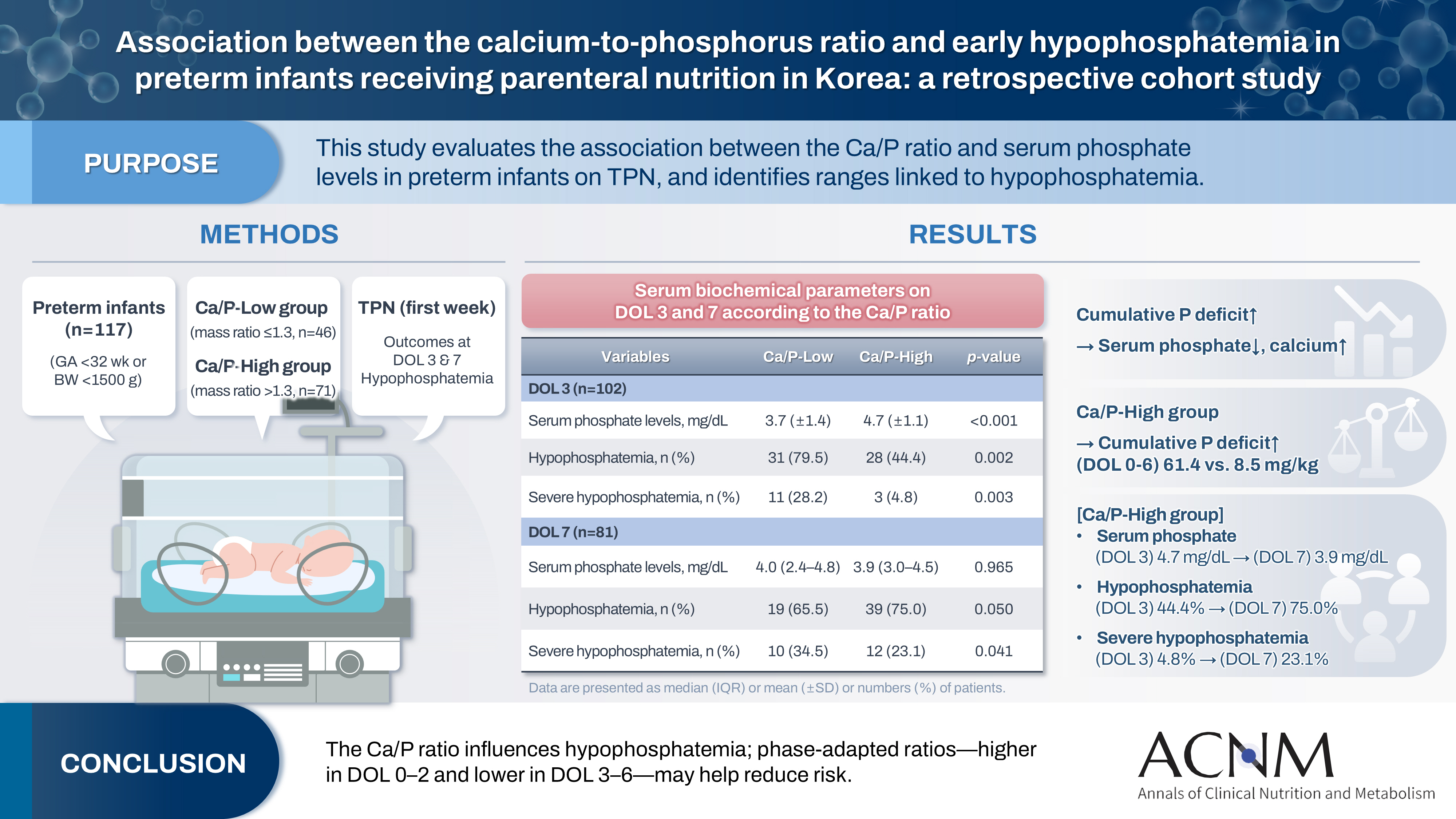
This study aimed to evaluate the association between the calcium-to-phosphorus (Ca/P) ratio and serum phosphate levels in preterm infants receiving total parenteral nutrition (TPN) and to explore Ca/P ratio ranges associated with hypophosphatemia.
Methods
We retrospectively reviewed the medical records of preterm infants admitted to the neonatal intensive care unit at Ajou University Hospital between January 2022 and June 2024. The review focused on TPN composition and serum electrolyte changes during the first week of life. Based on the cumulative Ca/P ratio during this period, infants were categorized into two groups: Ca/P-Low (mass ratio ≤1.3) and Ca/P-High (mass ratio >1.3).
Results
A total of 117 preterm infants were included in the analysis (Ca/P-Low group, n=46; Ca/P-High group, n=71). During the first week of life, the cumulative phosphorus deficit was significantly greater in the Ca/P-High group (61.4 mg/kg vs. 8.5 mg/kg; P<0.001). By day of life (DOL) 7, both hypophosphatemia and severe hypophosphatemia had increased markedly in the Ca/P-High group compared with DOL 3. In the Ca/P-High group, the incidence of hypophosphatemia increased from 44.4% on DOL 3 to 75.0% on DOL 7, while the incidence of severe hypophosphatemia increased from 4.8% to 23.1%.
Conclusion
These findings suggest that parenteral nutrition strategies may benefit from phase-adapted Ca/P ratios rather than a fixed ratio during the first week of life. A higher ratio may be considered during DOL 0–2, whereas a lower ratio may be considered during DOL 3–6, particularly when overall calcium and phosphorus supply is suboptimal.
- 1,687 View
- 31 Download
- Association of soy oil-based lipid injectable emulsion with early body weight loss after minimally invasive esophagectomy in Japan: a retrospective cohort study
-
Tomonori Narita
 , Kazuhiko Fukatsu, Kenichi Kono, Satoshi Murakoshi, Reo Inoue, Midori Noguchi, Nana Matsumoto, Shoh Yajima, Koichi Yagi, Yoshifumi Baba
, Kazuhiko Fukatsu, Kenichi Kono, Satoshi Murakoshi, Reo Inoue, Midori Noguchi, Nana Matsumoto, Shoh Yajima, Koichi Yagi, Yoshifumi Baba - Ann Clin Nutr Metab 2026;18(1):34-43. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0030
-
Graphical Abstract
Abstract
PDFSupplementary Material
- Purpose
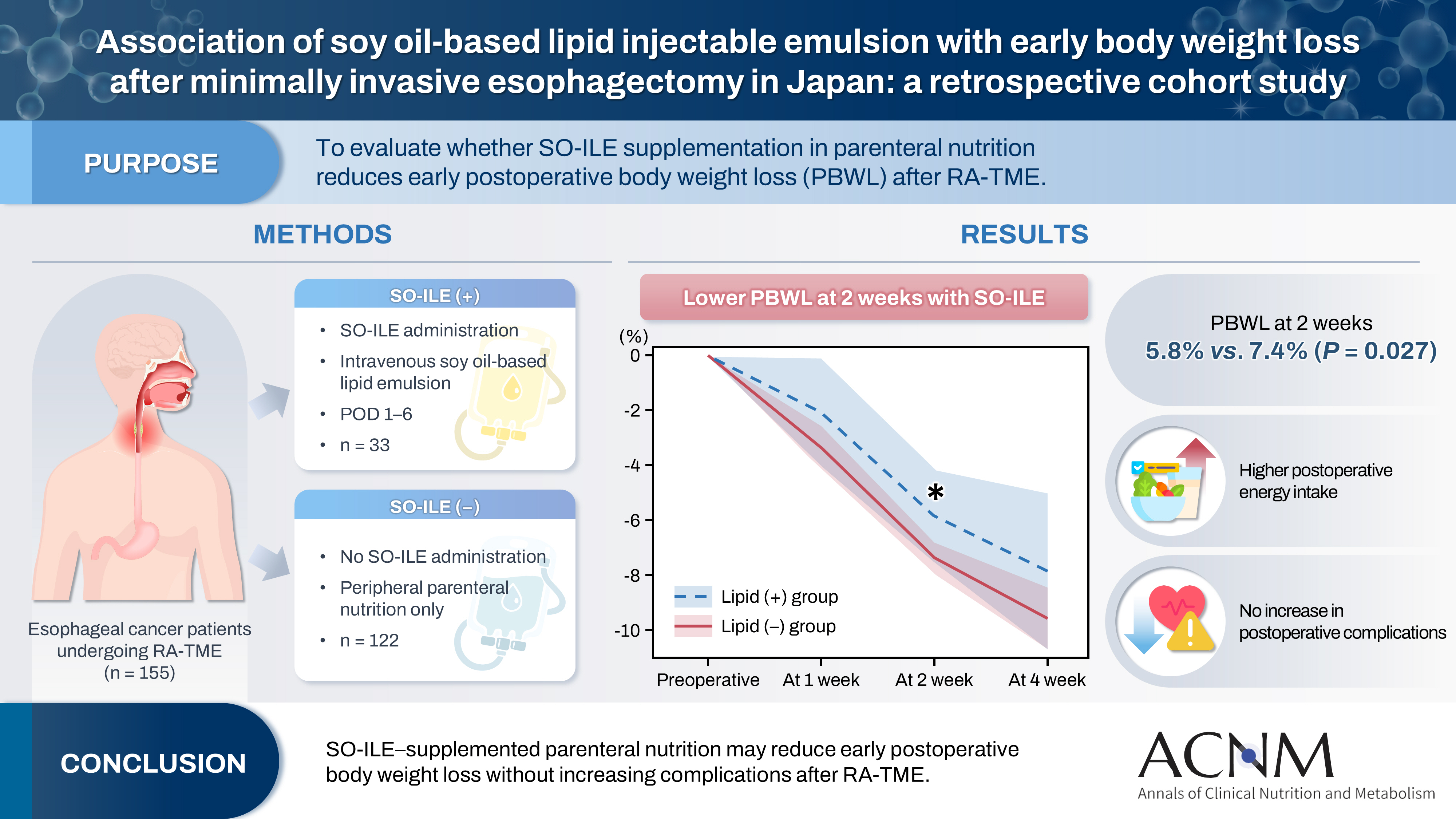
Postoperative body weight loss (PBWL) is associated with poor long-term outcomes following esophagectomy for esophageal cancer, underscoring the critical importance of perioperative nutritional management. Although minimally invasive procedures, such as robot-assisted radical transmediastinal esophagectomy (RA-TME), have become increasingly prevalent, perioperative nutritional strategies have received comparatively limited attention. This study evaluated the impact of soy oil-based injectable lipid emulsion (SO-ILE) on PBWL in patients undergoing RA-TME.
Methods
We retrospectively analyzed 155 patients who underwent RA-TME for esophageal or esophagogastric junction cancer at our hospital between 2011 and 2022. Patients were divided into two groups: the lipid (+) group (n=33), which received SO-ILE between postoperative days 1 and 6, and the lipid (–) group (n=122), which did not receive SO-ILE. Oral or enteral nutrition was withheld until postoperative day 6. Nutrient intake, postoperative outcomes, and nutritional status were compared between the two groups.
Results
Patient backgrounds, surgical outcomes, and postoperative complication rates were similar between the two groups. However, patients in the lipid (+) group received significantly greater total energy and nutrient intake. PBWL at 2 weeks after surgery was significantly lower in the lipid (+) group than in the lipid (–) group (5.8% vs. 7.4%; P=0.027). Univariate analysis showed that absence of SO-ILE administration was the only significant risk factor for PBWL greater than 5% at 2 weeks after RA-TME (P=0.038).
Conclusion
SO-ILE may have the potential to mitigate early PBWL after RA-TME.
- 1,669 View
- 19 Download
Review
- Effectiveness of perioperative rehabilitation and nutrition in esophageal cancer: a narrative review
-
Ryoma Haneda, Yuki Sakai, Kenichi Sekimori, Tomohiro Murakami, Eisuke Booka, Tomohiro Matsumoto, Hirotoshi Kikuchi, Yoshihiro Hiramatsu, Hiroya Takeuchi
- Ann Clin Nutr Metab 2026;18(1):18-26. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0021
-
Abstract
PDF
- Purpose
Esophageal cancer surgery requires robust perioperative management to reduce its high rate of complications. This review evaluates the clinical utility of comprehensive exercise and nutritional therapy, with a specific focus on initiatives led by the multidisciplinary Hamamatsu Perioperative Care Team (HOPE), established at Hamamatsu University Hospital to optimize patient safety and postoperative recovery outcomes.
Current concept
The HOPE protocol involves a diverse team, including surgeons, nurses, pharmacists, and dietitians, who collaboratively implement a multifaceted perioperative care bundle. These interventions include strict smoking cessation, intensive oral care, and immunonutrition incorporating n-3 fatty acids. A distinctive feature of this program is the integration of patient-reported treatment diaries and wearable fitness tracking devices (WFTs) to visualize daily activity, thereby helping to sustain patient motivation. Preoperative rehabilitation focuses on preventing sarcopenia through combined aerobic and resistance training, while postoperative care emphasizes immediate enteral nutrition and early mobilization. Retrospective analyses demonstrated that HOPE implementation reduced Clavien-Dindo grade III or higher infectious complications, pneumonia and surgical site infections, compared with historical controls. In addition, a propensity score–matched analysis showed that WFT users experienced lower pneumonia rates, shorter hospital stays, and better preservation of nutritional markers, including albumin and transthyretin, during the recovery phase compared with non-users.
Conclusion
The HOPE strategy illustrates that combining standard nutritional support and exercise therapy with digital tools enables individualized rehabilitation. This integrated approach reduces morbidity and preserves function, strongly suggesting that incorporation of wearable technology into established surgical care protocols represents a strategy for improving long-term outcomes in high-risk cancer patients.
- 1,240 View
- 18 Download
Guideline
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part II. selection and initiation of enteral feeding routes
-
Ja Kyung Min, Ye Rim Chang, Bo-Eun Kim, In Seok Lee, Jung Mi Song, Hyunjung Kim, Jae Hak Kim, Kyung Won Seo, Sung Shin Kim, Chi-Min Park, Jeongyun Park, Eunjung Kim, Eunmi Sul, Sung-Sik Han, Jeong Wook Kim, Seungwan Ryu, Minji Seok, Jinhee Yoon, Eunhee Kong, Youn Soo Cho, Jeong Meen Seo, for KSPEN Enteral Nutrition Committee
- Ann Clin Nutr Metab 2025;17(3):165-171. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0037
-
Abstract
PDF
- Purpose
We developed evidence-based recommendations for selecting and initiating the enteral nutrition (EN) delivery route in adult and pediatric patients to improve safety and standardize practice in Korea.
Methods
Key questions covered feeding tube selection, methods to verify tube placement, confirmation in pediatric patients, and timing of EN following percutaneous endoscopic gastrostomy (PEG). Recommendations were drafted and refined through multidisciplinary expert consensus under the Korean Society for Parenteral and Enteral Nutrition (KSPEN).
Results
Feeding tube selection should be based on gastrointestinal anatomy, function, and expected EN duration. Short-term feeding is recommended with nasogastric or orogastric tubes, whereas long-term feeding should use percutaneous or surgical routes such as PEG. Tube position must always be verified before use, preferably with radiography or pH testing; auscultation alone is unreliable and should not be used. In pediatric patients, radiographic confirmation remains the gold standard, although pH testing and insertion-length assessment may be considered when imaging is not feasible. After PEG, EN can be initiated safely within 4 hours in both adults and children without increasing complications if trained staff monitor for leakage or infection.
Conclusion
This guideline offers a structured framework for safe and timely EN tailored to patient characteristics. Early verification and multidisciplinary collaboration help reduce complication, improving outcomes of EN therapy.
- 2,467 View
- 103 Download
Interesting image
- Penetration of a nasogastric tube by a stylet during insertion
-
Akihide Takami, Haruka Tsuji, Kazuya Omura
- Ann Clin Nutr Metab 2025;17(3):210-211. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0029
- 1,185 View
- 18 Download
Original Articles
- Perioperative nutritional practices and pediatric nutrition support team implementation in Korea: a cross-sectional study
-
Dayoung Ko, Honam Hwang, Hee-Beom Yang, Joong Kee Youn, Hyun-Young Kim
- Ann Clin Nutr Metab 2025;17(3):181-187. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0027
-
Graphical Abstract
Abstract
PDFSupplementary Material
- Purpose
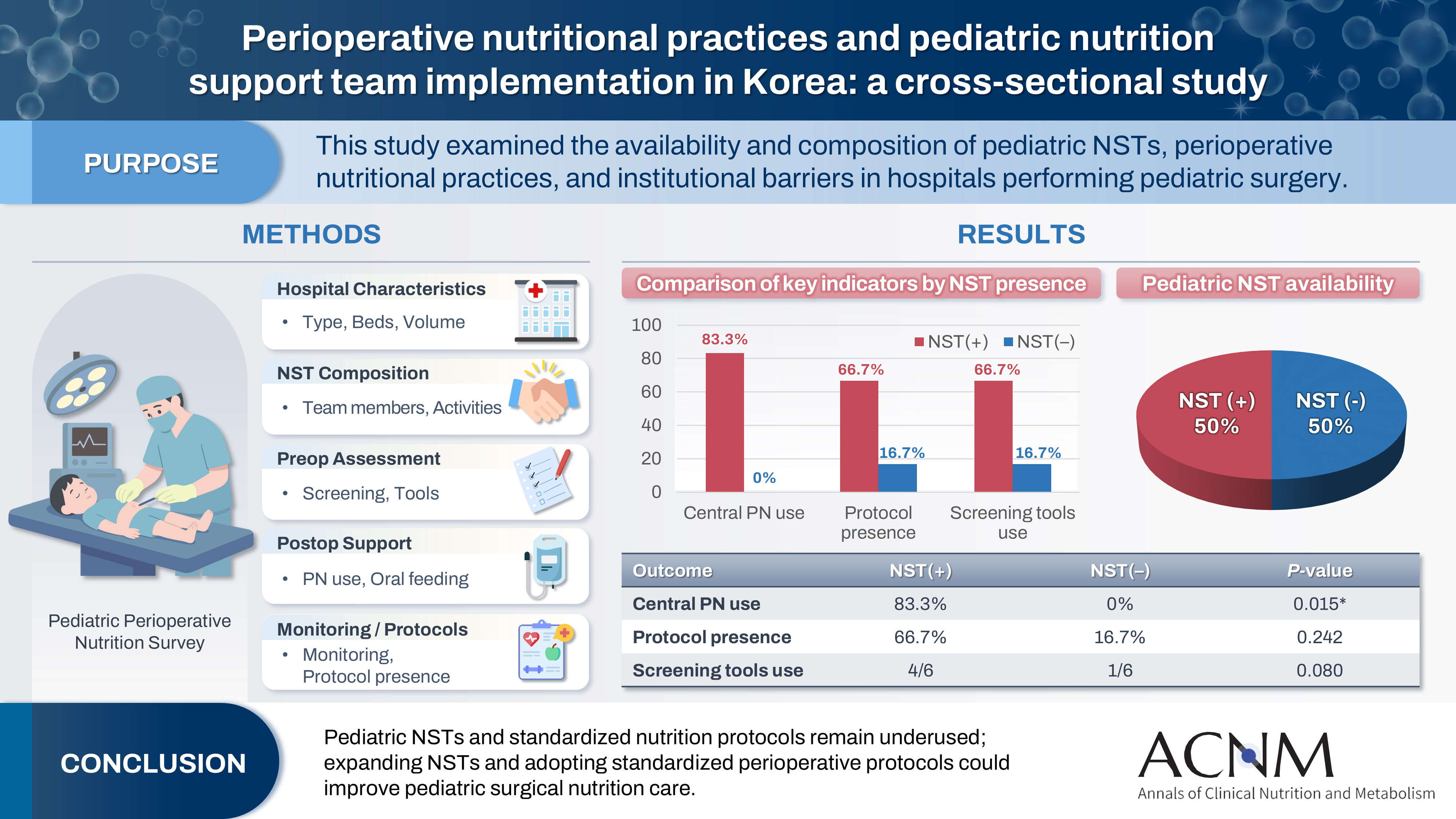
Pediatric surgical patients are vulnerable to perioperative malnutrition, yet standardized nutritional care and structured nutrition support team (NST) involvement remain inconsistent across institutions. Although multidisciplinary nutritional support has gained increasing attention, data on pediatric NST practices within surgical settings in Korea are limited. This study examined the availability and composition of pediatric NSTs, perioperative nutritional practices, and barriers in hospitals performing pediatric surgery.
Methods
A nationwide cross-sectional survey was conducted among tertiary and secondary hospitals that perform pediatric surgery in Korea. The questionnaire assessed hospital characteristics, the presence and composition of pediatric NSTs, perioperative nutritional screening and support practices, monitoring protocols.
Results
A total of 12 hospitals participated. Although all were high-capacity institutions, only half reported having a pediatric NST. Routine preoperative nutritional screening was performed in 50% of hospitals, and validated tools such as Screening Tool for the Assessment of Malnutrition in Pediatrics (STAMP) and Pediatric Yorkhill Malnutrition Score (PYMS) were used in 41.7%. Hospitals with a pediatric NST more frequently had institutional protocols for nutritional evaluation (66.7% vs. 16.7%) and were more likely to administer central venous parenteral nutrition postoperatively (83.3% vs. 0%, P=0.015). Enhanced Recovery After Surgery protocols were implemented in only two hospitals (16.7%). Major barriers to pediatric NST operation included insufficient staffing and time constraints.
Conclusion
Pediatric NSTs and standardized perioperative nutrition protocols remain underutilized in Korean surgical centers. Institutions with a pediatric NST demonstrated more structured nutritional practices. Expanding NST infrastructure and establishing standardized perioperative protocols for pediatric surgical patients may enhance the quality and consistency of nutritional care.
- 2,552 View
- 43 Download
- Impact of tube feeding after pancreaticoduodenectomy on nutritional intake and status: a retrospective cohort study in Japan
-
Masaharu Ishida, Masahiro Iseki, Shuichiro Hayashi, Aya Noguchi, Hideaki Sato, Shingo Yoshimachi, Akiko Kusaka, Mitsuhiro Shimura, Shuichi Aoki, Daisuke Douchi, Takayuki Miura, Shimpei Maeda, Masamichi Mizuma, Kei Nakagawa, Takashi Kamei, Michiaki Unno
- Ann Clin Nutr Metab 2025;17(3):203-209. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0020
-
Graphical Abstract
Abstract
PDF
- Purpose
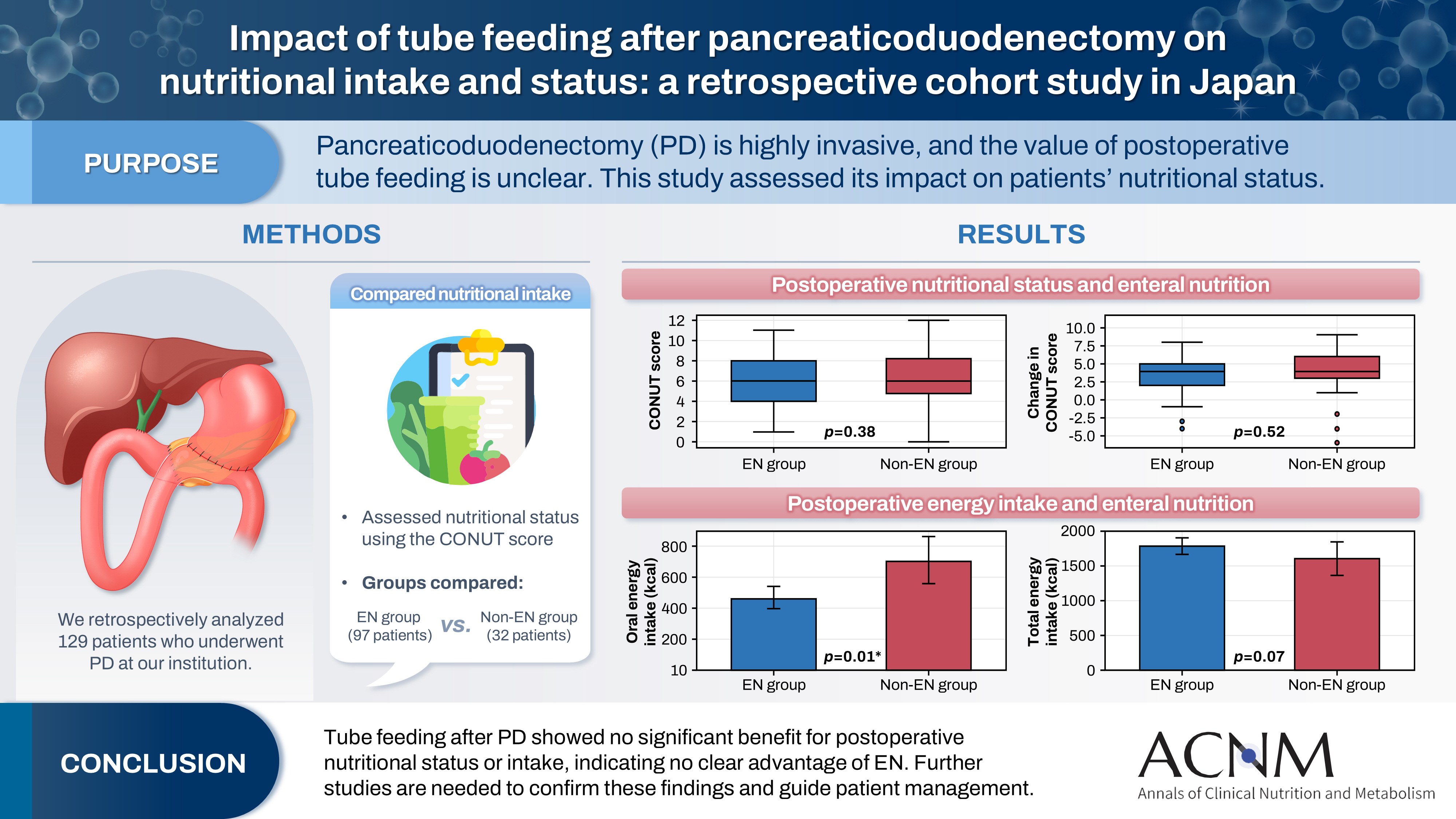
Pancreaticoduodenectomy (PD) is one of the most invasive procedures in gastrointestinal surgery. However, the clinical significance of postoperative tube feeding remains unclear. This study investigated the impact of enteral nutrition (EN) on the postoperative nutritional status of patients undergoing PD.
Methods
We retrospectively analyzed 129 patients who underwent PD at Tohoku University Hospital. Nutritional intake and status, evaluated using the Controlling Nutritional Status score, were compared between two groups: an EN group (97 patients) and a non-EN group (32 patients).
Results
There were no significant differences between the two groups in age, sex, body mass index, underlying diseases, operative duration, blood loss, postoperative pancreatic fistula, postoperative complications, delayed gastric emptying, or length of hospital stay. Although the EN group showed improvements in nutritional status both at discharge and compared with preoperative values, none of these changes reached statistical significance. Oral caloric intake was significantly higher in the non-EN group (P=0.01). In contrast, total energy intake was higher in the EN group, but this difference did not reach statistical significance (P=0.07).
Conclusion
Tube feeding after PD did not significantly influence postoperative nutritional status or overall nutritional intake. These findings suggest that EN offers no clear advantage over other approaches; however, further research is warranted to validate these results, refine existing guidelines, and optimize postoperative patient management.
- 1,570 View
- 22 Download
Review
- Improving the usability of lipid emulsions and optimizing their user-friendliness: a narrative review
-
Keisuke Kubota, Natsuko Ichikawa, Kazuhiro Isoda, Misato Enomoto, Miyoko Kosugi, Mari Tanabe, Naoya Sakuraba, Sayuri Endo, Atsushi Suzuki, Masanori Hashimoto
- Ann Clin Nutr Metab 2025;17(2):104-113. Published online August 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0015
-
Abstract
PDF
- Purpose
Reluctance to administer lipid emulsions to patients receiving treatment, or as recommended by a nutritional support team, often stems from various restrictions or concerns about potential adverse effects. This paper aims to discuss the appropriate clinical use of lipid emulsions to enhance both patient safety and convenience.
Current concept
We conducted a literature review to assess the importance of nutritional therapy and nutritional intervention, the advantages and disadvantages of lipid-emulsion administration, the current situation in Japan, and differences between lipid formulations. Here, we address issues regarding lipid-emulsion use, including: administration rate, drug mixing, administration in critically ill patients, and early postoperative use. Our findings suggest the following solutions to each issue: although a rate below 0.1 g/kg/hr is generally recommended, faster administration is possible if needed, depending on the case; administration via a piggy tube to basic infusion formulations is unproblematic; second- and third-generation fat emulsions are safe for critically ill patients, though soybean oil should be used with caution; and while fat emulsion administration is feasible immediately after surgery, due to endogenous energy mobilization, it is preferable to initiate administration from the third to fourth postoperative day.
Conclusion
The provisional conclusions of this study are as follows: the introduction of medium-chain triglyceride formulations and fish oil (second- and third-generation lipid emulsions), which are not yet available in Japan, is urgently needed; and individualized administration is essential due to substantial interindividual variability in lipid emulsion usage. -
Citations
Citations to this article as recorded by
- Impact of soybean oil lipid emulsion on clinical outcomes in critically ill pediatric patients
Yuki Yamano, Yoshiyuki Shimizu, Yu Inata, Takeshi Hatachi, Yuri Etani
Clinical Nutrition ESPEN.2026; 72: 102907. CrossRef
- Impact of soybean oil lipid emulsion on clinical outcomes in critically ill pediatric patients
- 8,228 View
- 53 Download
- 1 Crossref
Original Article
- Effects of enteral nutrition formulas with varying carbohydrate amounts on glycemic control in diabetic mice
-
Yukari Miki, Kazuo Hino
- Ann Clin Nutr Metab 2025;17(1):85-93. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0006
-
Abstract
PDF
- Purpose
This study evaluated the effects of an 8‑week liquid diets with different carbohydrate contents–64% energy in HINE E‑Gel (ST) and 50% energy in HINE E‑Gel LC (LC)–on glycemic control and nutritional status in a mouse model of type 2 diabetes mellitus (db/db mice). The objective was to determine whether reducing carbohydrate intake within the Dietary Reference Intakes for Japanese people improves glycemic control indices, addressing the evidence gap in regarding the long‑term safety and efficacy of low‑carbohydrate enteral nutrition in patients with diabetes.
Methods
db/db mice (n=10 per group) and non‑diabetic db/m mice (n=4) as controls were fed ST, LC, or AIN‑93G diets ad libitum for 8 weeks. The diets primarily differed in carbohydrate content (64% in ST vs. 50% in LC). Blood glucose and glycated hemoglobin (HbA1c), plasma glucose and glycoalbumin, organ weights, and renal function markers were measured weekly or at 4 and 8 weeks. Histopathological examinations of the liver and kidneys were performed at 8 weeks.
Results
At 8 weeks, the LC group showed significantly lower plasma glucose (P=0.0051) and glycoalbumin (P=0.0013) levels compared to the ST group, with a trend toward lower HbA1c (P=0.0514). Although body weight was significantly higher in the LC group (P=0.0038), there were no significant differences between the ST and LC groups in caloric intake, renal function, or histopathological findings.
Conclusion
Reducing carbohydrate intake to 50% of total energy within dietary guidelines may improve glycemic control in diabetic mice, suggesting the need for further long‑term evaluation for clinical applications. -
Citations
Citations to this article as recorded by- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
Ye Rim Chang
Ann Clin Nutr Metab.2025; 17(2): 95. CrossRef
- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
- 2,763 View
- 34 Download
- 1 Crossref
Review
- Perioperative nutritional management to improve long-term outcomes in critically ill perioperative organ transplant patients: a narrative review
-
Toshimi Kaido
- Ann Clin Nutr Metab 2025;17(1):18-24. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0005
-
Abstract
PDF
- Purpose
This review examines the significance of perioperative nutritional management in organ transplantation, with a particular focus on liver transplantation. Organ transplant recipients often experience malnutrition and sarcopenia due to nutritional and metabolic abnormalities associated with organ dysfunction. Because transplantation is a highly invasive procedure, optimizing perioperative nutritional care is critical for improving short-term outcomes and reducing postoperative infection-related mortality.
Current concept
Recent clinical investigations have shown that liver transplant recipients, who are frequently afflicted with end-stage liver disease and uncompensated cirrhosis, are particularly vulnerable to protein-energy malnutrition and secondary sarcopenia. Our analysis identified low pre-transplant nutritional status and the absence of preoperative branched-chain amino acid supplementation as independent risk factors for post-transplant sepsis. In response, we developed a customized nutritional therapy protocol that incorporates precise body composition analysis, serial measurements of biochemical markers (including prealbumin, zinc, and the branched-chain amino acid/tyrosine ratio), and targeted supplementation with branched-chain amino acids, zinc acetate, and synbiotics. Early initiation of enteral nutrition coupled with postoperative rehabilitative interventions resulted in improved outcomes. In addition, stratified body composition parameters correlated with survival differences and informed revised transplantation criteria.
Conclusion
Tailored perioperative nutritional management and rehabilitative strategies are essential for improving early postoperative outcomes in liver transplantation. These findings underscore the need for proactive nutritional assessment and intervention, which may represent a breakthrough in transplant prognosis. Future research should refine nutritional protocols and integrate novel biomarkers, while education and interdisciplinary collaboration remain crucial for enhancing transplant outcomes and reducing complications. -
Citations
Citations to this article as recorded by- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
Ye Rim Chang
Ann Clin Nutr Metab.2025; 17(2): 95. CrossRef
- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
- 11,012 View
- 132 Download
- 1 Crossref
Original Article
- The enteral feeding tube access route in esophageal cancer surgery in Japan: a retrospective cohort study
-
Hiroyuki Kitagawa, Keiichiro Yokota, Tsutomu Namikawa, Kazuhiro Hanazaki
- Ann Clin Nutr Metab 2025;17(1):58-65. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0003
-
Graphical Abstract
Abstract
PDF
- Purpose
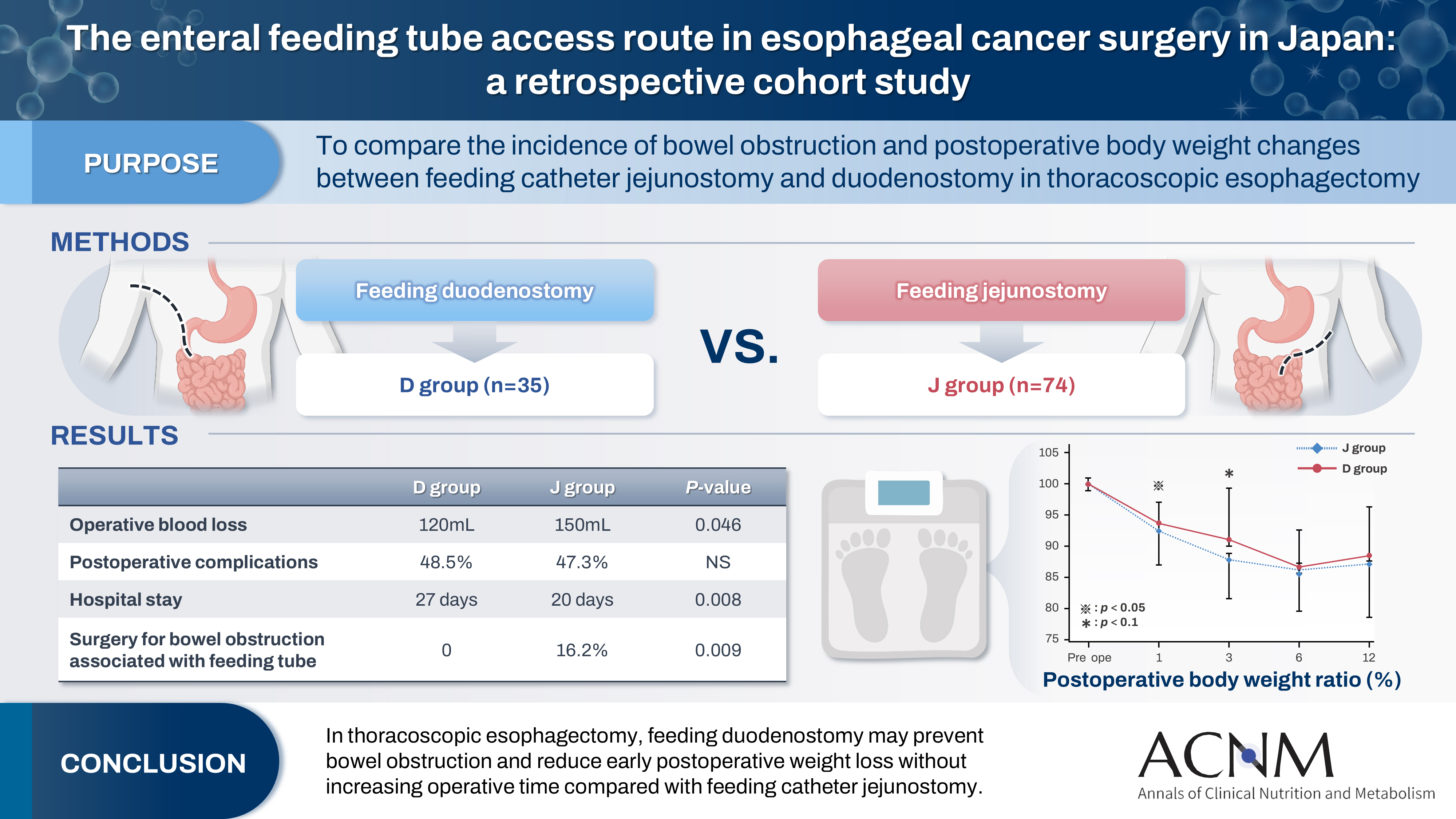
Feeding catheter jejunostomy is a useful access route for early enteral nutrition during esophageal cancer surgery. However, it may lead to postoperative bowel obstruction associated with feeding jejunostomy (BOFJ). To prevent BOFJ, we introduced feeding catheter duodenostomy via the round ligament in 2018. This study aimed to compare the incidence of BOFJ and postoperative body weight changes between feeding catheter jejunostomy and duodenostomy.
Methods
A total of 109 patients who underwent thoracoscopic esophagectomy and gastric tube reconstruction for esophageal cancer at Kochi Medical School Hospital between March 2013 and November 2020 were included. Preoperative patient characteristics (age, sex, preoperative weight, body mass index, cancer stage, and preoperative treatment), surgical outcomes (operative time, blood loss, and postoperative complications [wound infection, pneumonia, anastomotic leakage, BOFJ]), and body weight changes at 1, 3, 6, and 12 months post-surgery were compared between the jejunostomy (J) and duodenostomy (D) groups.
Results
The D group consisted of 35 patients. No significant differences were observed between the groups regarding age, sex, weight, body mass index, cancer stage, operative time, postoperative complications, or duration of tube placement. However, the D group had a significantly lower rate of preoperative chemotherapy (45.7% vs. 78.4%, P=0.001) and lower operative blood loss (120 mL vs. 150 mL, P=0.046) than the J group. All 12 cases of BOFJ occurred in the J group. Furthermore, the D group experienced a significantly lower weight loss ratio at 1 month postoperatively (93.9% vs. 91.8%, P=0.039).
Conclusion
In thoracoscopic esophagectomy, feeding duodenostomy may prevent bowel obstruction and reduce early postoperative weight loss without increasing operative time compared with feeding catheter jejunostomy. -
Citations
Citations to this article as recorded by- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
Ye Rim Chang
Ann Clin Nutr Metab.2025; 17(2): 95. CrossRef
- Strengthening collaboration: introducing the contributions of Japanese Society for Surgical Metabolism and Nutrition to Annals of Clinical Nutrition and Metabolism
- 4,522 View
- 44 Download
- 1 Crossref
Guideline
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part I. prescribing enteral nutrition orders
-
Ye Rim Chang, Bo-Eun Kim, In Seok Lee, Youn Soo Cho, Sung-Sik Han, Eunjung Kim, Hyunjung Kim, Jae Hak Kim, Jeong Wook Kim, Sung Shin Kim, Eunhee Kong, Ja Kyung Min, Chi-Min Park, Jeongyun Park, Seungwan Ryu, Kyung Won Seo, Jung Mi Song, Minji Seok, Eun-Mi Seol, Jinhee Yoon, Jeong Meen Seo, for KSPEN Enteral Nutrition Committee
- Ann Clin Nutr Metab 2025;17(1):3-8. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0002
-
Abstract
PDF
- Purpose
This study aimed to develop a comprehensive practical guide for enteral nutrition (EN) designed to enhance patient safety and reduce complications in Korea. Under the leadership of the Korean Society for Parenteral and Enteral Nutrition (KSPEN), the initiative sought to standardize EN procedures, improve decision-making, and promote effective multidisciplinary communication.
Methods
The KSPEN EN committee identified key questions related to EN practices and organized them into seven sections such as prescribing, delivery route selection, formula preparation, administration, and quality management. Twenty-one experts, selected based on their expertise, conducted a thorough literature review to formulate evidence-based recommendations. Drafts underwent peer review both within and across disciplines, with final revisions completed by the KSPEN Guideline Committee. The guide, which will be published in three installments, addresses critical elements of EN therapy and safety protocols.
Results
The practical guide recommends that EN orders include detailed elements and advocates the use of electronic medical records for communication. Standardized prescription forms and supplementary safety measures are outlined. Review frequency is adjusted according to patient condition—daily for critically ill or unstable patients and as dictated by institutional protocols for stable patients. Evidence indicates that adherence to these protocols reduces mortality, complications, and prescription errors.
Conclusion
The KSPEN practical guide offers a robust framework for the safe delivery of EN tailored to Korea’s healthcare context. It emphasizes standardized protocols and interdisciplinary collaboration to improve nutritional outcomes, patient safety, and operational efficiency. Rigorous implementation and monitoring of adherence are critical for its success. -
Citations
Citations to this article as recorded by- Rationale for Determining Energy Requirement in Hospitalized Patients: A Narrative Review
Suk-Kyung Hong, Kyung Mo Kim
Pediatric Gastroenterology, Hepatology & Nutrition.2026; 29(3): 212. CrossRef - Bridging evidence and clinical practice: a practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition
Suk-Kyung Hong
Ann Clin Nutr Metab.2025; 17(1): 1. CrossRef
- Rationale for Determining Energy Requirement in Hospitalized Patients: A Narrative Review
- 9,173 View
- 237 Download
- 2 Crossref
Original Articles
- Comparison of efficacy of enteral versus parenteral nutrition in patients after esophagectomy in Malaysia: a prospective cohort study
-
Ramizah Mohd Shariff
 , Sze Chee Tee, Shukri Jahit Mohammad, Khei Choong Khong
, Sze Chee Tee, Shukri Jahit Mohammad, Khei Choong Khong - Ann Clin Nutr Metab 2025;17(1):41-49. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.24.016
-
Graphical Abstract
Abstract
PDF
- Purpose
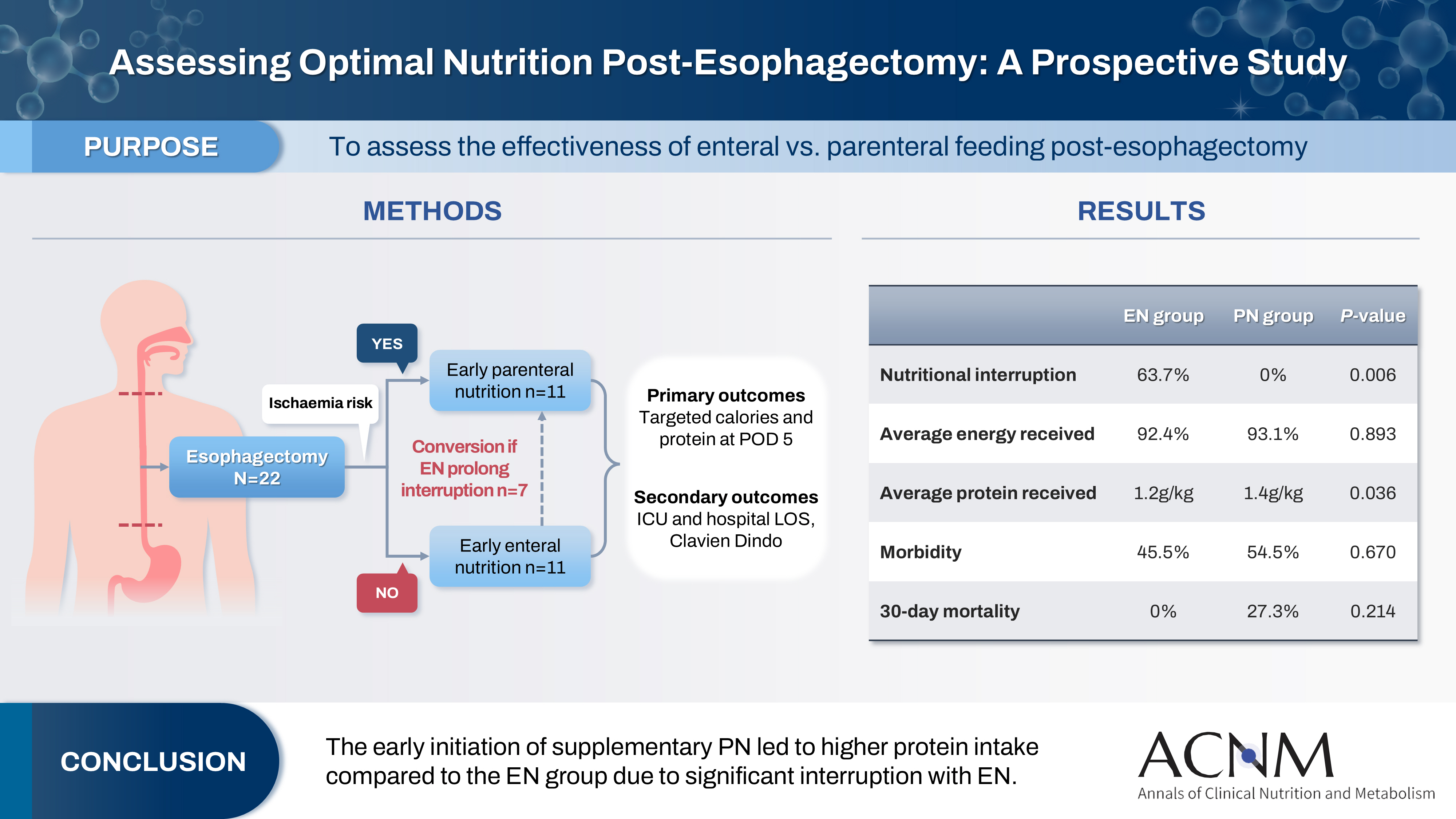
This study aims to assess the effectiveness of enteral versus parenteral feeding in patients after esophagectomy.
Methods
This a prospective cohort study of post-esophagectomy intensive care unit (ICU) patients over 12 months in the National Cancer Institute, Malaysia. Early enteral feeding followed the Enhanced Recovery After Surgery protocol, and parenteral nutrition (PN) was considered if there was a risk for conduit ischemia. It compared the effectiveness of enteral versus PN following esophagectomy, and assessed the correlations between biochemical nutritional markers and hospital lengths of stay or ventilation days.
Results
It included two cohorts receiving PN (n=11) or enteral nutrition (EN) (n=11) following elective esophagectomy. Preoperative weight, body mass index, and Subjective Global Assessment were higher in the EN group (P=0.033, P=0.021, P=0.031, respectively). Nutritional interruption occurred more frequently in the EN group (63.7%) compared to the PN group (P=0.001). Mean levels of energy and protein received were 93.1 kcal/kg and 1.4 g/kg for PN versus 92.4 kcal/kg and 1.2 g/kg for EN (P=0.893, P=0.036). The median lengths of ICU stay (P=0.688) and postoperative stay (P=0.947) between groups showed no significant difference. In addition, 30-day mortality (P=0.214) and other postoperative complications (P>0.05) were comparable in the two groups.
Conclusion
Early initiation of supplementary PN due to significant interruption in EN led to higher protein intake compared to the EN group. However, there were no significant differences in postoperative outcomes, including 30-day mortality, ICU length of stay, and ventilation days. PN ensures adequate nutritional intake, especially in terms of protein delivery, without adversely affecting postoperative recovery and clinical outcomes. -
Citations
Citations to this article as recorded by- Optimizing nutritional support in upper gastrointestinal surgery: A comprehensive review of feeding jejunostomy techniques and outcomes
Ioana Alexandra Prisacariu, Konstantinos Eleftherios Koumarelas, Konstantinos Argyriou, Alexandros Charalabopoulos, Grigorios Christodoulidis
World Journal of Gastrointestinal Surgery.2025;[Epub] CrossRef
- Optimizing nutritional support in upper gastrointestinal surgery: A comprehensive review of feeding jejunostomy techniques and outcomes
- 7,523 View
- 88 Download
- 1 Crossref
- The impact of nutritional intervention by a nutrition support team on extrauterine growth restriction in very low birth weight infants in Korea: a retrospective cohort study
-
Seung Yun Lee, Hye Su Hwang, Waonsun Im, Hyojoung Kim, Mi Lim Chung
- Ann Clin Nutr Metab 2024;16(3):149-157. Published online December 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.3.149
-
Abstract
PDF
- Purpose: Achieving proper weight gain through adequate nutrition is critically important in very low birth weight (VLBW) infants. Despite recent active nutritional interventions, growth restriction is still common in VLBW infants. We aimed to determine whether nutritional intervention by a nutrition support team (NST) mitigated extrauterine growth restriction (EUGR) in VLBW infants.
Methods: We retrospectively reviewed the medical records of VLBW infants admitted to Haeundae Paik Hospital between March 2010 and February 2024. EUGR was defined as a decrease in the weight-for-age-z-score>1.2 from birth to the postconceptional age of 36 weeks, using Fenton growth charts.
Results: Among the 603 enrolled VLBW infants, 434 (72.0%) were diagnosed with EUGR. When comparing the control and nutritional intervention groups, the incidence of EUGR was significantly lower in infants in the intervention group (80.6% vs. 62.8%, P<0.00). Intervention group infants started enteral feeding earlier and reached half and full enteral feeding earlier (P<0.05). In addition, intravenous protein and lipid supply started sooner, increased at a faster rate, and reached peak concentrations sooner in the intervention group (P<0.05).
Conclusion: Nutritional intervention by an NST resulted in a significant decrease in the development of EUGR in VLBW infants.
- 3,987 View
- 62 Download
- Perioperative nutritional practice of surgeons in Korea: a survey study
-
Ji-Hyeon Park, Mi Ran Jung, Sang Hyun Kim, Hongbeom Kim, Gyeongsil Lee, Jae-Seok Min, Heung-Kwon Oh, Jung Hoon Bae, Yoona Chung, Dong-Seok Han, Seung Wan Ryu, The External Relation Committee of the Korean Society of Surgical Metabolism and Nutrition
- Ann Clin Nutr Metab 2024;16(3):134-148. Published online December 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.3.134
-
Abstract
PDFSupplementary Material
- Purpose: Enhanced recovery after surgery (ERAS) protocols advocate reduced fasting and early nutrition to improve recovery in surgical patients. However, data on ERAS implementation among Korean surgeons performing major abdominal surgeries remain sparse.
Methods: A survey conducted by the External Relation Committee of the Korean Society of Surgical Metabolism and Nutrition assessed perioperative nutritional practices among 389 Korean general surgeons from February to September 2023. The survey covered preoperative fasting, carbohydrate drinks, nasogastric tube use, postoperative dietary progression, parenteral nutrition (PN), and oral supplements, yielding 551 responses stratified by specialty.
Results: More than 80% of respondents practiced “midnight NPO (Nil Per Os)” fasting, often at the anesthesiology department’s request, while 70%–80% reported no use of preoperative carbohydrate drinks. Most surgeons began dietary progression with water on postoperative day one, advancing to a liquid or soft diet by day two. PN was routinely prescribed by 49% of respondents, with a common dosage of 1,000–1,500 kcal/d. Oral supplements were selectively provided, with 21% of surgeons prescribing them universally.
Conclusion: The results reveal significant variability in perioperative nutrition practices across Korean surgical specialties, with many adhering to traditional practices despite ERAS guidelines. These findings highlight a need for standardized guidelines in Korea to optimize perioperative nutritional support and improve patient recovery outcomes following major abdominal surgeries. -
Citations
Citations to this article as recorded by- Development of the Korean enhanced recovery after surgery audit program
Soo-Hyuk Yoon, Jae-Woo Ju, Ho-Jin Lee, Jeesun Kim, Min Jung Kim, Ji Won Park, Do Joong Park, Seung Yong Jeong
Scientific Reports.2025;[Epub] CrossRef - Perioperative nutrition practices in gastrointestinal cancer surgery: A nationwide survey among German surgical departments
Rahel Maria Strobel, Katharina Beyer, Johannes Christian Lauscher, Marc Martignoni, Christoph Reißfelder, Tim Vilz, Arved Weimann, Maria Wobith
Langenbeck's Archives of Surgery.2025;[Epub] CrossRef
- Development of the Korean enhanced recovery after surgery audit program
- 8,443 View
- 100 Download
- 2 Crossref
Interesting image
- Pneumothorax due to malpositioned nasogastric enteral feeding tube
-
Hyebeen Kim, Suk-Kyung Hong
- Ann Clin Nutr Metab 2024;16(2):87-88. Published online August 1, 2024
- DOI: https://doi.org/10.15747/ACNM.2024.16.2.87
-
PDF
-
Citations
Citations to this article as recorded by- Bilateral Pneumothoraces During Nasogastric Tube Placement: A Case Report
Gideon Asaolu, Martin Aaron Tan, Jay Narula, Rajat Gupta, Sana Ahmed, Hardeep Singh, Dhaval Patel, Amr A. Arafat
Case Reports in Medicine.2026;[Epub] CrossRef
- Bilateral Pneumothoraces During Nasogastric Tube Placement: A Case Report
- 3,271 View
- 36 Download
- 1 Crossref
Original Article
- Consultation pattern changes of parenteral nutrition with a multidisciplinary nutrition support team in a recently opened hospital in Korea: a retrospective cohort study
-
Kyoung Won Yoon, Hyo Jin Kim, Yujeong Im, Seul Gi Nam, Joo Yeon Lee, Hyo Gee Lee, Joong-Min Park
- Ann Clin Nutr Metab 2023;15(2):57-63. Published online August 1, 2023
- DOI: https://doi.org/10.15747/ACNM.2023.15.2.57
-
Abstract
PDF
- Purpose: Parenteral nutrition (PN) is essential for the treatment of patients with malnutrition. The provision of central PN should be recommended by a nutrition support team (NST) made up of a team of experts, even in a newly established hospital. This study sought to evaluate the effectiveness of PN delivered by a multidisciplinary NST in a recently opened hospital.
Methods: This was a retrospective study of the effectiveness of a central PN recommendation pop-up message by the electronic medical record (EMR) software to prompt physicians to either calculate the required calorie and protein intake or consult with the NST. The study period was divided into pre-NST and post-NST based on the time of recruitment of NST-dedicated personnel.
Results: Patients in the 12-week pre-NST period (n=50) and 12-week post-NST period (n=74) were compared retrospectively. Baseline characteristics were not significantly different between the two groups, except for the median Acute Physiology and Chronic Health Evaluation II score (pre-NST group, 8 [interquartile range, IQR 5–15.5] vs. post-NST group, 15 [IQR 9–24], P=0.012) of the 45 patients total admitted to the intensive care unit. The percentage of patients for whom physicians requested a consultation with the NST for central PN was significantly higher in the post-NST group (52.0% vs. 75.7%, P=0.011). There was no significant difference in achievement of nutrition targets or mortality.
Conclusion: Building a multidisciplinary NST may increase awareness of nutritional status and affect the behavior of physicians in recently-opened hospitals.
- 2,978 View
- 17 Download
Review
- Perioperative nutrition support: a narrative review
-
Rajeev Joshi
 , Asma Khalife
, Asma Khalife - Ann Clin Nutr Metab 2023;15(2):40-45. Published online August 1, 2023
- DOI: https://doi.org/10.15747/ACNM.2023.15.2.40
-
Abstract
PDF
- Purpose: Proper nutrition and supplementation are paramount in surgical patients. Suboptimal nutrition status is increasingly recognized as an independent predictor of poor surgical outcomes. The purpose of this review is to highlight the need for nutritional protocols, with an emphasis on perioperative nutrition.
Current concept: Perioperative nutrition support is considered an adjunctive strategy in most centers, although it is proven to be the key in improving surgical outcomes. There is a need to increase the standards and formulate policies and protocols to optimize perioperative nutrition support. Components of perioperative nutrition include nutritional screening and assessment, prehabilitation, preoperative metabolic optimization and carbohydrate loading, postoperative early enteral feeding and perioperative parenteral nutrition, immunonutrition and micronutrients, and oral nutritional supplementation vs. hospital-based kitchen feeds. Supplemental parenteral nutrition becomes valuable when enteral nutrition alone cannot fulfil energy needs. In patients in the surgical intensive care unit who are dealing with hemodynamic instability, high levels of serum lactate unrelated to thiamine deficiency, acidosis, significant liver dysfunction, high blood sugar, and high blood lipid levels, parenteral nutrition must be started with caution. In the post-surgery care ward, it is advisable to administer up to 30 kcal/kg/day and 1.2–2 g/kg/day of protein.
Conclusion: The positive impact of comprehensive nutritional support and the importance of setting and executing standards must be highlighted. Emphasis should be placed on overcoming existing challenges in implementing nutrition therapy in current surgical practice, as better perioperative nutrition supports better surgical outcomes. -
Citations
Citations to this article as recorded by- Preoperative Optimization in Patients with Diabetes Undergoing Foot and Ankle Surgery: BMI, Glycemic Control, and GLP-1 Agonists
Kaitlyn Leslie Hurka, Arun Kiran Movva, Anoop Sunkara, Siddhartha Kalala, Michael O’Connor Sohn, Kishen Mitra, Albert Thomas Anastasio
Diabetology.2026; 7(3): 54. CrossRef - Fueling failure or fostering fusion? A critical review of the potential effect of ketogenic, intermittent fasting, and low-carbohydrate diets on dental implant osseointegration
Faris A. Alshahrani, Noha Taymour
The Saudi Dental Journal.2026;[Epub] CrossRef - Peri-operative nutrition in femoral neck fracture arthroplasty: a pragmatic framework to mitigate dual-hit catabolism and improve outcomes
Leonard Muhango, Dyllan B. Geldenhuys, Nena Elebo, Winifred Mukiibi, Nkhodiseni Sikhauli, Jurek R.T. Pietrzak
Orthopedic Reviews.2026;[Epub] CrossRef - Nutritional intervention for weight loss in presurgical phase – case study
Ana-Maria Damian
The Romanian Journal of Nutrition.2024; 4(4): 4. CrossRef
- Preoperative Optimization in Patients with Diabetes Undergoing Foot and Ankle Surgery: BMI, Glycemic Control, and GLP-1 Agonists
- 31,381 View
- 341 Download
- 4 Crossref
Original Article
- Comparison of a volume-based feeding protocol with standard feeding for trauma patients in intensive care units in Korea: a retrospective cohort study
-
Juhong Park, Yesung Oh, Songhee Kwon, Ji-hyun Lee, Mihyang Kim, Kyungjin Hwang, Donghwan Choi, Junsik Kwon
- Ann Clin Nutr Metab 2023;15(1):22-29. Published online April 1, 2023
- DOI: https://doi.org/10.15747/ACNM.2023.15.1.22
-
Abstract
PDF
- Purpose: Although early enteral nutrition for critically ill patients is essential, it is difficult to provide enteral nutrition to trauma patients in early hospitalization stages due to frequent surgeries and examinations. We aimed to identify the effect of achieving early enteral nutrition goals and improving outcomes through a volume-based feeding (VBF) protocol for trauma patients.
Methods: Patients who were admitted to the trauma intensive care units (TICUs) of the Ajou University Hospital from January 2020 to September 2021 and received enteral tube feeding for at least 7 days were studied. An institution-specific VBF protocol was developed, and nurses were trained in its execution. We retrospectively compared outcomes, such as in-hospital mortality and initial nutritional goal achievement, between the new and standard protocols.
Results: Among 2,935 patients, 109 met the inclusion criteria. Of these, 64 patients received nutrition through VBF, with no feeding intolerance symptoms. The VBF group started enteral nutrition approximately 16.9 hours earlier and group achieved 80% of the target calorie and protein intake approximately one day faster than the control group (n=45). The average calorie supply per body weight per day was 4.9 kcal/kg/day more in the VBF group. An increase of 0.2 g/kg/day was also observed in protein uptake. However, mortality and adverse hospital events did not differ between the groups.
Conclusion: The VBF protocol for patients admitted to the TICU increased the initial nutrient supply without risk of feeding intolerance, but there was no improvement in major clinical outcomes, including mortality and adverse hospital events. -
Citations
Citations to this article as recorded by- Early initiation of gastric tube feeding: ultrasound assessment. A prospective interventional study
Islam M. Elbardan, Ahmed A. Alla Ossman, Nada El Kayal, Assem A. ElRazek Abd-Rabih
Research and Opinion in Anesthesia & Intensive Care.2024; 11(4): 270. CrossRef
- Early initiation of gastric tube feeding: ultrasound assessment. A prospective interventional study
- 6,301 View
- 83 Download
- 1 Crossref
Review
- Efficacy of monounsaturated fatty acids in reducing risk of the cardiovascular diseases, cancer, inflammation, and insulin resistance: a narrative review
-
Ki Hyun Kim, Yoonhong Kim, Kyung Won Seo
- Ann Clin Nutr Metab 2023;15(1):2-7. Published online April 1, 2023
- DOI: https://doi.org/10.15747/ACNM.2023.15.1.2
-
Abstract
PDF
- Purpose: The purpose of this review is to explore the potential benefits of monounsaturated fatty acids (MUFAs), specifically those found in olive oil, on weight loss, cardiovascular disease, cancer, inflammation, and insulin resistance. Additionally, this review examines the use of olive oil–based intravenous lipid emulsions (ILEs) in providing parenteral nutrition to patients with diverse needs.
Current concept: MUFAs, found in olive oil, nuts, and some animal foods, have been found to have numerous health benefits. A diet high in MUFAs can aid in weight loss and reduce the risk of cardiovascular disease. Olive oil, in particular, has been linked to a lower risk of cancer, inflammation, and insulin resistance. In addition, olive oil–based ILEs have been utilized for over two decades and are well tolerated by patients requiring parenteral nutrition.
Conclusion: A diet rich in MUFAs, specifically from olive oil, can provide numerous health benefits, including weight loss and reducing the risk of cardiovascular disease, cancer, inflammation, and insulin resistance. Additionally, olive oil–based ILEs have been shown to effectively provide nutrients to diverse populations requiring parenteral nutrition and have demonstrated the ability to preserve immune function and induce less lipid peroxidation than other ILEs. Further research is needed to fully understand the potential benefits of MUFAs and olive oil-based ILEs, but current evidence suggests that they may be a valuable addition to a healthy diet and medical treatment. -
Citations
Citations to this article as recorded by- Effects of daily extra virgin olive oil consumption on biomarkers of inflammation and oxidative stress: a systematic review and meta-analysis
Jéssica Vidal Damasceno, Anderson Garcez, Andressa Anelo Alves, Isabella Rosa da Mata, Simone Morelo Dal Bosco, Juliano Garavaglia
Critical Reviews in Food Science and Nutrition.2026; 66(2): 392. CrossRef - Applying Wild Mistol Fruits (Sarcomphalus Mistol) from the Paraguayan Chaco as Value-Added Food Ingredients
Villalba R., Belotto J., Coronel E., Carvajal M., Recalde C., Caballero S., Friesen A., Mereles L.
Plant Foods for Human Nutrition.2026;[Epub] CrossRef - Multi-Omics Integration Reveals Key Genes, Metabolites and Pathways Underlying Meat Quality and Intramuscular Fat Deposition Differences Between Tibetan Pigs and Duroc × Tibetan Crossbred Pigs
Junda Wu, Qiuyan Huang, Baohong Li, Zixiao Qu, Xinming Li, Fei Li, Haiyun Xin, Jie Wu, Chuanhuo Hu, Sen Lin, Xiangxing Zhu, Dongsheng Tang, Chuang Meng, Zongliang Du, Erwei Zuo, Fanming Meng, Sutian Wang
Animals.2026; 16(2): 214. CrossRef - The MetaboHealth Score Enhances Insulin Resistance Metabotyping for Targeted Fat Loss: The PERSON Study
Jordi Morwani‐Mangnani, Fatih A. Bogaards, Alexander Umanets, Gabby B. Hul, Anouk Gijbels, Gijs H. Goossens, Joris Deelen, Marian Beekman, Lydia Afman, Ellen E. Blaak, P. Eline Slagboom
Obesity.2026; 34(3): 550. CrossRef - Video and Text‐Based Supplemental Health Information and Consumer Willingness to Pay for Nutrient‐Enhanced Eggs
Edeoba W. Edobor, Michael J. Best, Anita R. Best, Ondulla T. Toomer
Agribusiness.2026;[Epub] CrossRef - Optimizing Pistacia lentiscus (mastic tree) food and healthcare applications: phytochemical composition, extraction methods, quality control, and novel delivery systems
Mohamed A. Anwar, Yuting Fu, Haroun Khan, Mohamed A. Farag
Phytochemistry Reviews.2026; 25(5): 3249. CrossRef - Soybean molasses: a promising substrate for the production of microbial oil by Phaffia rhodozyma
Shirley Denisse Ccori Ponce, Luiz Henrique Han, Luiz Antonio de Almeida Pinto, Carlos André Veiga Burkert, Janaina Fernandes de Medeiros Burkert
Bioprocess and Biosystems Engineering.2026;[Epub] CrossRef - The impact of Lactiplantibacillus plantarum on the cream composition: Insight into changes of vitamin D3 content and fatty acid composition
Tetiana Dyrda-Terniuk, Viorica Railean, Aleksandra Bogumiła Florkiewicz, Justyna Walczak-Skierska, Mateusz Kolankowski, Joanna Rudnicka, Dorota Białczak, Paweł Pomastowski
International Dairy Journal.2025; 161: 106118. CrossRef - Palmitoleic and oleic fatty acids as biomarkers for coronary heart disease: A predictive model
Guangzhou Wang, Lin Zhou, Zhengfang Wang, Asmaa Ali, Liang Wu
Irish Journal of Medical Science (1971 -).2025; 194(1): 59. CrossRef - Macrophages: their role in immunity and their relationship with fatty acids in health and disease
Mayte Rueda-Munguía, Luis Alberto Luévano-Martínez, Gerardo García-Rivas, Elena Cristina Castillo, Omar Lozano
Frontiers in Immunology.2025;[Epub] CrossRef - Evaluation of the Nutritional Value of Prunus dulcis Blossoms and the Antioxidant Compounds of Their Extracted Oil Using Green Extraction Method
Theodoros Chatzimitakos, Vassilis Athanasiadis, Konstantina Kotsou, Ioannis Makrygiannis, Eleni Bozinou, Stavros I. Lalas
Applied Sciences.2024; 14(5): 2001. CrossRef - Oleic Acid and Succinic Acid: A Potent Nutritional Supplement in Improving Hepatic Glycaemic Control in Type 2 Diabetic Sprague–Dawley Rats
Kemmoy G. Lattibeaudiere, Ruby Lisa Alexander-Lindo, Mozaniel Oliveira
Advances in Pharmacological and Pharmaceutical Sciences.2024;[Epub] CrossRef
- Effects of daily extra virgin olive oil consumption on biomarkers of inflammation and oxidative stress: a systematic review and meta-analysis
- 40,195 View
- 156 Download
- 12 Crossref
Case Report
- Development of Wernicke’s Encephalopathy during Total Parenteral Nutrition Therapy without Additional Multivitamin Supplementation in a Patient with Intestinal Obstruction: A Case Report
-
Cheong Ah Oh
- Ann Clin Nutr Metab 2022;14(2):93-96. Published online December 1, 2022
- DOI: https://doi.org/10.15747/ACNM.2022.14.2.93
-
Abstract
PDF
- Wernicke’s encephalopathy (WE) is a serious neurological disorder that can be fatal if not properly treated. In this current paper, I present the case of a 51-year-old male with a perivesical fistula between a presacral abscess and the rectus abdominis muscle. He received total parenteral nutrition therapy during a fasting period because of small bowel obstruction and later developed WE. The patient’s WE-related symptoms improved following rapid treatment with high doses of thiamine.
- 5,238 View
- 38 Download
Original Article
- Provision of Enteral Nutrition in the Surgical Intensive Care Unit: A Multicenter Prospective Observational Study
-
Chan-Hee Park, Hak-Jae Lee, Suk-Kyung Hong, Yang-Hee Jun, Jeong-Woo Lee, Nak-Jun Choi, Kyu-Hyouck Kyoung
- Ann Clin Nutr Metab 2022;14(2):66-71. Published online December 1, 2022
- DOI: https://doi.org/10.15747/ACNM.2022.14.2.66
-
Abstract
PDF
- Purpose: Timely enteral nutrition (EN) is important in critically ill patients. However, use of EN with critically ill surgical patients has many limitations. This study aimed to analyze the current status of EN in surgical intensive care units (ICUs) in South Korea.
Materials and Methods: A multicenter, prospective, observational study was conducted on patients who received EN in surgical ICUs at four university hospitals between August 2021 and January 2022.
Results: This study included 125 patients. The mean time to start EN after admission to the surgical ICU was 6.2±4.6 days. EN was provided to 34 (27.2%) patients within 3 days after ICU admission. At 15.7±15.9 days, the target caloric requirement was achieved by 74 (59.2%) patients through EN alone. Furthermore, 104 (83.2%) patients received supplemental parenteral nutrition after a mean of 3.5±2.1 days. Only one of the four hospitals regularly used enteral feeding tubes and post-pyloric feeding tubes.
Conclusion: Establishing EN guidelines for critically ill surgical patients and setting an appropriate insurance fee for EN-related devices, such as the feeding pump and enteral feeding tube, are necessary.
- 4,937 View
- 37 Download
Review Article
- Selection of the Enterostomy Feeding Route in Enteral Nutrition
-
Dong-Seok Han
- Ann Clin Nutr Metab 2022;14(2):50-54. Published online December 1, 2022
- DOI: https://doi.org/10.15747/ACNM.2022.14.2.50
-
Abstract
PDF
- Enteral nutrition has several physiologic advantages. For example, it can reduce complications, result in immunological improvement, and prevent bacterial translocation by maintaining the integrity of the intestinal barrier. Enteral tube feeding has a major role in nutritional support of patients with swallowing disorders caused by stroke or other neurologic disorders, neoplasms of the upper digestive tract, and benign esophageal stricture. This review article aimed to present the current knowledge on the clinical application of enteral tube feeding. Especially, based on a literature search on PubMed using the index terms of enteral tube feeding; the indications, advantages, and disadvantages; and insertion methods of various enteral tubes were identified.
-
Citations
Citations to this article as recorded by- Preprocedural prognostic nutritional index predicts early gastrointestinal symptoms after percutaneous endoscopic gastrostomy or percutaneous radiologic gastrostomy in Korea: a retrospective cohort study
Yoonhong Kim, Jee Young Lee, Yeajin Moon, Seung Hun Lee, Kyung Won Seo, Ki Hyun Kim
Ann Clin Nutr Metab.2025; 17(3): 196. CrossRef
- Preprocedural prognostic nutritional index predicts early gastrointestinal symptoms after percutaneous endoscopic gastrostomy or percutaneous radiologic gastrostomy in Korea: a retrospective cohort study
- 11,095 View
- 65 Download
- 1 Crossref
Original Articles
- Characteristics and Practice of Parenteral Nutrition in Hospitalized Adult Cancer Patients in Korea
-
Hyo Jung Park, You Min Sohn, Jee Eun Chung, Jung Tae Kim, Jin A Yang, Hye Jung Bae, Ye Won Sung, Sun Hwa Kim,Ji Yoon Cho, Kyung Mi Jung, Hee Kyung Bae
- J Clin Nutr 2020;12(2):34-40. Published online December 31, 2020
- DOI: https://doi.org/10.15747/jcn.2020.12.2.34
-
Abstract
PDF
- Purpose: There have been no clinical studies on the characteristics of parenteral nutrition (PN) for adult cancer inpatients in South Korea. The published evidence describing modern PN practices in these patients is also extremely limited. Therefore in this retrospective multicenter cross-sectional study, we aimed to investigate the PN support practice in hospitalized adult cancer patients.
Methods: The study included adult cancer patients hospitalized in nine hospitals in South Korea and received PN, during the period from August 1st, 2017 to October 30th, 2017. We evaluated the relevant hospital-based PN practices in this group.
Results: Among the 11,580 inpatient admissions during this period, 759 cancer patients received PN (6.6%). The majority of enrolled patients (97.2%) used commercially available PN and 71.2% of these used peripheral PN formulations. The average in-hospital PN duration was 16.1±19.9 days. Patients received only 65.4±25.4% calories of the recommended target calories. The in-hospital mortality of enrolled patients was 26.1%.
Conclusion: We conclude that commercial PN is the most common form of PN administered to hospitalized adult cancer patients and the overall in-hospital mortality in the patients using PN is higher in South Korea compared to other countries.
- 1,491 View
- 8 Download
- Status of Nutritional Support after Emergency Gastrointestinal Surgery in Korea: Retrospective Multicenter Study
-
Dae Sang Lee, Young Eun Park, Kyoung Hoon Lim, Ye Rim Chang, Suk-Kyung Hong, Minchang Kang, Jung-Min Bae, Ji Young Jang, Young Goun Jo, Ki Hoon Kim, Gil Jae Lee
- Surg Metab Nutr 2020;11(1):1-6. Published online June 30, 2020
- DOI: https://doi.org/10.18858/smn.2020.11.1.1
-
Abstract
PDF
- Purpose: Surgery itself causes an inflammatory response to an injury to the patient that leads to a stress metabolic state. Emergency gastrointestinal surgery may cause complications, such as ileus, bowel obstruction, ischemia, or anastomotic leakage, resulting in a delayed oral diet or poor overall nutrition. This study investigated the route of nutrition for patients who underwent emergency gastrointestinal surgery and when to provide nutrition after surgery.
Materials and Methods: Ten hospitals collected data retrospectively on the nutritional status and nutritional status of patients undergoing emergency gastrointestinal surgery for one year from January to December 2016. The clinical outcomes of the nutrient supply method, duration of supply, and type of surgery were performed. The dates from the time of surgery to the start of enteral nutrition, oral nutrition, and parenteral nutrition were calculated.
Results: Of 706 patients, there were 187 (26.5%) trauma patients, of which 63.5% were male. The onset of nutrition began after an average of 10.7 days postoperatively and after an average of 12.1 days of enteral nutrition. On average, it took 7.7 days to provide adequate calories, of which 63.3% had achieved adequate calories within a week. In the case of minimally invasive surgery, such as laparoscopic surgery, the adequate calorie supply time was five days, which was reached within one week.
Conclusion: In a retrospective multicenter analysis, the patients who underwent emergency gastrointestinal surgery had a late start of oral or enteral nutrition, and the ratio of adequate calorie supply within a week was low.
- 1,036 View
- 3 Download
- The Influence of Pediatric Nutrition Support Team on Hospitalized Pediatric Patients Receiving Parenteral Nutrition
-
Sijin Baek, Juhyun Rho, Hyung Wook Namgung, Eunsook Lee, Euni Lee, Hye Ran Yang
- J Clin Nutr 2020;12(1):7-13. Published online June 30, 2020
- DOI: https://doi.org/10.15747/jcn.2020.12.1.7
-
Abstract
PDF
- Purpose: Malnutrition is a common problem in hospitalized patients that can increase the risk of complications, including infections and length of hospitalization. Appropriate nutritional support is important, particularly in pediatric patients, because growth and development are closely related to the nutritional supply. This study examined the status of nutritional support for pediatric patients in general wards to determine if interventions of the pediatric nutrition support team (pNST) contribute to appropriate nutritional support and help improve their nutritional status.
Methods: Between July 2016 and June 2017, all pediatric inpatients who received parenteral nutrition support at the Seoul National University Bundang Hospital were recruited and divided into the NST group and non-NST group according to the activities of pNST. The nutritional status was assessed in all subjects, and the calories and proteins delivered through nutritional support in each group were calculated and then compared with the recommended requirements in pediatric patients.
Results: The number of patients recruited was 174: 100 (57.5%) in the NST group and 74 (42.5%) in the non-NST group. Significantly more calories and protein were supplied in the NST group than the non-NST group in hospitalized children aged between four and 17 years (P<0.05). In the non-NST group, the amounts of calories supplied were insufficient compared to the recommended requirements. The proportion of patients supplied with the appropriate number of calories was 60.0% in the NST group and 20.0% in the non-NST group (P<0.001), and the proportion of cases supplied with the appropriate amount of protein was 87.0% in the NST group and 62.2% in the non-NST group (P<0.001).
Conclusion: Interventions of the pediatric nutrition support team contributed to the sufficient supply of calories and protein and the improvement of clinical outcomes in hospitalized children on parenteral nutrition therapy. -
Citations
Citations to this article as recorded by- Perioperative nutritional practices and pediatric nutrition support team implementation in Korea: a cross-sectional study
Dayoung Ko, Honam Hwang, Hee-Beom Yang, Joong Kee Youn, Hyun-Young Kim
Ann Clin Nutr Metab.2025; 17(3): 181. CrossRef
- Perioperative nutritional practices and pediatric nutrition support team implementation in Korea: a cross-sectional study
- 1,489 View
- 8 Download
- 1 Crossref
- Analysis of Compliance and Clinical Outcomes by Expanding Physician’s Departments in Pediatric Nutrition Support Team
- Hae Won Lee, Min Jae Jung, Ji Eun Park, Hee Kwon, Jae Song Kim, Hong Go, Eun Sun Son
- J Clin Nutr 2019;11(2):42-51. Published online December 31, 2019
- DOI: https://doi.org/10.15747/jcn.2019.11.2.42
-
Abstract
PDF
Purpose:
Malnutrition in hospitalized children has an impact on growth, morbidity, and mortality. For this reason, the implementation of pediatric nutrition support team (PNST) has been suggested. On April 2017, in Severance Hospital, more PNST physician’s departments participated in PNST, and a PNST physician assigning system was changed to be the same departments with the attending physician and PNST physician. This study performed a comparative analysis of the compliance and clinical outcomes after expanding the participation of the PNST physician’s department.
Methods:
Pediatric patients, who were referred to a PNST consultant, were divided into two groups: an unmatched group (different departments with the attending physician and PNST physician [154 patients, 233 consultations from May 2016 to October 2016]), and a matched group (same departments with the attending physician and PNST physician [169 patients, 302 consultations from May 2017 to October 2017]). The PNST compliance and clinical outcomes, such as the total delivered/required caloric and protein ratio, % ideal body weight (%IBW), serum total protein, and serum albumin, in the two groups were compared.
Results:
The compliance was significantly higher in the matched group than the unmatched group (63.4% vs. 47.3%, P=0.005). Although there was no significant difference, the total delivered/required caloric and protein ratio, and %IBW in the matched group tended to increase. The serum total protein (0.7±0.7 g/dL vs. –0.4±1.3 g/dL, P=0.004) and serum albumin (0.5±0.5 g/dL vs. –0.1±0.6 g/dL, P=0.003) were significantly higher in the matched group.
Conclusion:
After expanding the physician’s departments in PNST, the compliance was significantly higher in the matched group and the clinical outcomes tended to better. The physician assigning system to be matched with the departments between the attending physician and the PNST physician may help increase the compliance of NST consultations, resulting in an improvement of the patient’s clinical outcomes.
- 1,241 View
- 1 Download
Review Articles
- Nutritional Support for Cancer Patients
- Yoontaek Lee
- Surg Metab Nutr 2019;10(2):27-31. Published online December 30, 2019
- DOI: https://doi.org/10.18858/smn.2019.10.2.27
-
Abstract
PDF
Cancers are the leading cause of death worldwide, and various modalities of cancer treatment, such as surgery, radiation therapy, and pharmacological therapies, have been applied. Malnutrition and a loss of muscle mass are encountered frequently in cancer patients and adversely affect the clinical outcomes. Therefore, screening for, monitoring, and treating malnutrition are important procedures in treating cancer patients. This paper reviews the guidelines as well as comparative studies describing the nutritional support provided to cancer patients and describes the evidence-based guidelines and recommendation for each topic.
- 2,255 View
- 21 Download
- Nutrition Support for Pediatric Surgical Patients
- Jun Beom Park
- Surg Metab Nutr 2019;10(1):9-14. Published online June 30, 2019
- DOI: https://doi.org/10.18858/smn.2019.10.1.9
-
Abstract
PDF
Pediatric patients have characteristics such as a low capacity for storing energy/nutrients and high energy metabolism as compared those of adults. Because of the inherent characteristics that they are continually growing, supplying both rapid and adequate nutrition is of the utmost importance. In the case of children undergoing surgery (and particularly gastrointestinal surgery), there is a high possibility of a restricted supply of nutrition, and so active intervention to supply sufficient nutrition must be carried out. Of course, enteral nutrition is preferred, but continuous monitoring of nutrition is of paramount importance; thus, parenteral nutrition should be provided when necessary. Nutritional support requires continuous monitoring when and if complications arise. The complications of parenteral nutrition have yet to be overcome, so further research on this topic is certainly warranted.
- 1,409 View
- 9 Download
Original Article
- Physiological Change of Serum Bilirubin Level by ω-3 Enriched Parenteral Nutrition Versus ω-3 Free Parenteral Nutrition in Healthy Male Subjects
- Mi Rin Lee, Min-Gul Kim, Jae Do Yang, Hong Pil Hwang, Yunjeong Kim, Ji-Young Jeon, Sungwoo Ahn, Hee Chul Yu
- Surg Metab Nutr 2019;10(1):20-26. Published online June 30, 2019
- DOI: https://doi.org/10.18858/smn.2019.10.1.20
-
Abstract
PDF
Purpose:
Bilirubin is a biomarker for the diagnosis of liver diseases or bile duct dysfunction. This study assessed the physiological changes in the blood bilirubin level infusing ω-3 enriched parenteral nutrition (PN) and ω-3 free PN in healthy male subjects.
Materials and Methods:
This study was a randomized, open-label, two-treatment, two-way crossover trial. Sixteen subjects were assigned randomly to one of two sequences of the two treatments: ω-3 enriched PN or ω-3 free PN was infused via aperipheral venous catheter for six hours at 3 mL/kg/h. Blood samples were collected every one hour from 0 to 12 hours after starting an intravenous infusion for bilirubin concentrations. The total bilirubin and direct bilirubin concentrations in the blood were analyzed using an enzymatic method.
Results:
The bilirubin concentration in the blood was reduced while infusing the ω-3 enriched PN and ω-3 free PN. When it stopped infusing, the bilirubin concentration was recovered. A similar pattern was observed, but there was a further decline and recovery in ω-3 free PN.
Conclusion:
When ω-3 enriched PN and ω-3 free PN are infused in healthy male subjects, the blood bilirubin level decreasedand there is no difference between the two groups.
- 4,591 View
- 8 Download
Review Article
- Review of Worldwide Regulations and Management Systems for Medical Foods
- Hyojung Lim, Jeong-Meen Seo
- J Clin Nutr 2019;11(1):5-11. Published online June 30, 2019
- DOI: https://doi.org/10.15747/jcn.2019.11.1.5
-
Abstract
PDF
Enteral nutrition (EN) formulas are foods that are used to improve the nutritional status of patients and these foods’ safety and quality must be ensured. Therefore, EN formulas in other countries are managed differently from that of general foods. We investigated the direction of development of the relevant laws regulations and guidelines pertaining to EN formulas and we compared these laws regulations and guidelines from different countries, including Korea. The United States and Europe manage EN formulas as foods, but they are managed differently compared to general foods because of separate laws or programs pertaining to EN foods. In addition, the use of the formulas does not necessarily require a prescription, but when used by prescription, then medical insurance covers them. In Japan, there are two types of EN formulas, food and drug, and there are differences for their management and insurance coverage. In the case of Korea, EN formulas are classified as food and drug, and different management and insurance are applied in each case, which inhibits their systematic management and industrial development. Integration of a management system and establishment of a legal foundation is necessary for the systematic management and development of EN formula in Korea.
-
Citations
Citations to this article as recorded by- Report on the Current Trend of Commercial Enteral/Parenteral Nutrition in Outpatient
Hyun Ji Lee, Hyo Jung Park, Seon Young Chung, Myung Sook Min, Ok Soon Jeong, Ja Kyung Min
Journal of Korean Society of Health-System Pharmacists.2023; 40(2): 211. CrossRef
- Report on the Current Trend of Commercial Enteral/Parenteral Nutrition in Outpatient
- 2,071 View
- 12 Download
- 1 Crossref
Original Article
- Nutritional Therapy Related Complications in Hospitalized Adult Patients: A Korean Multicenter Trial
- Eun-Mi Seol, Kye Sook Kwon, Jeong Goo Kim, Jung-Tae Kim, Jihoon Kim, Sun-Mi Moon, Do Joong Park, Jung Hyun Park, Je Hoon Park, Ji Young Park, Jung-Min Bae, Seung Wan Ryu, Ji-Young Sul, Dong Woo Shin, Cheung Soo Shin, Byung Kyu Ahn, Soo Min Ahn, Hee Chul Yu, Gil Jae Lee, Sanghoon Lee, A Ran Lee, Jae Young Jang, Hyun Jeong Jeon, Sung Min Jung, Sung-Sik Han, Suk-Kyung Hong, Sun-Hwi Hwang, Yunhee Choi, Hyuk-Joon Lee
- J Clin Nutr 2019;11(1):12-22. Published online June 30, 2019
- DOI: https://doi.org/10.15747/jcn.2019.11.1.12
-
Abstract
PDF
Purpose:
Nutritional therapy (NT), such as enteral nutrition (EN) or parenteral nutrition (PN), is essential for the malnourished patients. Although the complications related to NT has been well described, multicenter data on symptoms in the patients with receiving NT during hospitalization are still lacking.
Methods:
Nutrition support team (NST) consultations, on which NT-related complications were described, were collected retrospectively for one year. The inclusion criteria were patients who were (1) older than 18 years, (2) hospitalized, and (3) receiving EN or PN at the time of NST consultation. The patients’ demographics (age, sex, body mass index [BMI]), type of NT and type of complication were collected. To compare the severity of each complication, the intensive care unit (ICU) admission, hospital stay, and type of discharge were also collected.
Results:
A total of 14,600 NT-related complications were collected from 13,418 cases from 27 hospitals in Korea. The mean age and BMI were 65.4 years and 21.8 kg/m2. The complications according to the type of NT, calorie deficiency (32.4%, n=1,229) and diarrhea (21.6%, n=820) were most common in EN. Similarly, calorie deficiency (56.8%, n=4,030) and GI problem except for diarrhea (8.6%, n=611) were most common in PN. Regarding the clinical outcomes, 18.7% (n=2,158) finally expired, 58.1% (n=7,027) were admitted to ICU, and the mean hospital days after NT-related complication were 31.3 days. Volume overload (odds ratio [OR]=3.48) and renal abnormality (OR=2.50) were closely associated with hospital death; hyperammonemia (OR=3.09) and renal abnormality (OR=2.77) were associated with ICU admission; “micronutrient and vitamin deficiency” (geometric mean [GM]=2.23) and volume overload (GM=1.61) were associated with a longer hospital stay.
Conclusion:
NT may induce or be associated with several complications, and some of them may seriously affect the patient’s outcome. NST personnel in each hospital should be aware of each problem during nutritional support.
-
Citations
Citations to this article as recorded by- Provision of Enteral Nutrition in the Surgical Intensive Care Unit: A Multicenter Prospective Observational Study
Chan-Hee Park, Hak-Jae Lee, Suk-Kyung Hong, Yang-Hee Jun, Jeong-Woo Lee, Nak-Jun Choi, Kyu-Hyouck Kyoung
Annals of Clinical Nutrition and Metabolism.2022; 14(2): 66. CrossRef - Pathophysiology and protective approaches of gut injury in critical illness
Chang Yeon Jung, Jung Min Bae
Yeungnam University Journal of Medicine.2021; 38(1): 27. CrossRef - Nutrition Support Team Reconsultation During Nutrition Therapy in Korea
Eun‐Mi Seol, Yun‐Suhk Suh, Dal Lae Ju, Hye Jung Bae, Eunjung Kim, Hyuk‐Joon Lee
Journal of Parenteral and Enteral Nutrition.2021; 45(2): 357. CrossRef
- Provision of Enteral Nutrition in the Surgical Intensive Care Unit: A Multicenter Prospective Observational Study
- 2,121 View
- 10 Download
- 3 Crossref
Review Article
- In-line Filtration in Parenteral Nutrition
- Eunjung Kim, Eun-Mi Seol
- J Clin Nutr 2019;11(1):1-4. Published online June 30, 2019
- DOI: https://doi.org/10.15747/jcn.2019.11.1.1
-
Abstract
PDF
Metabolic abnormalities and catheter-related infections are common complications of parenteral nutrition (PN). Particulate contamination is a catheter-related complication can occur when administering PN: mixing the electrolytes, trace elements, vitamins into the PN, or puncturing a rubber stopper at the PN formulation. In addition, the aggregation of the components of the PN solution by a drug incompatibility reaction could be related to particulate contamination. PN contaminated with precipitates, insoluble particles, and bacteria was reported as the cause of the death of a patient. The Food and Drug Administration recommended that the filters be used during PN administration. In-line filters can retain the bacteria and insoluble particles in PN solutions, and prevent their infusion into the patient. Therefore, in-line filters are recommended to prevent catheter-related complications that can occur during PN infusion. A 0.2
µ filter for lipid-free PN and a 1.2µ filter for lipid-containing PN solutions can be used. On the other hand, when a filter is applied, the infusion rate can decrease and the economic burden will increase for patients requiring long-term PN. In addition, small particles, such as viruses, polymers, and proteins cannot be filtered out completely. In conclusion, in-line filers are recommended to prevent catheter-related complications that can occur during PN administration, but there are no international standardized guidelines. Therefore, standardized guidelines will be needed based on evidence accompanied by clinical trials. In addition, in-line filter applications should be considered in the clinical field depending on the patient’s condition.
- 1,661 View
- 17 Download
Original Articles
- Multidisciplinary Intestinal Rehabilitation for Short Bowel Syndrome in Adults: Results in a Korean Intestinal Rehabilitation Team
- Sojeong Yoon, Sanghoon Lee, Hyo Jung Park, Hyun-Jung Kim, Jihye Yoon, Ja-Kyung Min, Jeong-Meen Seo
- J Clin Nutr 2018;10(2):45-50. Published online December 31, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.2.45
-
Abstract
PDF
Purpose:
Intense multidisciplinary team effort is required for the intestinal rehabilitation of patients afflicted with the short bowel syndrome (SBS). These include enteral and parenteral nutrition (PN) support, monitoring of complications related to treatment, and considering further medical or surgical options for intestinal adaptation.
Methods:
In the Intestinal Rehabilitation Team (IRT) at the Samsung Medical Center, we have experienced 20 cases of adult SBS requiring multidisciplinary intestinal rehabilitation. This study is a retrospective review of the collected medical records.
Results:
Of the 20 subjects treated, 12 patients were male and 8 patients were female. At the time of referral to the IRT, the mean age was 51.5 years, and the mean body weight was 50.1 kg, which was 90% of the usual body weight. The diseases or operative managements preceding massive bowel resection were malignancy in 11 cases, cardiac surgery in 2 cases, trauma in 2 cases and one case, each of tuberculosis, corrosive esophagitis, atrial fibrillation, simultaneous pancreas and kidney transplantation, and perforated appendicitis. Of these, there were 14 survivals and 6 mortalities. The fatalities were attributed to progression of disease, intestinal failure-associated liver disease, and sepsis (unrelated to intestinal failure) (2 cases each). Among the 14 surviving patients, 8 patients have been weaned off PN, whereas 6 are still dependent on PN (mean PN dependence 36%).
Conclusion:
This paper reports the results of multidisciplinary intestinal rehabilitation of adult short bowel patients treated at the Samsung Medical Center. Further studies are required to improve survival and enteral tolerance of these patients.
-
Citations
Citations to this article as recorded by- The Post-Discharge Caregiving Experiences of Mothers of Children with Intestinal Failure
Yunhyung Kim, Yeon Hee Kim, Jae Sim Jeong
Journal of Korean Association for Qualitative Research.2024; 9(1): 1. CrossRef - Intestinal Rehabilitation Program for Adult Patients with Intestinal Failure: A 20-Year Analysis of Outcomes in the Single-Center Experience at a Tertiary Hospital
Kyoung Moo Im, Jae Hee Chung
Digestive Diseases and Sciences.2024; 69(5): 1770. CrossRef - Vitamin D Deficiency is Prevalent in Short Bowel Syndrome Patients on Long-Term Parenteral Nutrition Support
SungHyo An, Sanghoon Lee, Hyun-Jung Kim, Hyo Jung Park, Jeong-Meen Seo
Journal of Clinical Nutrition.2021; 13(1): 12. CrossRef - Multidisciplinary Intestinal Rehabilitation in Children: Results from a Korean Intestinal Rehabilitation Team
Cheolgu Lee, Sanghoon Lee, Hyo Jung Park, Hyun-Jung Kim, Ja-Kyung Min, Jeong-Meen Seo
Advances in Pediatric Surgery.2020; 26(2): 61. CrossRef
- The Post-Discharge Caregiving Experiences of Mothers of Children with Intestinal Failure
- 2,122 View
- 2 Download
- 4 Crossref
- Parenteral Nutrition in Hospitalized Adult Patients in South Korea
- Miyoung Ock, Sera Lee, Hyunah Kim
- J Clin Nutr 2018;10(2):38-44. Published online December 31, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.2.38
-
Abstract
PDF
Purpose:
Parenteral nutrition (PN) is known to provide therapeutic beneficial improvements in malnourished patients for whom enteral nutrition is not feasible. The objective of this study was to investigate the current clinical characteristics and utilization of PN in Korea.
Methods:
We analyzed the Health Insurance Review Agency National Inpatients Sample database from 2014 to 2016, which included 13% of all hospitalized patients in Korea. Adult patients aged 20 years or older and receiving premixed multi-chamber bag containing PN were included for this study. Patient characteristics, admission type, primary diagnosis, and hospital demographics were evaluated. SAS version 9.4 was used for data analysis.
Results:
From 2014 to 2016, 149,504 patients received premixed PN, with 226,281 PN prescriptions being written. The mean patient age was 65.0 years, and 81,876 patients (54.8%) were male. Premixed 3-chamber bag and 2-chamber bag PN solutions were utilized in 131,808 (88.2%) and 32,033 (21.4%) patients, respectively. The number of patients hospitalized through the emergency department were 70,693 (47.3%), whereas 43,125 patients (28.8%) were administered PN in intensive care units. In the adult PN patients, the highest primary diagnosis was malignant neoplasm of the stomach (8,911, 6.0%), followed by organism unspecified pneumonia (7,008, 4.7%), and gastroenteritis and colitis of unspecified origin (6,381, 4.3%). Overall, 34% of adult PN patients were diagnosed with malignancies, the most common being neoplasm of the stomach (17.7%), neoplasm of bronchus/lung (11.2%), neoplasm of colon (11.1%), and neoplasm of liver/intrahepatic bile ducts (10.0%). PN solutions were most frequently administered in the metropolitan area (55.0%) and in hospitals with more than 1,000 beds (23.6%).
Conclusion:
PN was commonly administered in older patients, with primary diagnosis of malignancy in a significant number of cases. This study is the first large-scale description of PN-prescribing patterns in real-world clinical practice in South Korea.
- 1,549 View
- 9 Download
- Effect of Total Parenteral Nutrition Therapy in Palliative Gastrojejunostomy Status Patients
- Yung Kil Kim, Geum Jong Song, Tae Sung Ahn, Myoung Won Son, Sun Wook Han, Joon-Hwan Song, Ho Kim, Sang Ho Bae, Sung Yong Kim, Moo Jun Baek, Moon Soo Lee
- Surg Metab Nutr 2018;9(1):26-30. Published online June 30, 2018
- DOI: https://doi.org/10.18858/smn.2018.9.1.26
-
Abstract
PDF
Purpose:
Gastric outlet obstruction (GOO) is a common problem associated with advanced malignancies of the upper gastrointestinal tract. Adverse events, such as malnutrition, can affect the quality of life, and gastrojejunostomy can be performed for palliative care. This study evaluated effects of total parenteral nutrition (TPN) therapy in post-operation state patients who underwent a palliative gastrojejunostomy (PGJ).
Materials and Methods:
Between January 2011 and June 2015, a total of 65 patients underwent PGJ at Soonchunhyang University Cheonan Hospital and all consecutive patients were included in this retrospective study. All patients were divided into the preoperative TPN group and non-TPN group. A nutritional status assessment included the body weight (BW), body mass index (BMI), CRP level, serum albumin, serum total protein, hemoglobin, and total lymphocyte count (TLC).
Results:
Thirty-one patients did not receive the TPN treatment, and 34 patients received the TPN treatment before surgery. Significant differences between preoperative and postoperative BW, BMI, CRP level, serum albumin, serum total protein, hemoglobin, and TLC were observed in the non-TPN group. On the other hand, there was no significant difference between the preoperative BW, BMI, TLC and postoperative BW, BMI, TLC in the TPN group (p=0.914, p=0.873, p=0.319).
Conclusion:
These results suggest that preoperative TPN therapy can improve the nutritional status in patients who underwent PGJ.
- 1,159 View
- 1 Download
Review Article
- Role of Postoperative Parenteral Nutrition in Elective Surgery; Selection of Patients and Conditions for Postoperative Parenteral Nutrition
- Jong Won Kim
- Surg Metab Nutr 2018;9(1):1-4. Published online June 30, 2018
- DOI: https://doi.org/10.18858/smn.2018.9.1.1
-
Abstract
PDF
Postoperative early enteral nutrition or early oral ingestion is recommended in surgical patients. In this situation, this study examined the role of parenteral nutrition in the postoperative period in patients undergoing elective surgery. The nutritional status should be assessed before surgery and in the case of malnutrition, nutritional support should be provided before surgery to obtain good results. More than 2 weeks of insufficient nutritional support after surgery may worsen the patient’s progress. Therefore, it is recommended to start nutritional care if the oral intake is not appropriate until 7 days or 5 to 7 days after surgery. Enteral nutrition is related to the quick restoration of the bowel function and reduction of infection-related complications. Therefore, enteral nutrition has priority. On the other hand, depending on the patient’s condition, it may not be possible to perform enteral nutrition, and the uniform implementation of the early enteral nutrition may be a burden to the patient. Parenteral nutrition has the advantage that it can supply nutrition without being affected by the intestinal condition, and it can be calculated to supply as much energy as required. The situation, where parenteral nutrition is required after elective surgery, could be summarized as 1) the patients who underwent nutritional therapy before surgery and could not tolerate oral intake or enteral nutrition after surgery. or 2) in the case where enteral nutrition did not satisfy 50% of the demand at 7 days after surgery, and it is judged that this situation should continue for 7 days.
- 1,131 View
- 3 Download
Original Article
- Effects of Parenteral Nutrition in Pediatric Patients with Hematopoietic Stem Cell Transplantation
- Soo Young Lim, Min Jae Jung, Ji Eun Park, Jae Song Kim, Soo Hyun Kim, Chuhl Joo Lyu, Eun Sun Son
- J Clin Nutr 2018;10(1):9-19. Published online June 30, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.1.9
-
Abstract
PDF
Purpose:
This study examined the effects of parenteral nutrition (PN) on the nutritional status, clinical improvement, and PN-related complications in pediatric patients who had undergone hematopoietic stem cell transplantation (HSCT).
Methods:
A retrospective audit of 110 pediatric patients (age≤18), who underwent HSCT from March 2015 to February 2017 was undertaken. The patients were divided into 3 groups based on the ratio of daily calorie supplementation to the daily calorie requirement (ROCS). The clinical factors related to the nutritional status, such as difference in body weight (BW), body mass index (BMI), percent ideal body weight (PIBW), total protein (T.protein), and albumin; the early clinical outcome, such as PN-duration, length of hospitaliaztion (LOH), engraftment day (ED), graft-versus-host disease, sepsis, pneumonia and mucositis; and PN-related complications, including elevation of total bilirubin (T.bil), direct bilirubin (D.bil), aspartate aminotransferase, alanine aminotransferase, glucose and cholesterol levels, and hepatic veno-occlusive disease were analyzed using the electronic medical records. Additional analysis subject to auto-HSCT and allo-HSCT patients was also performed.
Results:
The very-low-ROCS, low-ROCS, and satisfied-ROCS group were 30 (27.3%), 47 (42.7%), and 33 (30.0%) patients, respectively. The PN-duration (P=0.005, z=–2.271), LOH (P=0.023, z=–2.840), ED (P<0.001, z=–3.695), T.bil elevation (P<0.001, z=–3.660), and D.bil elevation (P=0.002, z=–3.064) tended to decrease with increasing ROCS. The difference in the PN-duration (P=0.017), ED (P=0.001), T.bil elevation (P=0.001), and D.bil elevation (P=0.011) in the 3 groups was statistically significant. In the auto-HSCT patients, the change in BW (P=0.031, z=+2.154), PIBW (P=0.029, z=+2.187), and BMI (P=0.021, z=+2.306) tended to increase. In the allo-HSCT patients, the change in T.protein (P=0.022, z=+2.286) increased but the ED (P=0.021, z=–2.304) decreased.
Conclusion:
Aggressive PN supplementation has an effect on maintaining the nutritional status and achieving better early outcomes in pediatric HSCT patients, whereas it has no effect on increasing the PN-related complications.
- 1,154 View
- 8 Download
Case Report
- Esophageal Obstruction Caused by the Solidification of Residue of an Enteral Feeding Formula
- Hancheol Jo, Ye Rim Chang, So Mi Kim, Dong Wook Kim, Ye Seob Jee
- J Clin Nutr 2018;10(1):25-30. Published online June 30, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.1.25
-
Abstract
PDF
The nutritional support of acutely ill patients is very important and early enteral nutrition is recommended. Feeding
via the nasogastric route is used widely for its ease of access if the patient cannot maintain volitional food intake. If the position of the tip or side holes of the nasogastric tube (NGT) is above the gastroesophageal junction, there is the possibility of retention and solidification of the administered enteral feeding formula in the esophagus. Therefore, the tip of the NGT should be checked carefully; a chest radiograph to confirm its position can be considered, especially in patients with a higher risk of aspiration and gastroesophageal reflux. In addition, careful consideration of the risk factors that can trigger esophageal obstruction is required when feeding patients in the intensive care unit. This paper describes two unusual cases of esophageal obstruction caused by the solidification of residue of an enteral feeding formula.-
Citations
Citations to this article as recorded by- Body Composition and Physical Performance Measures of a Special Operations Police Unit: Characteristics and Associations Between Determinant Factors of Physical Performance
Braian Fink, Tomás T. Freitas, Santiago Zabaloy
Journal of Science in Sport and Exercise.2024; 6(1): 61. CrossRef
- Body Composition and Physical Performance Measures of a Special Operations Police Unit: Characteristics and Associations Between Determinant Factors of Physical Performance
- 2,749 View
- 2 Download
- 1 Crossref
Original Article
- Clinical Outcomes of Nutritional Supply in Critically Ill Patients in the Prone Position
- Yeonju Lee, Hyung-Sook Kim, Hyungwook Namgung, Eun Sook Lee, Euni Lee, Young-Jae Cho, Yeon Joo Lee
- J Clin Nutr 2018;10(1):2-8. Published online June 30, 2018
- DOI: https://doi.org/10.15747/jcn.2018.10.1.2
-
Abstract
PDF
Purpose:
Enteral nutrition is recommended in critically ill patients. On the other hand, the recommendation of nutritional support is limited and often controversial in critically ill patients in the prone position. Therefore, this study evaluated the clinical outcomes of nutritional support in critically ill patients in the prone position.
Methods:
A retrospective evaluation of the electronic medical records was conducted, including adult patients who were in the medical intensive care unit (ICU) in the prone position in Seoul National University Bundang Hospital from May 1, 2015 to June 30, 2017. The patients’ characteristics, nutritional support status while they were in the prone position, mortality in ICU and during hospitalization, ICU length of stay, mechanical ventilation days, and complications, such as ventilator associated pneumonia (VAP) and vomiting were collected.
Results:
In total, 100 patients were included. Of these, 12 received enteral nutrition and parenteral nutrition and 88 received only parenteral nutrition. The groups were similar in terms of age, sex, number of comorbidity, weight, PaO2/FiO2, hours of prone position, Simplified Acute Physiology Score II (SAPS II), Acute Physiologic and Chronic Health Evaluation II (APACHE II) score, and Sequential Organ Failure Assessment (SOFA) score. No differences were observed in ICU mortality (75.0%
vs . 46.6%; P=0.065), hospital mortality (83.3%vs . 58.0%; P=0.081), ICU length of stay (22.2±14.6vs . 18.2±21.2; P=0.128) and mechanical ventilation days (19.3±14.8vs . 14.5±19.1; P=0.098). In addition, there were no differences in the possible complications of the prone position, such as VAP (8.3%vs . 4.5%; P=0.480) and vomiting (8.3%vs . 1.1%; P=0.227).Conclusion:
No significant differences in the clinical outcomes were observed. Further studies will be needed to confirm the way of nutrition support while in the prone position.
- 1,228 View
- 7 Download
Review Articles
- Enteral Nutrition in Liver Disease
- Kyung Sik Kim
- Surg Metab Nutr 2017;8(2):28-35. Published online December 30, 2017
- DOI: https://doi.org/10.18858/smn.2017.8.2.28
-
Abstract
PDF
Patients with chronic liver disease have a high risk to malnutrition. Proper nutrition should be provided through a proper nutritional assessment. Enteral nutrition is recommended as a nutritional supplement because it maintains the intestinal mucosa, reduces infectious complications, is less costly than parenteral nutrition, and is more physiological to use intestine. The purpose of this review is to define the nutritional deficiencies of patients with liver disease and to show the indications for enteral nutrition and to validate the efficacy of enteral nutrition. According to the various guidelines and researches, enteral nutrition is used as a solution to the nutritional problems caused by patients with liver disease. The optimal enteral formula will be selected on the nutritional problems. It is expected that the enteral nutrition will reduce especially postoperative complications, intraperitoneal complications, pneumonia, and wound infection. The enteral nutrition for patients with chronic liver disease should be actively implemented.
- 1,923 View
- 13 Download
- Parenteral Nutrition-associated Liver Disease
- Jin Hong Lim
- Surg Metab Nutr 2017;8(1):7-12. Published online June 30, 2017
- DOI: https://doi.org/10.18858/smn.2017.8.1.7
-
Abstract
PDF
Parenteral nutrition-associated liver disease (PNALD) is frequently observed in patients who require long-term parenteral nutrition. PNALD is diagnosed by clinical presentation, biochemical liver function test, long-term usage of parenteral nutrition, and negative workup for other liver diseases. Pathogenesis of PNALD is multifactorial and includes prematurity, nutritional excess, sepsis, and lack of enteral nutrition. Since PNALD was first reported more than 30 years ago, there have been various attempts to find effective treatments for PNALD. Cyclic parenteral nutrition and use of ω-3 polyunsaturated long-chain fatty acids (ω-3 PUFA) instead of ω-6 PUFA were reported worldwide as effective treatments. This article reviews the literature relating to PNALD.
-
Citations
Citations to this article as recorded by- The Post-Discharge Caregiving Experiences of Mothers of Children with Intestinal Failure
Yunhyung Kim, Yeon Hee Kim, Jae Sim Jeong
Journal of Korean Association for Qualitative Research.2024; 9(1): 1. CrossRef - Treatment Status of Parenteral Nutrition-Associated Cholestasis in Pediatric Patients at a Single Tertiary Hospital
Soh Yeon Park, Yu Jeong Son, Min Jung Geum, Jong Hee Ko, Eun Sun Son, Yun Mi Yu, Eun Joo Lee
Journal of Korean Society of Health-System Pharmacists.2024; 41(4): 373. CrossRef
- The Post-Discharge Caregiving Experiences of Mothers of Children with Intestinal Failure
- 3,199 View
- 34 Download
- 2 Crossref
Original Articles
- Evaluation on the Time to Start Parenteral Nutrition in Hospitalized Cancer Patients
- Nam Hyo Kim, Hyo Jung Park, Yong Won In, Young Mee Lee
- J Clin Nutr 2017;9(1):30-35. Published online June 30, 2017
- DOI: https://doi.org/10.15747/jcn.2017.9.1.30
-
Abstract
PDF
Purpose:
Malnutrition is quite prevalent in hospitalized cancer patients, with a 40%∼80% rate. Malnutrition in cancer patients can result in an increase in the number of complications, length of stay, mortality, and morbidity. Therefore, cancer patients with malnutrition must have the appropriate nutritional support to improve the prognosis of cancer. This study evaluated the appropriate time point to start parenteral nutrition (PN) after admission according to the nutrition support guidance in Samsung Medical Center.
Methods:
This study enrolled patients diagnosed with the Korean standard classification of disease 6 (KCD6) code C00-C97 and discharged from March 1st to 31st, 2016. The following data were collected: patients’ age, gender, diagnosis, length of stay, body mass index, nutritional status, and whether to consult nutrition support team (NST).
Results:
Among a total of 2,944 patients, 381 patients (12.9%) were in a malnourished status upon admission. In the malnourished patients, 139 patients were prescribed PN for a median of 6 days (range, 1∼49) and moderate to severe malnourished patients were started on PN within 2 days after admission. The proportion of patients with a poor nutritional status was lower in the NST group than in the non-NST group (50.0% vs. 66.7%) on the 28th day after admission. Among the nourished patients, 229 patients were prescribed PN. Of them, 183 patients (79.9%) were started on PN within 7 days after admission.
Conclusion:
In moderate to severe malnourished cancer patients, the initiation of PN on the day after admission is appropriate.
-
Citations
Citations to this article as recorded by- Best evidence summary for the rational use of parenteral nutrition in hospitalized cancer patients
Zhengzheng Liu, Beijia Liu, Niannian Weng, Qian Gui, Di Liu, Yuchi Wu, Guiyu Huang, Mingxue Yang, Xiaoli Tang
Frontiers in Nutrition.2026;[Epub] CrossRef
- Best evidence summary for the rational use of parenteral nutrition in hospitalized cancer patients
- 1,396 View
- 3 Download
- 1 Crossref
- Influence of Fish Oil-Containing Lipid Emulsions on Parenteral Nutrition-Associated Liver Disease in Neonates
- Jeong-A Park, Ji-Eun Park, Min-Jae Jeong, Jae-Song Kim, Eun-Sun Son, Ho-Seon Eun
- J Clin Nutr 2017;9(1):21-29. Published online June 30, 2017
- DOI: https://doi.org/10.15747/jcn.2017.9.1.21
-
Abstract
PDFSupplementary Material
Purpose:
This study is a comparative evaluation of the incidence of parenteral nutrition-associated liver disease (PNALD) when administering intravenous fat emulsions containing fish oil.
Methods:
The medical records of patients who were in the neonatal intensive care unit at Severance Hospital from January, 2012 to December 2015, were reviewed retrospectively. Patients who were administered either soybean oil (SO) or SMOF (containing soybean oil, medium chain triglycerides, olive oil, and fish oil) more than 14 days were included. The patients were excluded if they were administered both agents or had underlying hepatic disease. An increase in bilirubin to 2 mg/dL was defined as PNALD.
Results:
PNALD occurred in only 8 out of a total of 77 patients: 6 out of 31 (19.4%) in the SO group and 2 out of 46 (4.3%) in the SMOF group (P=0.055). The number of patients, whose lab values, such as direct bilirubin, total bilirubin, asparate aminotransferase (AST), alanine amino-transferase, gamma-glutamyl transpeptidase, C-reactive protein, serum triglyceride, and alkaline phosphate, exceeded the normal range, were similar in both groups. The gestational age, birth body weight, and APGAR score at 1 min and 5 min were significantly higher in the SO group and the PN duration was significantly long in the SMOF group. Considering only term infants, there were no significant differences in baseline characteristics and incidence of PNALD. The number of patients whose AST exceeded the normal range was significantly higher in the SO group (P=0.034).
Conclusion:
The incidence of PNALD was similar in both groups. On the other hand, considering the tendency, there was a high correlation between the type of lipid emulsion and an increased direct bilirubin level in the SO group.
- 1,339 View
- 1 Download
- Analysis of Adverse Reactions Associated with Parenteral Nutrition Use in Korea
- Sera Lee, Miyoung Ock, Seonghee Kim, Hyunah Kim
- J Clin Nutr 2017;9(1):16-20. Published online June 30, 2017
- DOI: https://doi.org/10.15747/jcn.2017.9.1.16
-
Abstract
PDF
Purpose:
To evaluate the clinical manifestations of adverse drug reactions (ADRs) of parenteral nutrition (PN) use in Korea.
Methods:
The Korean Adverse Event Reporting System (KAERS) database records in 2015 on PN-treated patients were used. ADRs classified as “certain,” “probable,” and “possible” based on the WHO-Uppsala Monitoring Centre criteria were analyzed.
Results:
In total, 21,436 ADRs from 2,346 patients were included for analysis. The mean patient age was 57.1 years and the mean number of ADRs per patient was 9.1. ADRs were reported frequently with amino acids solutions (682 events, 40.8%), followed by combinations products (519 events, 31.1%), and fat emulsions (363 events, 21.7%). The frequent ADRs were gastrointestinal (507 events, 30.3%), skin (343 events, 20.5%), general disorders (239 events, 14.3%), and central/peripheral nervous system disorders (165 events, 9.9%). The common clinical symptoms were nausea (321 events, 19.2%), vomiting (105 events, 6.3%), and vein pain (102 events, 6.1%). Serious ADRs accounted for 220 patients (9.4%) and dyspnea was the most frequent clinical manifestation.
Conclusion:
This study analyzed the KAERS data in 2015 from patients treated with PN and revealed gastrointestinal and skin disorders to be the leading ADRs.
-
Citations
Citations to this article as recorded by- Health State Utility Associated with Parenteral Nutrition Requirement in Patients with Short Bowel Syndrome and Intestinal Failure in Korea: A Vignette-Based Approach
Hyewon Sim, Jin Soo Moon, Young Suk Park, Eunji Heo, Yoon Soo Chun, Songhwa Choi, Hyemin Ku, Jae Hee Chung
Nutrients.2025; 17(22): 3551. CrossRef
- Health State Utility Associated with Parenteral Nutrition Requirement in Patients with Short Bowel Syndrome and Intestinal Failure in Korea: A Vignette-Based Approach
- 1,641 View
- 5 Download
- 1 Crossref
- Enteral Nutrition Support in Coronary Care Unit Patients Receiving Extraocorporeal Membrane Oxygenation: An Observational Case Study
- Sung Hye Kim, Yoonjin Shin, Mi Yong Rha, Young Yun Cho, Jeong Hoon Yang, Yang-Hyun Cho, Ji Young Seo, Bori Kang, Yangha Kim
- J Clin Nutr 2016;8(3):77-83. Published online December 31, 2016
- DOI: https://doi.org/10.15747/jcn.2016.8.3.77
-
Abstract
PDF
Purpose:
Enteral feeding remains controversial in patients receiving extracorporeal membrane oxygenation (ECMO), particularly in those treated with a high-dose vasopressor. This study examined the safety and feasibility of enteral nutritional support for patients undergoing ECMO in a cardiac care unit (CCU).
Methods:
Adult patients admitted to the CCU undergoing ECMO from January 2014 to May 2015 were included. Patients with <48 hours of support, undergoing ECMO at another hospital, and inaccurate medical records were excluded.
Results:
Among the 14 patients undergoing ECMO in the CCU, 2 patients were diagnosed with malnutrition and the others were in the normal state in the initial assessment. On the other hand, they had the malnutrition risk factors (anorexia, weight loss, fluid retention, and hypermetabolic state). Thirteen patients received enteral nutrition and 1 patient had possible oral intake. The average initiation day of enteral nutrition was 2.0±1.6 days on ECMO. The mean duration of enteral nutrition was 5.2±4.9 days and the target goal was achieved within 3 days. There were no serious adverse effects for enteral nutrition but 3 patients had gastrointestinal problems (diarrhea and anorexia), and gastrointestinal bleeding occurred in 1 patient. In 1 case, enteral nutrition had to be stopped due to the prone position. Overall, 5 patients were cured, 3 patients recovered through heart transplantation, and 6 patients died.
Conclusion:
Most CCU patients receiving ECMO were well nourished but had the malnutrition risk factors in progress. These results suggest that enteral feeding might be safe and feasible in patients treated with ECMO but there were minor side effects.
-
Citations
Citations to this article as recorded by- Nutrition Support in Critically Ill Cancer Patient Receiving Extracorporeal Membrane Oxygenation: A Case Report
Ji-Yeon Kim, Gyung-Ah Wie, Kyoung-A Ryu, So-Young Kim
Clinical Nutrition Research.2023; 12(2): 91. CrossRef - Comparison of the nutritional indicators of critically Ill patients on extracorporeal membrane oxygen (ECMO)
Nah-Mee Shin, Suk Yeon Ha, Yoon Soo Cho
Journal of Nutrition and Health.2021; 54(5): 489. CrossRef
- Nutrition Support in Critically Ill Cancer Patient Receiving Extracorporeal Membrane Oxygenation: A Case Report
- 1,749 View
- 3 Download
- 2 Crossref
Review Article
- Postoperative Nutritional Support for Gastrectomized Patients
- Han Hong Lee
- Surg Metab Nutr 2016;7(2):25-28. Published online December 30, 2016
- DOI: https://doi.org/10.18858/smn.2016.7.2.25
-
Abstract
PDF
Nutritional deficiency after gastrectomy is caused by anatomical and physiologic changes in the stomach. In the case of patients with gastric cancer, nausea and loss of appetite due to cancer cachexia syndrome can affect nutritional status after gastrectomy. Prognostic nutritional index based on preoperative nutritional conditions is used for prediction of postoperative outcomes including long-term survival. Generally, enteral nutrition is more effective for post-gastrectomy conditions than parenteral nutrition. In addition, specialized enteral formulas such as immunonutrition (amino acids, ω-3 fatty acids and nucleotide) seem to have benefits for gastrectomy patients, although there is still insufficient evidence. Ghrelin is a next generation agent to stimulate appetite in patients that underwent gastrectomy.
- 1,121 View
- 2 Download
Original Article
- The Effects of Early Enteral Nutrition in Patients: A Role of Nutrition Support Team
- Kye Wol Park, Hee Ryoung Son, Ji Hoon Kim, Myoung Hee Kim, Eun Jin Choi
- J Clin Nutr 2016;8(2):66-70. Published online August 31, 2016
- DOI: https://doi.org/10.15747/jcn.2016.8.2.66
-
Abstract
PDF
Purpose:
The study examined the effects of early enteral nutrition on the patients’ length of stay in an intensive care unit (ICU), length of stay and mortality rate.
Methods:
A retrospective design was employed with a total of 461 patients (mean age=69.9±15.6 years; 253 males; 208 females). They were divided into two groups according to when they received enteral feeding: an “early enteral nutrition” (EEN) group of 148 patients (32.1%) who received enteral feeding within 48 hours of their arrival at the hospital and a “delayed enteral nutrition” (DEN) group of 313 patients (67.9%) who received enteral feeding at some point after 48 hours of their arrival at the hospital. The EEN group and control group were similar in terms of age, sex, body mass index, and underlying diseases.
Results:
The EEN group’s total length of stay in hospital was shorter (23.29±27.19 days) than that of the control group (36.74±32.24 days); the difference was significant (P<0.001). The EEN group also showed a shorter length of stay in the ICU (13.67±22.77 days) than the DEN group (17.46±21.02 days) and a lower mortality rate (17.6%) than the control group (18.8%), but these differences were not significant.
Conclusion:
The study found that early enteral nutrition treatment reduced total length of stay in hospital significantly. The findings suggest that early enteral nutrition treatment plays an important role in the patients’ recovery and prognosis.
-
Citations
Citations to this article as recorded by- Nutritional support for critically ill patients by the Korean Society for Parenteral and Enteral Nutrition — part I: a clinical practice guideline
Seung Hwan Lee, Jae Gil Lee, Min Kwan Kwon, Jiyeon Kim, Mina Kim, Jeongyun Park, Jee Young Lee, Ye Won Sung, Bomi Kim, Seong Eun Kim, Ji Yoon Cho, A Young Lim, In Gyu Kwon, Miyoung Choi
Annals of Clinical Nutrition and Metabolism.2024; 16(3): 89. CrossRef - The Status of Enteral Nutrition Formula Use by Dietitians in Hospitals Within Busan and Gyeongnam Area
Haejin Kang, Minji Woo, Eunju Park, Yoo Kyoung Park
Clinical Nutrition Research.2022; 11(1): 9. CrossRef - Physician Compliance with Nutrition Support Team Recommendations: Effects on the Outcome of Treatment for Critically Ill Patients
Hyon-Ju Yon, Eun-Suk Oh, Ji Young Jang, Ji Yun Jang, Hongjin Shim
Journal of Acute Care Surgery.2022; 12(1): 1. CrossRef - Health and Nutrition Status of Elderly People with Multimorbidity: A Korea National Health and Nutrition Examination Survey (2013~2015)
Na-Gyeong Oh, Jung-Sook Seo
Korean Journal of Community Nutrition.2020; 25(6): 502. CrossRef
- Nutritional support for critically ill patients by the Korean Society for Parenteral and Enteral Nutrition — part I: a clinical practice guideline
- 1,807 View
- 8 Download
- 4 Crossref
Review Article
- Sources and Formulation of Macro- and Micro-Nutrients in Enteral Nutrition Formula
- Suhee Kim
- J Clin Nutr 2016;8(2):45-50. Published online August 31, 2016
- DOI: https://doi.org/10.15747/jcn.2016.8.2.45
-
Abstract
PDF
Enteral feeding therapy has existed since ancient Egypt, but most of the major advances in enteral nutrient techniques and formulas have taken place during the 20th century through the development of sources and ingredients This review provides a historical account of enteral nutrition (EN), including the sources and formulation of macro-and micro-nutrients in the formula and how to manufacture them. The formulas were improved by the development of raw materials that are easier to digest and the next formula is expected to develop functionality using more raw materials, such as ω-3, amino acid, and more functional ingredients to heal the disease.
-
Citations
Citations to this article as recorded by- Production of BCAA Fortified Soybean Powder Hydrolysate Using Enzymes from Bacillus amyloliquefaciens and Its Application in Functional Protein Formula Foods
Hyo Min Jin, Ae Eun Im, Jeong-Yong Cho, Seung-Hee Nam
Journal of the Korean Society of Food Science and Nutrition.2023; 52(4): 383. CrossRef - Physicochemical and sensory properties of protein-fortified cookies according to the ratio of isolated soy protein to whey protein
Hye-Rin Park, Ga-Hyun Kim, Yeseul Na, Ji-Eun Oh, Mi-Sook Cho
Food Science and Biotechnology.2021; 30(5): 653. CrossRef - Use of Oral Nutritional Supplements for Patients with Diabetes
Mi Ra Kang
The Journal of Korean Diabetes.2017; 18(3): 181. CrossRef
- Production of BCAA Fortified Soybean Powder Hydrolysate Using Enzymes from Bacillus amyloliquefaciens and Its Application in Functional Protein Formula Foods
- 2,483 View
- 10 Download
- 3 Crossref
 First
First Prev
Prev

